- Cancer Health Disparities Among Racial and Ethnic Minority Populations
- Cancer Health Disparities Among Other Medically Underserved Populations
- Impact of COVID-19 on Cancer Health Disparities
- Factors that Drive Cancer Health Disparities
- Achieving Health Equity: A Vital Investment for the U.S. Public Health and Economy
The State of Cancer Health Disparities in 2022
In this section, you will learn:
- Cancer health disparities are adverse differences in cancer burden experienced by racial and ethnic minorities and other medically underserved populations that include those living in rural areas; individuals from sexual and gender minorities; and those living in persistent poverty.
- In recent decades, overall cancer incidence and mortality rates have declined for all racial and ethnic minorities in the United States. The disparity in overall cancer mortality rates between Black people and White people has narrowed from 26 percent in 2000 to 13 percent in 2019.
- There is a growing recognition of the heterogeneity among individuals within each of the racial and ethnic minority groups, highlighting the need for disaggregated cancer data to develop effective strategies for achieving health equity.
- Research has identified complex factors, such as socioeconomic, cultural, social, and environmental factors, that influence each other to drive and perpetuate cancer health disparities.
- The economic burden of health disparities, including cancer health disparities, is enormous, as illustrated by an estimated loss of $3.2 billion in earnings in 2015 because of disparities in premature cancer deaths between Black and White individuals.
Section Contents
Breakthrough discoveries and technological innovations that bring lifesaving anticancer treatments to the clinic have resulted in unprecedented progress against cancer in recent decades. The age-adjusted overall U.S. cancer death rate has declined by 32 percent from 1991 to 2019 (1)Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer Statistics, 2022. CA: A Cancer Journal for Clinicians 2022;72:7-33. [LINK NOT AVAILABLE], due to major advances in prevention, early detection, and treatment including treatment of aggressive tumors, such as lung cancer and melanoma. During the same period, the number of cancer survivors living in the U.S. has more than doubled from 7.2 million in 1992 to 16.9 million in 2019 (2)American Association for Cancer Research. Aacr Cancer Progress Report. [updated October 13, 2021, cited 2022 April 22]..
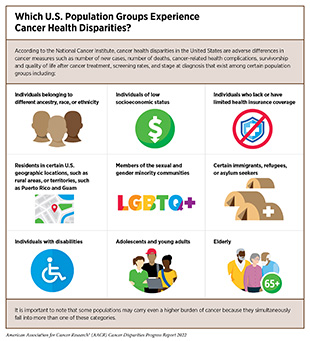
Despite the significant overall progress, cancer continues to pose a major public health challenge, and certain segments of the U.S. population continue to experience a disproportionate burden of cancer (see sidebar on Which U.S. Population Groups Experience Cancer Health Disparities?). A long history of racism has resulted in discriminatory policies, systemic inequities, and structural barriers that cause and perpetuate many of these health disparities (see Factors That Drive Cancer Health Disparities).
The exact measures of cancer burden when discussing health disparities often vary. Throughout this report, we use the NCI definition of cancer health disparities, i.e., adverse differences between certain population groups in cancer measures that include: number of new cases; number of deaths; cancer-related health complications; survivorship and quality of life after cancer treatment; screening rates; and stage at diagnosis. These population groups may be characterized by race, ethnicity, disability, gender and sexual identity, geographic location, income, education, and other characteristics (see sidebar on Which U.S. Population Groups Experience Cancer Health Disparities?) (3)Cancer Health Disparities Definitions and Examples – National Cancer Institute. [updated February 17, 2015, cited 2022 April 22]..
The AACR Cancer Disparities Progress Report 2022 aims to increase awareness of the progress in understanding and addressing disparities across the cancer care continuum , and to emphasize the vital importance of cancer health disparities research in saving lives. The report underscores the need for robust, sustained, and predictable annual federal funding increases for the entities that fuel progress against cancer health disparities, in particular, NIH, NCI, and CDC.
In this opening chapter, we provide an overview of the current state of disparities experienced by certain U.S. population groups in cancer incidence rates (i.e., the number of new individuals diagnosed with cancer per 100,000 people) and cancer death rates (i.e., the number of individuals who die from cancer per 100,000 people). We discuss the multifactorial, deeply rooted, and interconnected causes of cancer health disparities. The chapter concludes with the far-reaching and multifaceted adverse impacts of continued cancer health disparities on U.S. health and economy, and how addressing cancer health disparities through research funding can catalyze equitable access to health care.
Cancer Health Disparities Among Racial and Ethnic Minority Populations
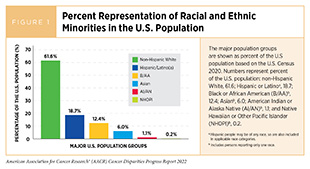
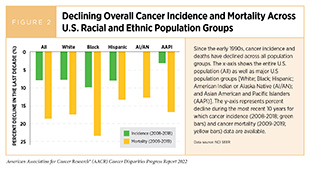
According to the 2020 Census, racial and ethnic minorities (see sidebar on U.S. Racial and Ethnic Population Groups) comprise nearly 40 percent of the U.S. population (Figure 1). It is encouraging that both the overall cancer incidence and cancer mortality—two key measures of cancer burden—have been steadily decreasing among all racial and ethnic minorities in the U.S. in recent decades (Figure 2). In some instances, the disparity in cancer incidence and mortality is narrowing between White populations and certain racial and ethnic minorities. For example, overall cancer incidence rates between 2013 and 2018 decreased the most among Black individuals compared to White individuals (eight percent versus five percent decline, respectively) (4)Kaiser Family Foundation. Racial Disparities in Cancer Outcomes, Screening, and Treatment. [updated February 3, 2022, cited 2022 April 22]..
Despite some promising trends, disparities across the cancer control continuum remain, and in some cases, continue to widen, as discussed throughout this report. As an example, although Black people experienced the largest decrease in cancer mortality rates between 2013 and 2018, cancer death rates were still the highest in this population group in 2018 (4)Kaiser Family Foundation. Racial Disparities in Cancer Outcomes, Screening, and Treatment. [updated February 3, 2022, cited 2022 April 22].. Furthermore, the burden of cancer among various racial and ethnic minorities varies substantially by cancer type as discussed in sections below.
It is also important to note that the latest years for which much of the cancer incidence and mortality data are presented in this report precede the onset of the COVID-19 pandemic. Thus, discussions and descriptions of cancer burden among racial and ethnic minorities in this report do not reflect the impact of COVID-19, which according to experts has worsened health disparities. For instance, because the adverse effects of COVID-19 were disproportionately higher among Black and Hispanic populations (7)American Association for Cancer Research. Aacr Report on the Impact of COVID-19 on Cancer Research and Patient Care. [updated February 10, 2022, cited 2022 April 22]., there is a greater possibility that individuals from these communities will experience additional delays in resuming routine cancer screening. It is therefore likely that the adverse impact of COVID-19 on disparities in the stage at which cancer is diagnosed, as well as the health outcomes for patients with cancer, will continue to evolve over the next several years.
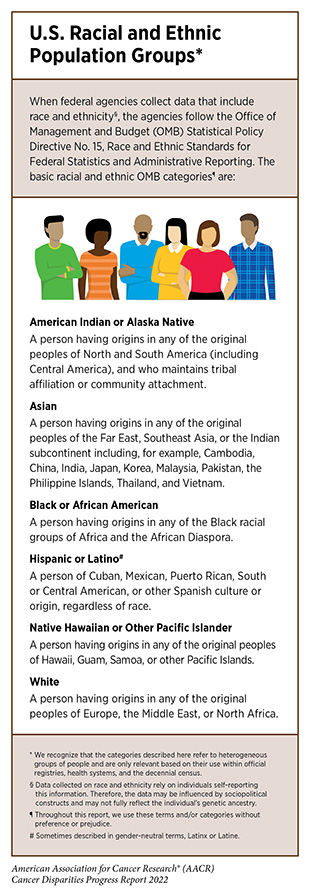
American Indian or Alaska Native (AI/AN) Population
According to the Census 2020, an estimated 9.7 million people identified as American Indian or Alaska Native (AI/AN)—alone or in combination with another race—accounting for 2.9 percent of the U.S. population (8)United States Census Bureau. Quickfacts United States. [updated July 1, 2021, cited 2022 April 22].. The AI/AN population is incredibly diverse, with 574 federally recognized tribes and more than 200 that remain unrecognized, encompassing many distinct customs, languages, and histories. It is important to note that the AI/AN population has the highest racial misclassification in health data of any racial or ethnic group in the U.S., likely contributing to an underestimation of the burden of cancer in the group (9)Jim MA, Arias E, Seneca DS, Hoopes MJ, Jim CC, Johnson NJ, et al. Racial Misclassification of American Indians and Alaska Natives by Indian Health Service Contract Health Service Delivery Area. American Journal of Public Health 2014;104:S295-S302. [LINK NOT AVAILABLE].
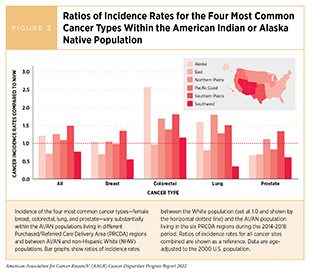
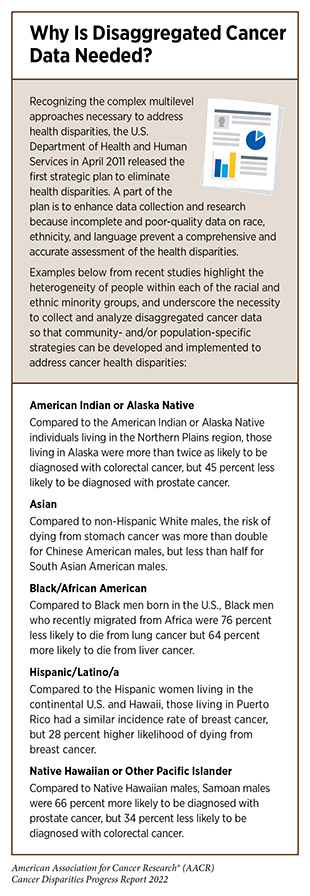
Compared to White people, AI/AN people had higher incidence rates during 2014-2018 for lung, colorectal, and kidney cancers, as well as liver, stomach, and cervical cancers that are caused by infectious agents (Figure 3). Furthermore, AI/AN populations living in different Purchased/Referred Care Delivery Area (PRCDA) regions has substantially different cancer risk and disparities compared to each other and to the White population. When compared to the White population, the incidence rate for all cancers combined is 23 percent lower in the AI/AN population living in the Southwest but 49 percent higher in those living in the Southern Plains (1)Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer Statistics, 2022. CA: A Cancer Journal for Clinicians 2022;72:7-33. [LINK NOT AVAILABLE]). Similar patterns extend to individual cancer types. As one example, AI/AN individuals living in the Northern Plains PRCDA region have five times higher incidence of lung cancer—the most diagnosed cancer in the AI/AN population—than those living in the Southwest PRCDA region (1)Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer Statistics, 2022. CA: A Cancer Journal for Clinicians 2022;72:7-33. [LINK NOT AVAILABLE]. When compared to White individuals, the lung cancer incidence is 80 percent higher among AI/AN individuals living in the Northern Plains, but 64 percent lower in those living in the Southwest (1)Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer Statistics, 2022. CA: A Cancer Journal for Clinicians 2022;72:7-33. [LINK NOT AVAILABLE].
An example of the burden of cancer for the AI/AN population is the disparity in kidney cancer. Compared to the White population, kidney cancer incidence rates are about 80 percent higher in the AI/AN population across all PRCDA regions except for the East region (1)Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer Statistics, 2022. CA: A Cancer Journal for Clinicians 2022;72:7-33. [LINK NOT AVAILABLE]. Alarmingly, these rates have been rapidly increasing in the AI/AN population over the last two decades (2.8 percent annual increase from 2009 to 2018) compared to the White population (1.1 percent increase during the same time) (10)National Cancer Institute. Surveillance, Epidemiology, and End Results Program. [updated January 8, 2022, cited 2022 April 22].. In addition to smoking, another reason for a higher incidence of kidney cancer is the higher rates of type 2 diabetes among AI/AN people (11)U.S. Department of Health and Human Services Office of Minority Health. Diabetes and American Indians/Alaska Natives the Office of Minority Health. [updated April 22, 2022, cited 2022 April 22]., which increases kidney cancer risk (12)Tseng C-H. Type 2 Diabetes Mellitus and Kidney Cancer Risk: A Retrospective Cohort Analysis of the National Health Insurance. PLOS ONE 2015;10:e0142480. [LINK NOT AVAILABLE]. During 2014-2019, the most recent period for which such data are available, AI/AN men and women had 75 percent and 64 percent higher death rates from kidney cancer compared to White men and women, respectively (13)Islami F, Guerra CE, Minihan A, Yabroff KR, Fedewa SA, Sloan K, et al. American Cancer Society’s Report on the Status of Cancer Disparities in the United States, 2021. CA Cancer J Clin 2022;72:112-43. [LINK NOT AVAILABLE]. This disparity is likely attributed also to poor access to quality health care.
Liver cancer represents another example of notable disparities in the burden of cancer between AI/AN and White populations. AI/ AN people have the highest liver cancer incidence of any major racial or ethnic group in the U.S. (1)Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer Statistics, 2022. CA: A Cancer Journal for Clinicians 2022;72:7-33. [LINK NOT AVAILABLE]. Both the liver cancer incidence (most recent 5-year data time period: 2014-2018) and mortality (most recent 5-year data time period: 2015-2019) were nearly double in the AI/AN population compared to White individuals (10)National Cancer Institute. Surveillance, Epidemiology, and End Results Program. [updated January 8, 2022, cited 2022 April 22].. This is likely due in large part to higher prevalence of risk factors in the AI/AN population, such as chronic hepatitis C virus (HCV) infection, obesity, diabetes, and cigarette smoking (1)Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer Statistics, 2022. CA: A Cancer Journal for Clinicians 2022;72:7-33. [LINK NOT AVAILABLE].
Examples presented in this section underscore the heterogeneity of the AI/AN population, which indicate differences in exposures to risk factors as well as access to health care in different PRCDA regions (see sidebar on Why Is Disaggregated Cancer Data Needed?). This highlights the importance of understanding region-specific needs and developing and implementing region-appropriate strategies to eliminate cancer health disparities in the AI/AN population.
Asian Population
The Asian population constitutes the fastest-growing racial group in the United States. In the 2020 U.S. Census, the Asian American population accounted for six percent of the U.S. population, a 35.5 percent increase since the 2010 Census (19)2020 Census Illuminates Racial and Ethnic Composition of the Country. [updated August 12, 2021, cited 2022 April 22].. With ancestry in numerous countries of origin, remarkable heterogeneity exists within the Asian population. The five largest groups constituting the Asian American designation are Chinese, South Asian, Filipino, Vietnamese, Korean, and Japanese. Differences in culture, nativity, migration history, and socioeconomic and behavioral factors impact the overall health as well as cancer-specific risk factors within these groups.
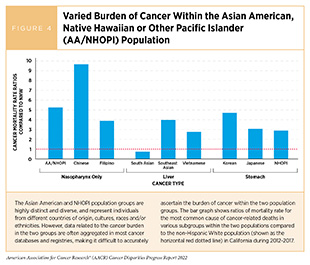
Compared to individuals from any other racial or ethnic groups, Asian individuals have the lowest rate of developing any type of cancer (20)U.S. Department of Health and Human Services Office of Minority Health. Cancer and Asian Americans – the Office of Minority Health. [updated August 26, 2021, cited 2022 April 22].. However, cancer is the leading cause of death for the Asian population in the United States (21)Chen MS, Lee RJ, Madan RA, Ta Park V, Shinagawa SM, et al. Charting a Path Towards Asian American Cancer Health Equity: A Way Forward. J Natl Cancer Inst. 2022;djac055. [LINK NOT AVAILABLE]. Asian people are disproportionately impacted by cancers that are caused by infectious agents (18)Torre LA, Sauer AM, Chen MS, Jr., Kagawa-Singer M, Jemal A, Siegel RL. Cancer Statistics for Asian Americans, Native Hawaiians, and Pacific Islanders, 2016: Converging Incidence in Males and Females. CA Cancer J Clin 2016;66:182-202. [LINK NOT AVAILABLE]. As one example, the higher burden of liver cancer due to chronic hepatitis B virus (HBV) infection among Asian individuals can be attributed to high HBV prevalence in the country of origin (22)Wong RJ, Brosgart CL, Welch S, Block T, Chen M, Cohen C, et al. An Updated Assessment of Chronic Hepatitis B Prevalence among Foreign-Born Persons Living in the United States. Hepatology 2021;74:607-26. [LINK NOT AVAILABLE]. However, liver cancer mortality varies greatly within the Asian population. A recent study examined nationwide death records of Americans from the years 2003 to 2017 and found that Vietnamese Americans were nearly three times more likely to die from liver cancer compared to non-Hispanic White (NHW) Americans; the likelihood of death from liver cancer was 35 percent less among Indian Americans compared to NHW Americans (23)Huang RJ, Sharp N, Talamoa R, Kapphahn K, Sathye V, Lin B, et al. Disaggregated Mortality from Gastrointestinal Cancers in Asian Americans: Analysis of United States Death Records. International journal of cancer 2021;148:2954-63. [LINK NOT AVAILABLE]. Similar variations in the burden among Asian Americans exist for cervical (caused by HPV), nasopharyngeal [caused by Epstein‐Barr virus (EBV)], and stomach (caused by Helicobacter pylori) cancers (Figure 4)(24)Lee RJ, Madan RA, Kim J, Posadas EM, Yu EY. Disparities in Cancer Care and the Asian American Population. Oncologist 2021;26:453-60. [LINK NOT AVAILABLE].
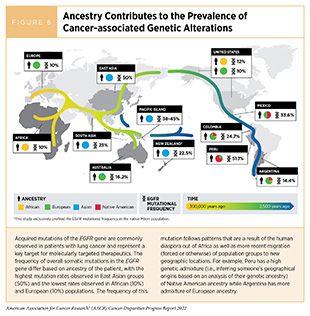
Of the cancer types common in the overall U.S. population, lung cancer is the leading cause of cancer-related deaths in the Asian population (18)Torre LA, Sauer AM, Chen MS, Jr., Kagawa-Singer M, Jemal A, Siegel RL. Cancer Statistics for Asian Americans, Native Hawaiians, and Pacific Islanders, 2016: Converging Incidence in Males and Females. CA Cancer J Clin 2016;66:182-202. [LINK NOT AVAILABLE]. Furthermore, Asian individuals, particularly women without a history of smoking, have a uniquely high burden of lung cancer among never-smokers (25)DeRouen MC, Canchola AJ, Thompson CA, Jin A, Nie S, Wong C, et al. Incidence of Lung Cancer among Never-Smoking Asian American, Native Hawaiian, and Pacific Islander Females. J Natl Cancer Inst 2022;114:78-86. [LINK NOT AVAILABLE]. Notably, more than 30 percent of lung cancer patients in Asia, including more than half of female patients with lung cancer, are never‐smokers. This observation has been attributed to a markedly increased rate of epidermal growth factor receptor (EGFR)–mutant lung cancer in Asian female nonsmokers (Figure 6) (26)Ha SY, Choi SJ, Cho JH, Choi HJ, Lee J, Jung K, et al. Lung Cancer in Never-Smoker Asian Females Is Driven by Oncogenic Mutations, Most Often Involving Egfr. Oncotarget 2015;6:5465-74. [LINK NOT AVAILABLE].
While smoking cessation remains key to reducing the overall lung cancer incidence and mortality, this example underscores the importance of understanding the disease in broader contexts of biology and country of origin, among other factors, to develop effective and population-specific interventions for eliminating cancer health disparities.
It is becoming evident that the aggregated reporting of cancer statistics for the Asian population results in underestimating the overall cancer burden as well as that of specific cancer types for specific subgroups within the Asian population—as it does for other racial and ethnic minorities (see sidebar on Why Is Disaggregated Cancer Data Needed?). Furthermore, it has been demonstrated that inaccuracies and deficiencies in data collection on cancer deaths for Asian individuals result in a misleading inflation of survival statistics for this population (27)Pinheiro PS, Morris CR, Liu L, Bungum TJ, Altekruse SF. The Impact of Follow-up Type and Missed Deaths on Population-Based Cancer Survival Studies for Hispanics and Asians. JNCI Monographs 2014;2014:210-7. [LINK NOT AVAILABLE]. Because of the heterogeneity of the Asian population, cancer researchers have been advocating for collection of disaggregated cancer data to accurately reflect the burden of cancer in this population and devise tailored strategies to close the disparities gap (21)Chen MS, Lee RJ, Madan RA, Ta Park V, Shinagawa SM, et al. Charting a Path Towards Asian American Cancer Health Equity: A Way Forward. J Natl Cancer Inst. 2022;djac055. [LINK NOT AVAILABLE](28)Chen MS, Jr. Cancer Health Disparities among Asian Americans: What We Do and What We Need to Do. Cancer 2005;104:2895-902. [LINK NOT AVAILABLE].
Black or African American Population
In 2020, nearly 47 million African American or Black individuals—including those who identified as African American or Black in combination with at least one additional race—were living in the U.S., constituting the third largest racial/ethnic population group (8)United States Census Bureau. Quickfacts United States. [updated July 1, 2021, cited 2022 April 22].. Recent estimates indicate that 111,990 new cancer diagnoses and 36,340 cancer deaths are expected in Black men in 2022. These projections are slightly higher—112,090 new cancer diagnoses and 37,250 cancer deaths—for Black women (1)Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer Statistics, 2022. CA: A Cancer Journal for Clinicians 2022;72:7-33. [LINK NOT AVAILABLE]. Prostate cancer is the most common cancer type in Black men and accounts for 37 percent of all new cancer diagnoses, while breast cancer is the most commonly diagnosed cancer in Black women and accounts for 32 percent of all new cancer diagnoses. Lung and colorectal cancers are the second (11-12 percent) and third (nine percent) most commonly diagnosed cancer types, respectively, in both Black men and Black women. The four cancer types are also the deadliest among the Black population and account for half of all cancer deaths in Black men and 44 percent of all cancer deaths in Black women (1)Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer Statistics, 2022. CA: A Cancer Journal for Clinicians 2022;72:7-33. [LINK NOT AVAILABLE].
The Black population in the U.S. experienced the largest decline in cancer incidence and mortality between 2013 and 2018 compared to any other racial population group (4)Kaiser Family Foundation. Racial Disparities in Cancer Outcomes, Screening, and Treatment. [updated February 3, 2022, cited 2022 April 22].. Despite recent progress toward reducing disparities in the burden of cancer, Black individuals continue to experience a disproportionate burden of cancer. Compared to White men, cancer incidence in Black men is six percent higher and cancer mortality is 19 percent higher. This disparity is even more notable in Black women who have eight percent lower cancer incidence than White women, but 12 percent higher cancer mortality (1)Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer Statistics, 2022. CA: A Cancer Journal for Clinicians 2022;72:7-33. [LINK NOT AVAILABLE]. Among the specific cancer types, stomach and prostate cancers and multiple myeloma show the largest racial disparities in incidence and mortality, with death rates more than two-fold higher in Black people than in White people.
Breast cancer is the most common cancer among Black women, with an estimated 36,260 new cases expected to be diagnosed in 2022. During 2014-2018, the overall breast cancer incidence rate was slightly lower in Black women compared to White women (127 versus 132 per 100,000 cases, respectively). However, it is concerning that, among women who are younger than 40 years, the breast cancer incidence rates are higher among Black women compared to White women. Furthermore, there are key differences in distribution of various breast cancer subtypes between Black and White women. For example, Black women are twice as likely as women of other racial and ethnic groups to be diagnosed with triple-negative breast cancer (TNBC) and 41 percent more likely to be diagnosed with inflammatory breast cancer, two aggressive subtypes of breast cancer (29)Stringer-Reasor EM, Elkhanany A, Khoury K, Simon MA, Newman LA. Disparities in Breast Cancer Associated with African American Identity. Am Soc Clin Oncol Educ Book 2021;41:e29-e46. [LINK NOT AVAILABLE]. Reasons for these differences are not yet clear. Unfortunately, these disparities in incidence are reflected in breast cancer mortality rates: Black women are 40 percent more likely to die from breast cancer compared to White women, despite a slightly lower overall breast cancer incidence rate (1)Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer Statistics, 2022. CA: A Cancer Journal for Clinicians 2022;72:7-33. [LINK NOT AVAILABLE]. Research indicates that the higher breast cancer mortality rate in Black women is multifactorial in etiology, explained, in part, by cancer diagnosis at an advanced stage; higher prevalence of aggressive subtypes of the disease; and more limited access to treatment options (29)Stringer-Reasor EM, Elkhanany A, Khoury K, Simon MA, Newman LA. Disparities in Breast Cancer Associated with African American Identity. Am Soc Clin Oncol Educ Book 2021;41:e29-e46. [LINK NOT AVAILABLE]. Socioeconomic disadvantages that are more prevalent in the Black community significantly contribute to this disparity, but the increased risk for biologically aggressive tumor subtypes is likely explained by genetic factors as well.
Although rare in U.S., 2,710 new cases of invasive male breast cancer will be diagnosed, and 530 men will die from it in 2022 (13)Islami F, Guerra CE, Minihan A, Yabroff KR, Fedewa SA, Sloan K, et al. American Cancer Society’s Report on the Status of Cancer Disparities in the United States, 2021. CA Cancer J Clin 2022;72:112-43. [LINK NOT AVAILABLE]. Breast cancer has a higher prevalence among Black men, as experienced by Dr. Mathew Knowles. Overall, Black men have 44-52 percent higher risk of developing breast cancer compared to White men (13)Islami F, Guerra CE, Minihan A, Yabroff KR, Fedewa SA, Sloan K, et al. American Cancer Society’s Report on the Status of Cancer Disparities in the United States, 2021. CA Cancer J Clin 2022;72:112-43. [LINK NOT AVAILABLE](30)Sung H, DeSantis C, Jemal A. Subtype-Specific Breast Cancer Incidence Rates in Black Versus White Men in the United States. JNCI Cancer Spectrum 2019;4(1):pkz091. [LINK NOT AVAILABLE]. Black men are also more than twice as likely as White men to develop highly aggressive forms of breast cancer, such as triple negative breast cancer (30)Sung H, DeSantis C, Jemal A. Subtype-Specific Breast Cancer Incidence Rates in Black Versus White Men in the United States. JNCI Cancer Spectrum 2019;4(1):pkz091. [LINK NOT AVAILABLE]. Well-known risk factors for male breast cancer include family history of breast and/or ovarian cancers, mutations in BRCA2 gene, radiation exposure, certain conditions that alter hormonal balance, and obesity, and diabetes (13)Islami F, Guerra CE, Minihan A, Yabroff KR, Fedewa SA, Sloan K, et al. American Cancer Society’s Report on the Status of Cancer Disparities in the United States, 2021. CA Cancer J Clin 2022;72:112-43. [LINK NOT AVAILABLE].
Prostate cancer is projected to account for 37 percent (or 41,600 cases) of all new cancer diagnoses in Black men in 2022, making it the most common cancer among Black men. The rate of prostate cancer incidence during 2014-2018 was 73 percent higher in Black men compared to White men, a disparity that has persisted for decades (1)Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer Statistics, 2022. CA: A Cancer Journal for Clinicians 2022;72:7-33. [LINK NOT AVAILABLE](10)National Cancer Institute. Surveillance, Epidemiology, and End Results Program. [updated January 8, 2022, cited 2022 April 22].. During 2015-2019, the most recent years for which such data are available, prostate cancer death rates declined every year by 1.3 percent for Black men compared to 0.7 percent for White men. This favorable trend indicates a narrowing of the disparity between the two populations, but much remains to be done. Black men continue to have the highest death rate for prostate cancer compared to any racial or ethnic group in the U.S.; during 2015-2019, Black men were twice as likely to die from prostate cancer compared to White men (1)Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer Statistics, 2022. CA: A Cancer Journal for Clinicians 2022;72:7-33. [LINK NOT AVAILABLE](10)National Cancer Institute. Surveillance, Epidemiology, and End Results Program. [updated January 8, 2022, cited 2022 April 22].. The reasons for disparities in the burden of prostate cancer among Black men are complex and multifactorial. Research has shown that biological factors (such as ancestry-related genetic differences) (31)McHugh J, Saunders EJ, Dadaev T, McGrowder E, Bancroft E, Kote-Jarai Z, et al. Prostate Cancer Risk in Men of Differing Genetic Ancestry and Approaches to Disease Screening and Management in These Groups. Br J Can 2021;126(10):1366-73. [LINK NOT AVAILABLE], as well as socioeconomic factors (such as lack of access to best available treatment options and/or suboptimal treatment for prostate cancer) contribute to the disparity in prostate cancer mortality among Black men (32)Dess RT, Hartman HE, Mahal BA, Soni PD, Jackson WC, Cooperberg MR, et al. Association of Black Race with Prostate Cancer–Specific and Other-Cause Mortality. JAMA Oncol 2019;5:975-83. [LINK NOT AVAILABLE](33)Cackowski FC, Mahal B, Heath EI, Carthon B. Evolution of Disparities in Prostate Cancer Treatment: Is This a New Normal? Am Soc Clin Oncol Educ Book 2021;41:1-12. [LINK NOT AVAILABLE]. Researchers are currently working on understanding the biological and genetic features of tumors that contribute to disparities in the burden of prostate cancer.
Lung cancer is the third most common cancer in Black people and will account for more than 11 percent of all new cancer diagnoses (25,690 cases) in the population group in 2022. Effective smoking cessation campaigns over the past five decades have resulted in a steady decline in the overall lung cancer incidence with a steeper decline among Black adults, greatly reducing the disparity in lung cancer incidence between Black and White populations (1)Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer Statistics, 2022. CA: A Cancer Journal for Clinicians 2022;72:7-33. [LINK NOT AVAILABLE].
Despite the narrowing disparities, lung cancer incidence rates in Black men were 12 percent higher than those in White men during 2014-2018 (1)Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer Statistics, 2022. CA: A Cancer Journal for Clinicians 2022;72:7-33. [LINK NOT AVAILABLE]. Furthermore, an estimated 14,160 Black individuals are expected to die from lung cancer in 2022. Lung cancer is also the leading cause of cancer-related mortality in Black men and the second-leading cause of cancer deaths in Black women. Encouragingly, the lung cancer-related mortality has declined at a faster pace in Black individuals than in White individuals over the past two decades. During 2015-2019, the most recent period for which such data are available, the lung cancer death rate declined by about six percent every year in Black men compared to five percent in White men, and four percent in Black and White women. These trends reflect a steep decline in smoking rates over the past five decades, thanks to effective public health policies (see Regulations to Reduce the Disparate Harms of Tobacco Products (2)American Association for Cancer Research. Aacr Cancer Progress Report. [updated October 13, 2021, cited 2022 April 22]..
An estimated 20,700 Black individuals are expected to be diagnosed with colorectal cancer in 2022, making it the fourth most common cancer in the Black population. During 2014-2018, Black people had the highest incidence of colorectal cancer in the U.S. compared to any other racial or ethnic minority group, and the incidence was nearly 15 percent higher compared to White people (10)National Cancer Institute. Surveillance, Epidemiology, and End Results Program. [updated January 8, 2022, cited 2022 April 22].. Historically, colorectal cancer was more common in White populations until the early 1990s, when the colorectal cancer incidence became higher in Black populations due to an increase in the associated risk factors as well as lower screening rates for colorectal cancer (1)Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer Statistics, 2022. CA: A Cancer Journal for Clinicians 2022;72:7-33. [LINK NOT AVAILABLE](34)Rutter CM, Knudsen AB, Lin JS, Bouskill KE. Black and White Differences in Colorectal Cancer Screening and Screening Outcomes: A Narrative Review. Cancer Epidemiol Biomarkers Prev 2021;30:3-12. [LINK NOT AVAILABLE]. Even though the incidence rates are declining at a faster pace among the overall Black population compared to the overall White population (three versus two percent annual decline from 2009 to 2018, respectively), it is concerning that among individuals who are younger than 50 years of age the yearly decline for the same period was four times lower in Black people compared to White people (1)Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer Statistics, 2022. CA: A Cancer Journal for Clinicians 2022;72:7-33. [LINK NOT AVAILABLE]. Furthermore, there is a major disparity between Black and White populations in mortality rates for colorectal cancer, which are 44 and 31 percent higher in Black men and women, respectively, compared to White men and women (1)Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer Statistics, 2022. CA: A Cancer Journal for Clinicians 2022;72:7-33. [LINK NOT AVAILABLE]. Research indicates that many biological and socioeconomic factors contribute to disparities in colorectal cancer mortality for Black people, such as: obesity, malnutrition, and physical inactivity (see Disparities in the Burden of Preventable Cancer Risk Factors; lower rates of screening for early detection (see Disparities in Cancer Screening for Early Detection); and lower stage-specific survival (34)Rutter CM, Knudsen AB, Lin JS, Bouskill KE. Black and White Differences in Colorectal Cancer Screening and Screening Outcomes: A Narrative Review. Cancer Epidemiol Biomarkers Prev 2021;30:3-12. [LINK NOT AVAILABLE](35)Holowatyj AN, Ruterbusch JJ, Rozek LS, Cote ML, Stoffel EM. Racial/Ethnic Disparities in Survival among Patients with Young-Onset Colorectal Cancer. J Clin Oncol 2016;34:2148-56. [LINK NOT AVAILABLE].
Another cancer type with a significant racial disparity for Black people is multiple myeloma. In 2022, an estimated 7,810 new myeloma cases and 2,530 myeloma deaths are expected among Black individuals (1)Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer Statistics, 2022. CA: A Cancer Journal for Clinicians 2022;72:7-33. [LINK NOT AVAILABLE]. Death rates for myeloma declined by three percent every year for Black women and one percent for Black men and White men during 2015-2019 (1)Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer Statistics, 2022. CA: A Cancer Journal for Clinicians 2022;72:7-33. [LINK NOT AVAILABLE], thanks to rapid advancements in effective therapeutics. However, both the incidence and mortality rates for myeloma in Black people remain at least twice as high as in White people, in part, due to disparities in access to quality health care and newer treatment options. From 2009 to 2018, there was also a concerning two percent yearly increase in the incidence of myeloma in Black women (1)Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer Statistics, 2022. CA: A Cancer Journal for Clinicians 2022;72:7-33. [LINK NOT AVAILABLE]. Reasons for an increase in multiple myeloma incidence among Black women are multifactorial and may include higher rates of obesity (36)Sonderman JS, Bethea TN, Kitahara CM, Patel AV, Harvey C, Knutsen SF, et al. Multiple Myeloma Mortality in Relation to Obesity among African Americans. JNCI: Journal of the National Cancer Institute 2016;(10):djw120. [LINK NOT AVAILABLE]; and a potential increase in the incidence of monoclonal gammopathy of undetermined significance, a blood condition that can progress to multiple myeloma (37)Landgren O, Kyle RA, Pfeiffer RM, Katzmann JA, Caporaso NE, Hayes RB, et al. Monoclonal Gammopathy of Undetermined Significance (Mgus) Consistently Precedes Multiple Myeloma: A Prospective Study. Blood 2009;113:5412-7. [LINK NOT AVAILABLE](38)Schinasi LH, Brown EE, Camp NJ, Wang SS, Hofmann JN, Chiu BC, et al. Multiple Myeloma and Family History of Lymphohaematopoietic Cancers: Results from the International Multiple Myeloma Consortium. Br J Haematol 2016;175:87-101. [LINK NOT AVAILABLE], among other factors.
The U.S. Black population is heterogeneous and includes Black individuals who were either born in the U.S. or emigrated to the U.S. and trace their ancestry to any of the Black racial groups of Africa and the African Diaspora (see sidebar on U.S. Racial and Ethnic Population Groups). It is important to underscore this heterogeneity because the burden of cancer varies substantially within the population subgroups (see sidebar on Why Is Disaggregated Cancer Data Needed?). A recent study found large variations in age-adjusted cancer incidence rates across non-Hispanic Black (NHB) subgroups (39)Llanos AAM, Li J, Tsui J, Gibbons J, Pawlish K, Nwodili F, et al. Variation in Cancer Incidence Rates among Non-Hispanic Black Individuals Disaggregated by Nativity and Birthplace, 20052017: A Population-Based Cancer Registry Analysis. Frontiers in Oncology 2022;12:857548. [LINK NOT AVAILABLE]. For example, age-adjusted cancer incidence was >32 percent lower among NHB individuals born outside the U.S. compared to those born in the U.S. Furthermore, females born in Jamaica and other Caribbean islands had lower rates of cancer incidence (114.6 and 128.8 per 100,000, respectively) than those born in Africa and Haiti (139.4 and 149.9 per 100,000, respectively). No significant differences in age-adjusted cancer incidence were observed by birthplace among the immigrant NHB males.
Hispanic or Latino(a) Population
The Hispanic population—one of the fastest growing ethnic groups in the U.S.— accounted for 18 percent of the total U.S. population in the 2020 U.S. consensus (Figure 1). It is a diverse community of individuals from many races, religions, languages, and cultural identities. It is important to note that, because most U.S. cancer data are reported in the aggregate, the descriptions of incidence and mortality rates in the population do not account for the important differences among the diverse subgroups within the Hispanic population. (see sidebar on Why Is Disaggregated Cancer Data Needed?). Furthermore, it has been demonstrated that inaccuracies and deficiencies in data collection on cancer deaths for Hispanic individuals results in a misleading inflation of survival statistics for this population (26)Ha SY, Choi SJ, Cho JH, Choi HJ, Lee J, Jung K, et al. Lung Cancer in Never-Smoker Asian Females Is Driven by Oncogenic Mutations, Most Often Involving Egfr. Oncotarget 2015;6:5465-74. [LINK NOT AVAILABLE].
Overall, Hispanic individuals are less likely to be diagnosed with cancer than NHW individuals, but have higher incidence of specific cancer types. In 2021, more than 1.7 million Hispanic individuals in the U.S. were diagnosed with cancer and nearly 50,000 died from the disease, making cancer the leading cause of death in this population group. Compared to the NHW population, the Hispanic population has lower rates of breast, colorectal, lung, and prostate cancers, but higher rates of gallbladder cancer as well as liver, stomach, and cervical cancers (1)Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer Statistics, 2022. CA: A Cancer Journal for Clinicians 2022;72:7-33. [LINK NOT AVAILABLE]. However, as in the overall U.S. population, prostate and breast cancers are the most common cancers in Hispanic men and women, respectively. In recent years, the reduction in the burden of cancer in the Hispanic population has closely followed the trends in the NHW population, i.e., 0.5 percent yearly decline in overall incidence for both populations during 2009-2018, and 1.2 percent and 1.6 percent yearly decrease in overall mortality during 2010-2019, respectively (10)National Cancer Institute. Surveillance, Epidemiology, and End Results Program. [updated January 8, 2022, cited 2022 April 22]..
Because of the heterogeneity of the Hispanic population, the risk for different cancer types varies widely depending upon country or region of ancestral origin (e.g., Mexican Americans versus Cuban Americans); nativity (e.g., U.S.-born versus foreign-born); and ancestral race (e.g., Indigenous Americans, Europeans, and Africans) (1)Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer Statistics, 2022. CA: A Cancer Journal for Clinicians 2022;72:7-33. [LINK NOT AVAILABLE](40)Martinez Tyson D, Medina-Ramirez P, Flores AM, Siegel R, Aguado Loi C. Unpacking Hispanic Ethnicity—Cancer Mortality Differentials among Hispanic Subgroups in the United States, 2004–2014. Frontiers in Public Health 2018;6:219. [LINK NOT AVAILABLE]. As an example, the lung cancer incidence rates during 2014-2018 among Hispanic individuals in Puerto Rico were 44 percent lower than among Hispanic individuals in mainland U.S. (16.1 versus 29.0 per 100,000, respectively)(41)National Cancer Institute. State Cancer Profiles Puerto Rico. [updated April, 22 2022, cited 2022 April 22].(10)National Cancer Institute. Surveillance, Epidemiology, and End Results Program. [updated January 8, 2022, cited 2022 April 22].. In contrast, prostate cancer incidence rates among men in Puerto Rico were nearly 70 percent higher than among Hispanic men in mainland U.S. (144.3 versus 94.1 per 100,000, respectively) (1)Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer Statistics, 2022. CA: A Cancer Journal for Clinicians 2022;72:7-33. [LINK NOT AVAILABLE]. As another example, genetic ancestry studies have demonstrated that risk of breast cancer is lower in Hispanic women if more of their genetic makeup comes from a higher proportion of Indigenous American ancestry but increases if more of their genetic makeup comes from European ancestry (42)Zavala VA, Serrano-Gomez SJ, Dutil J, Fejerman L. Genetic Epidemiology of Breast Cancer in Latin America. Genes (Basel) 2019;10:153. [LINK NOT AVAILABLE].
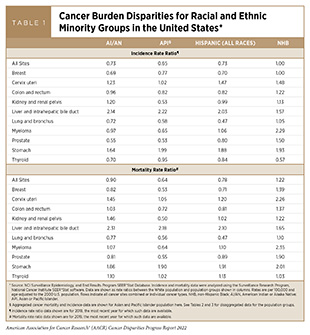
The three cancer types for which the Hispanic community shoulders a high burden of incidence and mortality compared to the NHW population are liver, stomach, and cervical cancers (Table 1) (1)Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer Statistics, 2022. CA: A Cancer Journal for Clinicians 2022;72:7-33. [LINK NOT AVAILABLE]. Hispanic men and women have nearly double the incidence and mortality rates for liver and stomach cancers compared to NHW men and women, while Hispanic women have an approximately 43 percent higher risk of cervical cancer incidence and 20 percent higher risk of death compared to NHW women (10)National Cancer Institute. Surveillance, Epidemiology, and End Results Program. [updated January 8, 2022, cited 2022 April 22].. More recently, Hispanic populations living in the mainland U.S. are also showing an increasing trend of liver cancer incidence and higher liver cancer mortality rates compared to NHW populations (43)Zavala VA, Bracci PM, Carethers JM, Carvajal-Carmona L, Coggins NB, Cruz-Correa MR, et al. Cancer Health Disparities in Racial/Ethnic Minorities in the United States. Br J Can 2021;124:315-32. [LINK NOT AVAILABLE]. Reasons of the disproportionate burden of these three cancer types in the Hispanic population are multifactorial but can be largely attributed to exposure to known risk factors, such as smoking, obesity, and pathogenic infections , all of which are highly prevalent within the Hispanic population subgroups (44)Centers for Disease Control and Prevention. Hispanics/Latinos and Tobacco Use. [updated March 22, 2022, cited 2022 April 22].(45)Centers for Disease Control and Prevention. Adult Obesity Facts. [updated November 12, 2021, cited 2022 April 22]..
Chronic infection with the bacterium, Helicobacter pylori—the strongest known risk factor for stomach cancer—remains high in Hispanic individuals compared to the NHW population (46)Tsang SH, Avilés-Santa ML, Abnet CC, Brito MO, Daviglus ML, Wassertheil-Smoller S, et al. Seroprevalence and Determinants of Helicobacter Pylori Infection in the Hispanic Community Health Study/Study of Latinos. Clinical Gastroenterology and Hepatology 2022;20:e438-e51. [LINK NOT AVAILABLE]. Chronic infection with HBV or HCV is the strongest risk factor for liver cancer and accounts for most liver cancer cases among Hispanic individuals in the United States (47)Pinheiro PS, Medina HN, Callahan KE, Jones PD, Brown CP, Altekruse SF, et al. The Association between Etiology of Hepatocellular Carcinoma and Race-Ethnicity in Florida. Liver International 2020;40:1201-10. [LINK NOT AVAILABLE]. Other contributing factors to rising incidence of liver cancer among Hispanic populations include obesity and fatty liver disease (43)Zavala VA, Bracci PM, Carethers JM, Carvajal-Carmona L, Coggins NB, Cruz-Correa MR, et al. Cancer Health Disparities in Racial/Ethnic Minorities in the United States. Br J Can 2021;124:315-32. [LINK NOT AVAILABLE]. Furthermore, Hispanic individuals from Mexico may also be exposed to aflatoxin—a carcinogen produced by a fungus that can grow in foods stored in moist, warm conditions—which is an important independent risk factor for liver cancer (48)Gomez-Quiroz LE, Roman S. Influence of Genetic and Environmental Risk Factors in the Development of Hepatocellular Carcinoma in Mexico. Annals of Hepatology 2022;27:100649. [LINK NOT AVAILABLE].
Cervical cancer is caused by persistent infection with certain strains of HPV. These carcinogenic strains of HPV have a higher prevalence among Hispanic women (1)Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer Statistics, 2022. CA: A Cancer Journal for Clinicians 2022;72:7-33. [LINK NOT AVAILABLE]. Other factors contributing to higher cervical cancer incidence and mortality in Hispanic women include structural barriers in access to screening as well as significantly lower HPV and HPV vaccine awareness and knowledge within the Hispanic population. According to a recent study, more than 50 percent of foreign-born U.S. Hispanic adults are unaware of HPV and the preventive vaccine (49)Escobar B, Amboree TL, Sonawane K, Deshmukh AA, McGee LU, Rodriguez AM, et al. Human Papillomavirus Awareness among Foreign- and US-Born Hispanics, United States, 2017-2018. Prev Med Rep 2021;22:101379. [LINK NOT AVAILABLE]. These examples not only highlight the heterogeneity of the Hispanic population, but also underscore the need for disaggregated cancer and risk prevalence data in heterogeneous ethnic minorities in the U.S. so that evidence-based and population-specific interventions and policies can be devised to reduce and ultimately eliminate cancer health disparities (see Policies to Address Disparities in Cancer Prevention).
Native Hawaiian or Other Pacific Islander (NHOPI) Population
The Native Hawaiian or Other Pacific Islander (NHOPI) racial group refers to individuals having origins in any of the original peoples of Hawaii and the six U.S.-associated Pacific Island jurisdictions: Guam; American Samoa; the Commonwealth of the Northern Mariana Islands; the Republic of the Marshall Islands; the Republic of Belau; and the Federated States of Micronesia. The NHOPI population is comprised of more than 25 diverse subgroups with distinct variations in historical backgrounds, languages, and cultural traditions and, according to the 2020 U.S. Census Bureau, makes up roughly 0.2 percent of the U.S. population (19)2020 Census Illuminates Racial and Ethnic Composition of the Country. [updated August 12, 2021, cited 2022 April 22]..
The overall cancer incidence in 2019 was 40 percent less in the NHOPI population compared to the NHW population (50)U.S. Department of Health and Human Services Office of Minority Health. Cancer and Native Hawaiians/Pacific Islanders. [updated July 29, 2021, cited 2022 April 22].. While many major registries aggregate cancer data from NHOPI and Asian American populations, the Hawaii Tumor Registry—funded by the NCI SEER—provides some cancer data for the state of Hawaii. According to its most recent Hawaii Cancer at a Glance 2012-2016 Report, the overall cancer mortality in the state was the highest in Native Hawaiians compared to the other major racial/ ethnic groups Chinese, Filipinos, Japanese, Whites, and Others (includes all other races and ethnicities). During 2012-2016, the most recent period for which such data are available, Native Hawaiian men had the lowest incidence of but the highest mortality from prostate cancer, while breast cancer incidence and mortality were highest among Native Hawaiian women compared to any other racial or ethnic group. Native Hawaiian women also had the highest mortality from multiple myeloma compared to any other racial or ethnic group in the state (51)University of Hawai’i Cancer Center. Hawai’i Cancer at a Glance 2012-2016. [updated 2018, cited 2022 April 22].. Although Hawaii had among the lowest rates of lung cancer in the United States in 2012-2016, lung cancer incidence was highest among Native Hawaiian men and women, and lung cancer mortality was highest in Native Hawaiian women compared to the other population groups in the state (51)University of Hawai’i Cancer Center. Hawai’i Cancer at a Glance 2012-2016. [updated 2018, cited 2022 April 22].. Another cancer type with the highest mortality rate among Native Hawaiian men is cancer of the liver and intrahepatic bile duct compared to men from other population groups in the state (51)University of Hawai’i Cancer Center. Hawai’i Cancer at a Glance 2012-2016. [updated 2018, cited 2022 April 22]..
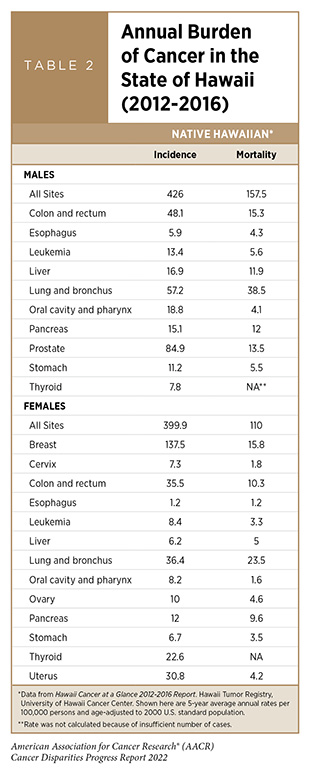
Cancer incidence and mortality data for the U.S.-affiliated Pacific Islands remain sparse. A recent report, which evaluated the cancer incidence and mortality data from the Pacific Regional Central Cancer Registry captured during 2008-2013, provides some insights into the burden of cancer among Pacific Islanders (52)Van Dyne EA, Saraiya M, White A, Novinson D, Senkomago V, Buenconsejo-Lum L. Cancer Mortality in the US-Affiliated Pacific Islands, 2008-2013. Hawaii J Health Soc Welf 2020;79:99-107. [LINK NOT AVAILABLE]. Incidence-based cancer mortality rates—a metric that allows calculation of mortality rates by stage at diagnosis, age at diagnosis and year of diagnosis—among males were highest in Palau (151 per 100,000) and lowest in American Samoa (22 per 100,000). Among females, rates were highest in the Republic of the Marshall Islands (120 per 100,000) and lowest in the Commonwealth of the Northern Mariana Islands (19 per 100,000) (Table 2) (52)Van Dyne EA, Saraiya M, White A, Novinson D, Senkomago V, Buenconsejo-Lum L. Cancer Mortality in the US-Affiliated Pacific Islands, 2008-2013. Hawaii J Health Soc Welf 2020;79:99-107. [LINK NOT AVAILABLE]. Overall, Pacific Islanders had the highest incidence-based mortality rates for cancer types (lung, liver, cervical, oral cavity, and pharynx) that are either preventable through reduction of risk factors, or can be detected through effective screening tests at an early stage when treatments are most effective (52)Van Dyne EA, Saraiya M, White A, Novinson D, Senkomago V, Buenconsejo-Lum L. Cancer Mortality in the US-Affiliated Pacific Islands, 2008-2013. Hawaii J Health Soc Welf 2020;79:99-107. [LINK NOT AVAILABLE]. Pacific Islanders also have a unique burden for certain cancer types. For example, women in the Republic of the Marshall Islands have eight times the U.S. incidence of invasive cervical cancer, making this the highest incidence of cervical cancer in the world (53)Pacific Regional Central Cancer Registry. Cancer in the US Affiliated Pacific Islands 2007-2015. [updated December 2019, cited 2022 April 22].. In addition, Pacific Islands were also the sites for nuclear bomb testing programs of many nations during the Cold War. Despite mixed evidence that radioactivity from the testing affected thyroid cancer rates among Pacific Islanders, the cultural context, perspectives, and fears related to radiation remain (54)Palafox NA, Riklon S, Alik W, Hixon AL. Health Consequences and Health Systems Response to the Pacific U.S. Nuclear Weapons Testing Program. Pac Health Dialog 2007;14:170-8. [LINK NOT AVAILABLE].
Because of its geographical location, racial and ethnic heterogeneity, and socioeconomic characteristics, the NHOPI population faces unique structural barriers to accessing quality health care, which can further exacerbate the disproportionate burden of certain types of cancer among the population. As evident from examples discussed throughout this section, disaggregated cancer data for the population group are sparse and not up to date with the mainland U.S. cancer data, underscoring the urgent need for collecting high-quality cancer data of the population so that effective and evidence-based strategies can be developed to address cancer health disparities in this population (see sidebar on Why Is Disaggregated Cancer Data Needed?).
Cancer Health Disparities Among Other Medically Underserved Populations
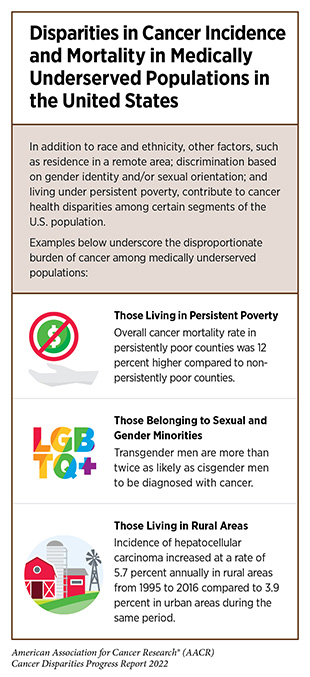
In addition to racial and ethnic minorities, many other segments of the U.S. population shoulder a disproportionate burden of cancer (see sidebar on Which U.S. Population Groups Experience Cancer Health Disparities?). These population groups are often racially and ethnically diverse, but are disadvantaged in their access to quality cancer care and may also have a higher prevalence of modifiable risk factors because of a myriad of factors including: residence in a remote area that lacks access to cutting-edge cancer treatments and/or state-of-the-art health care facilities (e.g., rural populations); gender and/or sexual orientation that may invoke implicit bias and discriminatory behavior (e.g., sexual and gender minorities); and persistent poverty that prevents a person from accessing the needed health care (e.g., low-income households) (see sidebar on Disparities in Cancer Incidence and Mortality in Medically Underserved Populations).
Populations Residing in Rural Areas
Rural and urban areas in the U.S. represent populations that are racially and ethnically diverse and have overlapping as well as distinct socioeconomic and sociodemographic patterns (58)Health Resources and Services Administration. Defining Rural Population. [updated October 2021, cited 2022 April 22].. Researchers and policy officials employ many definitions to distinguish rural from urban areas. NCI’s Division of Cancer Control and Population Sciences uses the United States Department of Agriculture (USDA) Economic Research Services’ 2013 Rural-Urban Continuum Codes to define rural areas. Based on this classification, an estimated 15 percent of the U.S. population and approximately 74 percent of the U.S. geographical areas are considered rural (59)U.S. Department of Agriculture. Rural-Urban Continuum Codes. [updated December 10, 2020, cited 2022 April 22]..
Rural counties have lower cancer incidence rates but higher death rates for all cancer sites combined compared to urban counties. It is of concern that differences in death rates between rural and urban areas are increasing over time (60)Henley SJ, Anderson RN, Thomas CC, Massetti GM, Peaker B, Richardson LC. Invasive Cancer Incidence, 2004-2013, and Deaths, 2006-2015, in Nonmetropolitan and Metropolitan Counties – United States. MMWR Surveill Summ 2017;66:1-13. [LINK NOT AVAILABLE]. Additionally, while a recent study shows that the cancer incidence rates are declining among both rural and urban populations, the rate of decline in urban areas between 1995 and 2013 was more than double that of rural areas (10.2 versus 4.8 percent, respectively) (61)Zahnd WE, James AS, Jenkins WD, Izadi SR, Fogleman AJ, Steward DE, et al. Rural-Urban Differences in Cancer Incidence and Trends in the United States. Cancer Epidemiol Biomarkers Prev 2018;27:1265-74. [LINK NOT AVAILABLE].
Evidence suggests that some cancers are more common in rural areas while others are more common in urban areas. Among the four most common cancers in the U.S., lung and colorectal cancers occur more often in rural populations (59)U.S. Department of Agriculture. Rural-Urban Continuum Codes. [updated December 10, 2020, cited 2022 April 22].. Notably, lung cancer incidence rates in rural areas declined at nearly one third the pace of urban counties during the 1995-2013 period (6.95 versus 18.4 percent, respectively) (61)Zahnd WE, James AS, Jenkins WD, Izadi SR, Fogleman AJ, Steward DE, et al. Rural-Urban Differences in Cancer Incidence and Trends in the United States. Cancer Epidemiol Biomarkers Prev 2018;27:1265-74. [LINK NOT AVAILABLE]. The slower decline in incidence rates of lung cancer in rural areas is mostly attributed to higher rates of tobacco use and lower rates of low-dose computed tomography (LDCT)—a screening exam for lung cancer (see Ways to Screen for Cancer). Elevated incidence of colorectal cancer rates is likely because of higher prevalence of obesity and lower adherence to screening. Conversely, breast cancer and prostate cancer incidence rates tend to be higher in urban areas, likely because of higher uptake in breast cancer screening (62)Tran L, Tran P. US Urban–Rural Disparities in Breast Cancer-Screening Practices at the National, Regional, and State Level, 2012–2016. Cancer Causes & Control 2019;30:1045-55. [LINK NOT AVAILABLE] and better access to quality health care.
Compared to those living in urban areas, individuals living in rural areas have 17 percent higher death rates from all cancers combined, areas, although disparities in deaths from prostate and breast cancers have narrowed substantially in recent years (63)Centers for Disease Control and Prevention. An Update on Cancer Deaths in the United States. [updated February 28, 2022, cited 2022 April 22].. However, disparities in death rates for lung and colorectal cancers remain large, with 34 and 23 percent higher death rates in rural residents, respectively (63)Centers for Disease Control and Prevention. An Update on Cancer Deaths in the United States. [updated February 28, 2022, cited 2022 April 22].. Evidence suggests that progress in reducing cancer death rates for all cancers combined and for most common cancers has been slower in rural than in urban areas, further widening the disparities in mortality.

Reasons for rural-urban disparities are multidimensional. Compared to those living in urban areas, rural residents face many disadvantages that place them at an increased risk of cancer such as: restricted means to enhance socioeconomic status; higher exposure to certain cancer risk factors; and limited access to quality health care. Rural communities also tend to have limited access to high-speed Internet resources, a phenomenon known as the “digital divide.” In the wake of the COVID-19 pandemic, the cancer care community has become even more reliant upon electronic health and telemedicine (see sidebar on What Is Telemedicine?), thus making the digital divide yet another cause for cancer disparities associated with rural residence. Cancer health disparities are further exacerbated, in part, by the lack of health insurance among some rural residents and shortages of primary care physicians, oncologists, and other cancer care specialists, as well as by limited access to state-of-the-art medical facilities. Furthermore, certain rural areas, especially in the Southeast, have disproportionately higher racial and ethnic minority populations. Due to historic and modern injustices these communities often live in persistently poor counties (see Populations That Live Under Persistent Poverty), thus further exacerbating and compounding cancer health disparities.
Individuals Who Belong to Sexual and Gender Minority Populations
According to NIH, the sexual and gender minority (SGM) populations include, but are not limited to, individuals who identify as lesbian, gay, bisexual, transgender, queer, intersex, asexual, and/ or Two-Spirit; those with same-sex or same-gender attractions or behaviors; those with a difference in sex development; and those who do not self-identify with one of these terms but whose sexual orientation, gender identity or expression, or reproductive development is characterized by nonbinary constructs of sexual orientation, gender, and/or sex (63)Centers for Disease Control and Prevention. An Update on Cancer Deaths in the United States. [updated February 28, 2022, cited 2022 April 22].. According to the 2021 Gallup poll, about 5.6 percent of the U.S. population self-identifies as belonging to the SGM population (65)GALLUP. Lgbt Identification Rises to 5.6% in Latest U.S. Estimate. [updated February 24, 2021, cited 2022 April 22]..
There are limited data on the prevalence and incidence of cancer among SGM individuals, with only a handful of studies documenting the cancer disparities that exist in this population (66)Quinn GP, Sanchez JA, Sutton SK, Vadaparampil ST, Nguyen GT, Green BL, et al. Cancer and Lesbian, Gay, Bisexual, Transgender/Transsexual, and Queer/Questioning (Lgbtq) Populations. CA Cancer J Clin 2015;65:384-400. [LINK NOT AVAILABLE]. As noted in the 2011 Institute of Medicine report on lesbian, gay, bisexual, and transgender (LGBT) health—the first comprehensive effort by a federal body to understand the state of SGM health—there are critical gaps in understanding the burden of cancer in this diverse population, many members of which also belong to one or more medically underserved communities (e.g., a person may simultaneously belong to a racial or ethnic minority; identify as a member of the SGM community; and live in a medically underserved remote area)(67)Institute of Medicine (US) Committee on lesbian, Gay, Bisexual, and Transgender Health Issues and Research Gaps and Opportunities. The Health of Lesbian, Gay, Bisexual, and Transgender People. [updated 2011, cited.
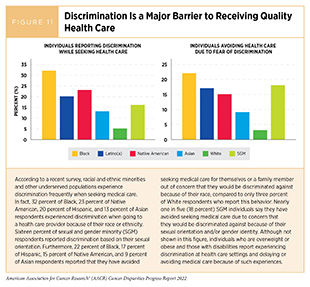
Since the publication of the report, many studies and surveys have evaluated aspects of cancer burden in the SGM community, such as experiences of SGM individuals within the health care system (68)National LGBT Cancer Network. Out: The National Cancer Survey. [updated February 18, 2022, cited 2022 April 22].. It has been documented that potentially modifiable causes of cancer disparities related to SGM identity include implicit biases and discriminatory health care provider behaviors (Figure 11). One important area warranting further research attention includes breast and cervical cancer screening guidelines for transgender individuals.
A follow-up report in 2020 from the National Academy of Sciences, Engineering, and Medicine indicated that some of the goals of the 2011 Institute of Medicine report have been met, but many challenges remain (69)National Academies of Sciences E, Medicine, Division of B, Social S, Education, Committee on P, et al. The National Academies Collection: Reports Funded by National Institutes of Health. In: White J, Sepúlveda MJ, Patterson CJ, editors. Understanding the Well-Being of Lgbtqi+ Populations. Washington (DC): National Academies Press (US);2020. [LINK NOT AVAILABLE]. In particular, comprehensive data on rates of cancer incidence and mortality in the SGM population remain sparse and mostly come from small observational studies (70)Pratt-Chapman ML, Alpert AB, Castillo DA. Health Outcomes of Sexual and Gender Minorities after Cancer: A Systematic Review. Systematic Reviews 2021;10:183. [LINK NOT AVAILABLE], making it difficult to evaluate the true burden of cancer in this population. It is imperative that health care providers collect information on sexual orientation and gender identity from patients with cancer, as Simone Saint Laurent emphasized. Cancer incidence and mortality data for the SGM populations in disaggregated form, for example, by sexual orientation and gender identity, as well as among sexual minorities (e.g., lesbian versus bisexual) and gender minorities (e.g., transgender versus nonbinary) will help researchers accurately capture the true burden of cancer in these heterogeneous and diverse populations. The NIH Sexual and Gender Minority Research Office is leading several research and educational efforts to close the gap in understanding the health needs, including the burden of cancer, among SGM individuals (71)National Institutes of Health. Strategic Plan to Advance Research on the Health and Well-Being of Sexual and Gender Minorities. [updated November 22, 2021, cited 2022 April 22]..
Populations That Live Under Persistent Poverty
According to the USDA, areas of persistent poverty in the U.S. are places where 20 percent or more of the residents have lived below the federal poverty level during a four-decade period. Many of these regions emerged following racial and/ or economic segregation and lack opportunities for residents to rise out of poverty. About 10 percent of U.S. counties fall into this category, and most of them are in the rural Southeast (72)United States Census Bureau. Poverty. [updated February 16, 2022, cited 2022 April 22]..
Areas with low household income share a disproportionate burden of cancer incidence. As one example, a decrease in prostate cancer screening over the past decade, likely because of the USPSTF recommendation in 2012 against routine PSA screening for men between ages 55 and 69 (73)Moyer VA. Screening for Prostate Cancer: U.S. Preventive Services Task Force Recommendation Statement. Ann Intern Med 2012;157:120-34. [LINK NOT AVAILABLE], raised concerns of an increase in new cases of metastatic prostate cancer. A recent study found that the overall incidence of metastatic prostate cancer increased by 18 percent from 2008-9 to 2014-16. Alarmingly, the increase in diagnoses of metastatic prostate cancer was substantially higher—31 percent during the same period—in U.S. counties where residents were living 20 percent below federal poverty levels (74)Zhang AC, Rasul R, Golden A, Feuerstein MA. Incidence and Mortality Trends of Metastatic Prostate Cancer: Surveillance, Epidemiology, and End Results Database Analysis. Canadian Urological Association Journal 2021;15:E637-43. [LINK NOT AVAILABLE]. Even though USPSTF revised its prostate cancer screening guidelines in 2018 and now recommends discussing the potential benefits and harms of routine screening with health care providers (75)U.S. Preventive Services Task Force. Screening for Prostate Cancer: U.S. Preventive Services Task Force Recommendation Statement. JAMA 2018;319:1901-13. [LINK NOT AVAILABLE], it remains to be seen whether this change in guidelines will lead to narrowing of the disparity.
Residents of low-income areas also share a disproportionate burden of cancer deaths. In a landmark study, researchers from NCI presented evidence that persistent poverty is linked with increased rates of cancer deaths. Compared to the counties that do not fall into the persistent poverty category, mortality rates were higher in the persistent-poverty counties for all cancer types (12.3 percent higher), as well as for cancers of lung and bronchus (16.5 percent higher); colon and rectum (17.7 percent higher); stomach (43.2 percent higher); and liver and intrahepatic bile duct (27.6 percent higher) (55)Moss JL, Pinto CN, Srinivasan S, Cronin KA, Croyle RT. Persistent Poverty and Cancer Mortality Rates: An Analysis of County-Level Poverty Designations. Cancer Epidemiol Biomarkers Prev 2020;29:1949-54. [LINK NOT AVAILABLE].
The reasons for higher cancer incidence and mortality in low-income areas are multidimensional and are influenced by adverse differences in SDOH (see Factors That Drive Cancer Health Disparities). Persistent-poverty counties are characterized by larger populations of racial and ethnic minorities; less formal education; limited access to quality health care; and greater unemployment. People living in persistent-poverty counties are also more likely to have higher prevalence of cancer risk factors such as obesity or cigarette smoking (72)United States Census Bureau. Poverty. [updated February 16, 2022, cited 2022 April 22]..
Impact of COVID-19 on Cancer Health Disparities
The COVID-19 pandemic has disrupted the everyday lives of billions of people, exhausted the health care infrastructure and workforce, upended societal norms, and shattered economies worldwide. As of March 31, 2022, the U.S.—which makes up 4.25 percent of the world’s population—accounted for 16.4 percent of global COVID-19 cases and 16.0 percent of global COVID-19 deaths (76)Johns Hopkins Coronavirus Resource Center. COVID-19 Dashboard. [updated April 22, 2022, cited. Unfortunately, many of the same complex and interrelated factors that contribute to U.S. cancer health disparities have also contributed to a disproportionate burden of the disease among racial and ethnic minorities and other medically underserved populations (7)American Association for Cancer Research. Aacr Report on the Impact of COVID-19 on Cancer Research and Patient Care. [updated February 10, 2022, cited 2022 April 22]..
Factors That Drive Cancer Health Disparities
Root causes of cancer health disparities are multidimensional and multifactorial. Over the past few decades, researchers have proposed many models to understand and address health inequities, including cancer health disparities (80)Asare M, Flannery M, Kamen C. Social Determinants of Health: A Framework for Studying Cancer Health Disparities and Minority Participation in Research. Oncol Nurs Forum 2017;44:20-3. [LINK NOT AVAILABLE](81)Warnecke RB, Oh A, Breen N, Gehlert S, Paskett E, Tucker KL, et al. Approaching Health Disparities from a Population Perspective: The National Institutes of Health Centers for Population Health and Health Disparities. American Journal of Public Health 2008;98:1608-15. [LINK NOT AVAILABLE]. A key component of these models is the framework of SDOH. According to NCI, SDOH are the social, economic, and physical conditions in the places where people are born and where they live, learn, work, play, and get older that can affect their health, well-being, and quality of life (82)National Cancer Institute. About the Nci Equity and Inclusion Program. [updated June 14, 2021, cited 2022 April 22].. SDOH have a major positive or negative impact on people’s health, well-being, and quality of life (Figure 5, p. 37). It is increasingly evident that, structural racism and systemic injustices are key contributors to adverse SDOH, creating conditions that perpetuate health inequities, including cancer health disparities, for racial and ethnic minorities and other medically underserved populations (80)Asare M, Flannery M, Kamen C. Social Determinants of Health: A Framework for Studying Cancer Health Disparities and Minority Participation in Research. Oncol Nurs Forum 2017;44:20-3. [LINK NOT AVAILABLE].

Notably, the overall health outcomes of a person, community, or society are determined by the overlapping as well as intersecting nature of SDOH. Thus, SDOH must be examined at individual, communal, and societal levels to comprehensively understand and address health inequities(83)National Institute on Minority Health and Health Disparities. National Minority Health and Health Disparities Research Framework. [updated December 2, 2021, cited 2022 April 22].. As one example, people who do not have access to grocery stores with healthy foods, or those who have access but cannot afford healthy foods, are less likely to have good nutrition. Lack of good nutrition, in turn, can increase the likelihood of developing health conditions, such as obesity and diabetes, that are major risk factors for cancer and other chronic diseases. Because SDOH are interconnected (Figure 5), promoting healthy choices alone will be insufficient to eliminate health disparities in this context. Instead, stakeholders from multiple sectors, such as education, health, labor, transportation, and housing, will need to take collective and coordinated action to improve access and affordability of healthy food and safe green spaces and gyms for physical activity, as well as to raise awareness of health benefits of eating well.
In recent years, there has been an increased focus on incorporating SDOH in public health programs. For example, addressing various aspects of SDOH is one of the five key objectives of the Healthy People 2030 Framework—a program by the United States Department of Health and Human Services (HHS) to promote, strengthen, and evaluate the nation’s efforts to improve the health and well-being of all people (87)U.S. Department of Health and Human Services, Office of Disease Prevention and Health Promotion. Social Determinants of Health. [updated August 18, 2020, cited 2022 April 22].. The National Institute of Minority Health and Disparities (NIMHD) Research Framework organizes SDOH in five domains of influence— biological, behavioral, physical/built environment, sociocultural environment, and health care system—whereby each domain can be influenced at four distinct levels—individual, interpersonal, community, and societal (83)National Institute on Minority Health and Health Disparities. National Minority Health and Health Disparities Research Framework. [updated December 2, 2021, cited 2022 April 22].. Researchers are also applying multilevel and transdisciplinary approaches to move the field of cancer health disparities research from simply describing different outcomes among populations into an established field of convergence science—the research that explores how social, lifestyle, structural, and biological determinants of health can impact each other to either exacerbate or mitigate disparities and either thwart or promote health equity (91)Mensah GA, Riley WT. Social Determinants of Health and Implementation Research: Three Decades of Progress and a Need for Convergence. Ethn Dis 2021;31:1-4. [LINK NOT AVAILABLE]. The overarching goal of such efforts is to identify and address knowledge gaps relevant to understanding and improving health and to the understanding and reduction of health disparities so that informed policy decisions can be made to achieve health equity for all.
In this section, we discuss key factors that overlap and intersect and, independently as well as collectively, contribute to cancer health disparities. It is important to note that the same SDOH that drive cancer health disparities also contributed to COVID-19 pandemic-related health inequities, as discussed in the AACR Report on the Impact of COVID-19 on Cancer Research and Patient Care, released early in early 2022 (7)American Association for Cancer Research. Aacr Report on the Impact of COVID-19 on Cancer Research and Patient Care. [updated February 10, 2022, cited 2022 April 22]..
Socioeconomic Status
Socioeconomic status (SES) is the social standing of an individual or a group. SES can be measured at the individual or neighborhood level. At the individual level, it is typically based on a person’s income, education level, occupation, and other factors. SES at the neighborhood level includes the SES of the residents and also captures influences of the social environment on access to goods and services; levels of crime, safety, and policing; and social norms (3)Cancer Health Disparities Definitions and Examples – National Cancer Institute. [updated February 17, 2015, cited 2022 April 22].. SES is one of the most important factors that contribute to cancer health disparities in people of all races and ethnicities (92)Homan P, Brown TH, King B. Structural Intersectionality as a New Direction for Health Disparities Research. Journal of Health and Social Behavior 2021;62:350-70. [LINK NOT AVAILABLE](93)Bailey ZD, Krieger N, Agénor M, Graves J, Linos N, Bassett MT. Structural Racism and Health Inequities in the USA: Evidence and Interventions. Lancet 2017;389:1453-63. [LINK NOT AVAILABLE](94)Agénor M. Future Directions for Incorporating Intersectionality into Quantitative Population Health Research. American Journal of Public Health 2020;110:803-6. [LINK NOT AVAILABLE](95)Kelly-Brown J, Palmer Kelly E, Obeng-Gyasi S, Chen J, Pawlik TM. Intersectionality in Cancer Care: A Systematic Review of Current Research and Future Directions. PsychoOncology;31:705-716. [LINK NOT AVAILABLE]. For example, a low SES substantially increases the likelihood of exposures to environmental (e.g., living in areas with high levels of air pollutants); behavioral (e.g., excessive alcohol intake); and clinical (e.g., lack of access to health insurance) risk factors, all of which can lead to adverse cancer outcomes.
It is known that many racial and ethnic minorities and other medically underserved populations live in conditions that perpetuate low SES. According to the 2020 U.S. Census, 19.5 percent of the Black and 17 percent of the Hispanic populations were living below the federal poverty level compared to 8.2 percent of the NHW population (96)United States Census Bureau. Income and Poverty in the United States: 2020. [updated September 14, 2021, cited 2022 April 22].. Those living in poverty lack access to healthy food; stable employment; suitable housing; formal education; and quality health care, all of which contribute to unhealthy behaviors and not only increase the risk of developing cancer and other chronic diseases, but also result in adverse health outcomes (see Populations That Live Under Persistent Poverty).
A recent study found that women residing in the lowest-SES neighborhoods of New York City were 73 percent more likely to develop cervical cancer than those in the highest-SES neighborhoods (98)Cham S, Li A, Rauh-Hain JA, Tergas AI, Hershman DL, Wright JD, et al. Association between Neighborhood Socioeconomic Inequality and Cervical Cancer Incidence Rates in New York City. JAMA Oncol 2022;8:159-61. [LINK NOT AVAILABLE]. Another example of how SES impacts health outcomes is the finding that overall cancer mortality rates among individuals with 12 or fewer years of formal education are more than double of that among individuals with at least 16 years of formal education (13)Islami F, Guerra CE, Minihan A, Yabroff KR, Fedewa SA, Sloan K, et al. American Cancer Society’s Report on the Status of Cancer Disparities in the United States, 2021. CA Cancer J Clin 2022;72:112-43. [LINK NOT AVAILABLE]. An emerging and important factor with potential to widen the disparities gap for individuals with low SES is access to digital services, such as reliable Internet connection and computers. Based on recent data, only 69 percent of Black adults and 67 percent of Hispanic adults reported owning a desktop or laptop computer compared to 80 percent of White adults (99)Pew Research Center. Home Broadband Adoption, Computer Ownership Vary by Race, Ethnicity in the U.S. [updated August 20, 2019, cited 2022 April 22].. The essentiality of digital services—especially in providing remote care through telemedicine to patients with cancer among other diseases—is underscored by the COVID-19 pandemic, raising concerns among researchers that the “digital divide” will further exacerbate cancer health disparities (see sidebar on What Is Telemedicine?) (7)American Association for Cancer Research. Aacr Report on the Impact of COVID-19 on Cancer Research and Patient Care. [updated February 10, 2022, cited 2022 April 22]..
Social and Built Environments
Neighborhoods where people live and work can be broadly described in terms of their social and built characteristics that intersect and overlap with each other to influence health outcomes. Social environment of a neighborhood is determined by the racial and ethnic composition of the community; SES of individuals and the neighborhood (see Socioeconomic Status); and residential segregation and distribution. These broad categories, in turn, determine cultural norms, quality of education, and crime, among other characteristics of a neighborhood. Built or physical environment of a neighborhood contains transportation; public services; and policies and regulations, all of which influence the availability of and access to food, medical facilities, and green spaces, among other attributes of a neighborhood. In addition to the individual SES, social and built environments of a neighborhood independently influence the cancer continuum (100)Gomez SL, Shariff-Marco S, DeRouen M, Keegan TH, Yen IH, Mujahid M, et al. The Impact of Neighborhood Social and Built Environment Factors across the Cancer Continuum: Current Research, Methodological Considerations, and Future Directions. Cancer 2015;121:2314-30. [LINK NOT AVAILABLE].
Decades of research have shown that the physical environments and surroundings in which people live and work are key determinants of exposure to risk factors that can adversely affect health outcomes (101)Koohsari J, Nakaya T, McCormack G, Oka K. Built Environment Design and Cancer Prevention through the Lens of Inequality. Cities 2021. [LINK NOT AVAILABLE]. This knowledge has prompted the U.S. HHS to include promoting healthier environments at home and workplaces as one of the five objectives of the Healthy People 2030 initiative (102)U.S. Department of Health and Human Services. Environmental Health. [updated August 18, 2020, cited 2022 April 22].. Due to a long history of racial segregation in the U.S., racial and ethnic minorities are more likely to live in poor neighborhoods. Although the number of individuals belonging to racial and ethnic minorities who live in poor neighborhoods has dropped by 10 percentage points between 1990 and 2019, more than 16 percent still live in poor neighborhoods compared to about 4 percent of the White population (103)National Equity Atlas. Neighborhood Poverty. [updated January 1, 2022, cited 2022 April 22]., increasing their likelihood of exposure to cancer risk factors. As noted above, these neighborhoods are also characterized by financially constrained public school systems, resulting in more limited higher education and future employment prospects, thereby perpetuating a legacy of generations that are trapped in poverty. This residential racial segregation contributes to the lack of diversity in the health care workforce (see Diversity in the Cancer Care Workforce), yet another source of cancer health disparities.
Historic and egregious housing policies such as redlining—a discriminatory practice in which financial and other services are withheld from potential customers who reside in neighborhoods classified as “hazardous” for investment—have resulted in residential segregation of many low-income people, often belonging to racial and ethnic minorities, into neighborhoods with industrial facilities and high air pollution. Although not legally supported, redlining and racial bias in mortgage lending continue to this day. A recent study found that women with breast cancer living in contemporary redlined areas were at a 58 percent increased risk of breast cancer mortality (105)Collin LJ, Gaglioti AH, Beyer KM, Zhou Y, Moore MA, Nash R, et al. Neighborhood-Level Redlining and Lending Bias Are Associated with Breast Cancer Mortality in a Large and Diverse Metropolitan Area. Cancer Epidemiol Biomarkers Prev 2021;30:53-60. [LINK NOT AVAILABLE]. Furthermore, a 2019 report by the U.S. Environmental Protection Agency (EPA) found that the Black and Hispanic individuals were consistently at a higher risk of exposure to air pollutants, as well as pollution-related adverse health effects, compared to White individuals (103)National Equity Atlas. Neighborhood Poverty. [updated January 1, 2022, cited 2022 April 22].. Another example of the impact of environmental pollutants on the health of workers comes from the exposure of Latino migrants, who account for nearly 75 percent of farmworkers in the U.S., to pesticides that are known to cause cancer (106)Castillo F, Mora AM, Kayser GL, Vanos J, Hyland C, Yang AR, et al. Environmental Health Threats to Latino Migrant Farmworkers. Annual Review of Public Health 2021;42:257-76. [LINK NOT AVAILABLE]. Concerningly, a recent study in California found that adolescent Latino boys whose mothers have been exposed to a commonly used pesticide are at a higher risk of developing testicular cancer (107)Froelich W. Pesticide Plays a Large Role in Development of Testicular Cancer. Oncology Times 2020;42:33. [LINK NOT AVAILABLE].
Mental Health
Mental health encompasses the emotional, psychological, and social well-being of a person and affects how one thinks, feels and acts (108)U.S. Department of Health and Human Services. What Is Mental Health? [updated February 28, 2022, cited 2022 April 22].. Negative mental health and the resulting psychological stress can directly or indirectly cause several physical health problems. While it is unclear whether the psychological stress is a direct cause of cancer, a growing body of knowledge suggests a reciprocal link between cancer and psychological and mental health of a person (109)Eckerling A, Ricon-Becker I, Sorski L, Sandbank E, Ben-Eliyahu S. Stress and Cancer: Mechanisms, Significance and Future Directions. Nature Reviews Cancer 2021;21:767-85. [LINK NOT AVAILABLE]. A recent study found that increased psychological distress was associated with increased cancer mortality (110)Huang W, Aune D, Ferrari G, Zhang L, Lan Y, Nie J, et al. Psychological Distress and All-Cause, Cardiovascular Disease, Cancer Mortality among Adults with and without Diabetes. Clin Epidemiol 2021;13:555-65. [LINK NOT AVAILABLE]. Furthermore, studies have shown that individuals who are under persistent stress, as well as those who have experienced adverse childhood experiences, can develop certain behaviors, such as tobacco smoking, that can increase the risk of developing cancer. A cancer diagnosis substantially impacts the mental and psychological health and well-being of a person (111)Niedzwiedz CL, Knifton L, Robb KA, Katikireddi SV, Smith DJ. Depression and Anxiety among People Living with and Beyond Cancer: A Growing Clinical and Research Priority. BMC Cancer 2019;19:943. [LINK NOT AVAILABLE]. For example, a recent study found that more than eight percent of individuals received a mental health diagnosis within 200 days of being diagnosed with cancer (112)Chen WC, Boreta L, Braunstein SE, Rabow MW, Kaplan LE, Tenenbaum JD, et al. Association of Mental Health Diagnosis with Race and All-Cause Mortality after a Cancer Diagnosis: Large-Scale Analysis of Electronic Health Record Data. Cancer 2022;128:344-52. [LINK NOT AVAILABLE]. There are also indications that psychological stress is moderately linked to cancer recurrence (113)Oh H-M, Son C-G. The Risk of Psychological Stress on Cancer Recurrence: A Systematic Review. Cancers 2021;13:5816. [LINK NOT AVAILABLE].
A large recent study examined the likelihood of psychological distress as a risk factor for U.S. cancer mortality between 1997 and 2014. Researchers found that cancer mortality risk was 33 percent higher in adults with serious psychological distress compared to adults without psychological distress (115)Lee H, Singh GK. The Association between Psychological Distress and Cancer Mortality in the United States: Results from the 1997-2014 NHIS-NDI Record Linkage Study. Ann Behav Med 2021;55:621-40. [LINK NOT AVAILABLE].
Mental health intersects with other SDOH: low SES is associated with more frequent mental health problems (117)Lorant V, Deliège D, Eaton W, Robert A, Philippot P, Ansseau M. Socioeconomic Inequalities in Depression: A Meta-Analysis. Am J Epidemiol 2003;157:98-112. [LINK NOT AVAILABLE]; persistent poverty adversely impacts mental health of adolescents (118)Adjei NK, Schlüter DK, Straatmann VS, Melis G, Fleming KM, McGovern R, et al. Impact of Poverty and Family Adversity on Adolescent Health: A Multi-Trajectory Analysis Using the Uk Millennium Cohort Study. Lancet Reg Health Eur 2022;13:100279. [LINK NOT AVAILABLE]; living in more urban environments is linked with negative mental health outcomes (119)Beemer CJ, Stearns-Yoder KA, Schuldt SJ, Kinney KA, Lowry CA, Postolache TT, et al. A Brief Review on the Mental Health for Select Elements of the Built Environment. Indoor and Built Environment 2021;30:152-65. [LINK NOT AVAILABLE]; and, while the link between race/ethnicity and mental health is more complex, those belonging to racial and ethnic minorities report consistently higher psychological stress and mental trauma compared to White people (120)Williams DR. Stress and the Mental Health of Populations of Color: Advancing Our Understanding of Race-Related Stressors. J Health Soc Behav 2018;59:466-85. [LINK NOT AVAILABLE].
Modifiable Risk Factors
Modifiable risk factors are aspects of behavior that can be changed to decrease the risk of developing cancer. These individual health behaviors include smoking, malnutrition, alcohol consumption, exposure to carcinogenic pathogens, and limited physical activity, and are often shaped by a person’s SES as well as the social and built environments. It is thus not surprising that racial and ethnic minorities and other medically underserved populations experience disparities in the burden of many modifiable cancer risk factors (see Disparities in the Burden of Preventable Cancer Risk Factors). It is noteworthy that most cancer risk factors also contribute to other chronic diseases, such as diabetes and chronic renal disease, which are also more common in racial and ethnic minorities and may influence disparities in cancer survival and treatment outcomes (43)Zavala VA, Bracci PM, Carethers JM, Carvajal-Carmona L, Coggins NB, Cruz-Correa MR, et al. Cancer Health Disparities in Racial/Ethnic Minorities in the United States. Br J Can 2021;124:315-32. [LINK NOT AVAILABLE]. Moreover, foreign-born people may face an increased risk for specific cancers associated with infection with cancer-associated pathogens that have higher incidence in their countries of origin (see Infectious Agents).
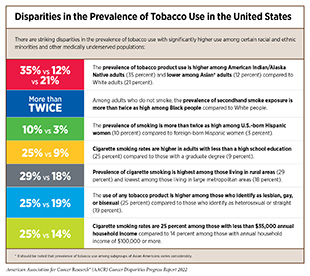
According to one estimate, 42 percent of cancer cases and 45 percent of all cancer deaths in the U.S. in 2014 were attributable to modifiable risk factors (121)American Cancer Society. Cancer Prevention & Early Detection Facts & Figures 2021-2022. [updated January 12, 2021, cited 2022 April 22].. Many of the modifiable cancer risk factors—smoking, physical inactivity, excess alcohol consumption, obesity—are also more prevalent in racial and ethnic minorities and other medically underserved populations (see sidebars on Disparities in the Prevalence of Tobacco Use in the United States; and Racial and Ethnic Disparities in Obesity, Diet, and Physical Activity in the United States).

There are only a few studies, especially those with racially and ethnically diverse study populations, that are directly examining the effects of changing or reducing risky health behaviors on decreasing the cancer risk. Most studies have primarily focused on Black women at high risk for breast cancer (122)Bandera EV, Alfano CM, Qin B, Kang DW, Friel CP, Dieli-Conwright CM. Harnessing Nutrition and Physical Activity for Breast Cancer Prevention and Control to Reduce Racial/Ethnic Cancer Health Disparities. Am Soc Clin Oncol Educ Book 2021;41:1-17. [LINK NOT AVAILABLE]. As an example, one study reported a marked reduction in signs of metabolic syndrome—a collection of conditions that include high cholesterol and excess body fat around the waist—following a 6-month light-to-moderate exercise program in Black women with unhealthy weight (123)Dash C, Taylor TR, Makambi KH, Hicks J, Hagberg JM, Adams-Campbell LL. Effect of Exercise on Metabolic Syndrome in Black Women by Family History and Predicted Risk of Breast Cancer: The Fierce Study. Cancer 2018;124:3355-63. [LINK NOT AVAILABLE].
Because modifiable behaviors affect the risk of developing cancer over longer periods of time, researchers are evaluating various multipronged and long-term interventions in medically underserved populations, including: increasing awareness of cancer risk factors among middle and high school students in the Appalachian Kentucky region (124)Hudson L, Sharp K, Prichard C, Ickes MJ, Alameh S, Vanderford NL. Cancer Curriculum for Appalachian Kentucky Middle and High Schools. Journal of Appalachian Health 2021;3:45. [LINK NOT AVAILABLE]; implementing evidence-based obesity education curricula that are specifically tailored for the Mexican Hispanic community, which has high prevalence of obesity (125)Valenzuela R, Morales A, Sheen J, Rangel S, Salinas JJ. The Implementation of Evidence-Based Obesity Education Curricula to Prevent Cancer in a Predominantly Mexican-American Community on the U.S.-Mexico Border. J Cancer Educ 2021:1-10. [LINK NOT AVAILABLE]; utilizing the reach of faith-based organizations for weight loss interventions to reduce cancer risk in Black men (126)Griffith DM, Jaeger EC. Mighty Men: A Faith-Based Weight Loss Intervention to Reduce Cancer Risk in African American Men. Advances in cancer research 2020;146:189-217. [LINK NOT AVAILABLE]; developing interactive cancer risk-reduction education tools (127)Zeinomar N, Grant-Alfieri A, Burke KR, de Hoz M, Tehranifar P, Walker DAH, et al. Cancer Risk Reduction through Education of Adolescents: Development of a Tailored Cancer Risk-Reduction Educational Tool. J Cancer Educ 2021. [LINK NOT AVAILABLE]; using narrative approaches to educate Hispanic women about the importance of screening for cervical cancer (128)Murphy ST, Frank LB, Chatterjee JS, Moran MB, Zhao N, Herrera PAd, et al. Comparing the Relative Efficacy of Narrative Vs Nonnarrative Health Messages in Reducing Health Disparities Using a Randomized Trial. American Journal of Public Health 2015;105:2117-23. [LINK NOT AVAILABLE](129)Ochoa CY, Murphy ST, Frank LB, Baezconde-Garbanati LA. Using a Culturally Tailored Narrative to Increase Cervical Cancer Detection among Spanish-Speaking Mexican-American Women. Journal of Cancer Education 2020;35:736-42. [LINK NOT AVAILABLE]; and employing smartphone-based interventions to promote smoking cessation among Alaska Native women (130)Alaska Native Tribal Health Consortium and the University of Vermont. Smartphone-Based Financial Incentives to Promote Smoking Cessation among Pregnant Women. [updated July 29, 2021, cited 2022 April 22].. Findings of these and other ongoing efforts will provide a clearer understanding of which interventions are successful in modifying unhealthy behavior to reduce cancer risk. Furthermore, it will be equally important to create interventions that are culturally tailored and inclusive, i.e., the study design, materials, and other components of the intervention reflect cultural needs and preferences of the community (131)Joo JY, Liu MF. Culturally Tailored Interventions for Ethnic Minorities: A Scoping Review. Nursing Open 2021;8:2078-90. [LINK NOT AVAILABLE].
Biological Factors
Since the decoding of the human genome more than two decades ago, research has increased our knowledge and understanding of the biological mechanisms that can lead to cancer development (see Understanding Cancer Development in the Context of Cancer Health Disparities). We now know that subtle changes in DNA sequence of certain genes, as well as changes in the patterns of expression of cancer-related genes, have the potential to increase the risk of cancer development. Research further shows that a combination of genetic changes and environmental influences can potentially contribute to racial disparities in cancer incidence and progression. It is important to note that, despite an explosion in our knowledge of the genetic basis of cancer development, much of the genome-wide information on the burden of cancer has been gleaned from studies in populations of primarily European ancestry, with substantial underrepresentation of racial and ethnic minorities.
As an example of the link between genetic ancestry and burden of cancer, Black women in the U.S. have a disproportionately higher rate of developing TNBC, a particularly aggressive type of breast cancer, compared to White women (132)Siddharth S, Sharma D. Racial Disparity and Triple-Negative Breast Cancer in African-American Women: A Multifaceted Affair between Obesity, Biology, and Socioeconomic Determinants. Cancers 2018;10:514. [LINK NOT AVAILABLE]. Researchers have found that TNBC is more prevalent in Black women who trace their ancestry to West Africa, and more specifically to Ghana (133)Stark A, Kleer CG, Martin I, Awuah B, Nsiah-Asare A, Takyi V, et al. African Ancestry and Higher Prevalence of Triple-Negative Breast Cancer. Cancer 2010;116:4926-32. [LINK NOT AVAILABLE](134)Newman LA, Jenkins B, Chen Y, Oppong JK, Adjei E, Jibril AS, et al. Hereditary Susceptibility for Triple Negative Breast Cancer Associated with Western Sub-Saharan African Ancestry: Results from an International Surgical Breast Cancer Collaborative. Ann Surg 2019;270:484-92. [LINK NOT AVAILABLE]. Similar links have been identified between ancestry and risk of developing prostate cancer in Black men (31)McHugh J, Saunders EJ, Dadaev T, McGrowder E, Bancroft E, Kote-Jarai Z, et al. Prostate Cancer Risk in Men of Differing Genetic Ancestry and Approaches to Disease Screening and Management in These Groups. Br J Can 2021;126(10):1366-73. [LINK NOT AVAILABLE](135)Conti DV, Darst BF, Moss LC, Saunders EJ, Sheng X, Chou A, et al. Trans-Ancestry Genome-Wide Association Meta-Analysis of Prostate Cancer Identifies New Susceptibility Loci and Informs Genetic Risk Prediction. Nature genetics 2021;53:65-75. [LINK NOT AVAILABLE]. Studies linking certain genetic variations with risk of developing specific cancer types carry the enormous potential of developing precise screening and/or treatment strategies (see Integrating and Translating our Knowledge). However, a key limitation of these studies is not only the lack of sufficiently diverse populations, but also the low number of racial and ethnic minority individuals who do participate. It is imperative to include racially and ethnically diverse populations in genomic research studies so that the promise of precision medicine can be fully realized.
Health Care Access and Experiences
The lack of access to quality health care, often associated with low SES, is a key driver of health disparities, including disparities in cancer care. According to the National Academy of Medicine, the quality of health care is the degree to which health care services for individuals and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge. It is well known that racial and ethnic minorities and other medically underserved populations receive lower quality care compared to White individuals (95)Kelly-Brown J, Palmer Kelly E, Obeng-Gyasi S, Chen J, Pawlik TM. Intersectionality in Cancer Care: A Systematic Review of Current Research and Future Directions. PsychoOncology;31:705-716. [LINK NOT AVAILABLE]. In the U.S., the only industrialized nation without universal health coverage for all citizens (136)The Economist. America Is a Health-Care Outlier in the Developed World. [updated April 26, 2018, cited 2022 April 22]., a key contributor to these access inequities is the lack of universal health insurance coverage.
In the U.S., a higher proportion of individuals belonging to racial and ethnic minorities and other medically underserved populations are without health insurance. Among those older than 65 years of age in 2019, 30.2 percent of Hispanic, 25.9 percent of AI/AN, and 14.3 percent of Black people were without insurance compared to 10.2 percent of White or 7.1 percent of Asian people (13)Islami F, Guerra CE, Minihan A, Yabroff KR, Fedewa SA, Sloan K, et al. American Cancer Society’s Report on the Status of Cancer Disparities in the United States, 2021. CA Cancer J Clin 2022;72:112-43. [LINK NOT AVAILABLE]. Lack of insurance often dictates whether an individual will receive the needed health care. Furthermore, compared to those with private insurance, uninsured individuals are less likely to be up to date with the recommended cancer screening and are more likely to be diagnosed with cancer at an advanced stage. It is noteworthy that insurance alone does not guarantee access to quality health care. For example, the distance between the place of residence and a well-equipped health care facility with highly trained staff can be a barrier to receiving quality health care (31)McHugh J, Saunders EJ, Dadaev T, McGrowder E, Bancroft E, Kote-Jarai Z, et al. Prostate Cancer Risk in Men of Differing Genetic Ancestry and Approaches to Disease Screening and Management in These Groups. Br J Can 2021;126(10):1366-73. [LINK NOT AVAILABLE](135)Conti DV, Darst BF, Moss LC, Saunders EJ, Sheng X, Chou A, et al. Trans-Ancestry Genome-Wide Association Meta-Analysis of Prostate Cancer Identifies New Susceptibility Loci and Informs Genetic Risk Prediction. Nature genetics 2021;53:65-75. [LINK NOT AVAILABLE]. One study found that the racial and ethnic disparities in treatment of colon cancer persisted even with comparable insurance status; among privately insured individuals, Black patients were 24 percent less likely to undergo surgical removal and 23 percent less likely to receive chemotherapy, and Hispanic patients were 24 percent less likely to undergo surgical removal compared to NHW patients (139)Hao S, Snyder RA, Irish W, Parikh AA. Association of Race and Health Insurance in Treatment Disparities of Colon Cancer: A Retrospective Analysis Utilizing a National Population Database in the United States. PLOS Medicine 2021;18:e1003842. [LINK NOT AVAILABLE]. In addition, not all health insurance plans are the same, as some may carry high deductibles and copays that can become financially prohibitive for cancer patients. Financial toxicity, or the financial strain associated with a cancer diagnosis, can affect the quality of care that a patient receives, as well as their psychosocial distress (see Financial Toxicity). It must be noted that the COVID-19-related economic recession was disproportionately severe for racial and ethnic minorities, resulting in the loss of employment and employment-based insurance for individuals as well as their families (140)Hamad R, Ruffini K, Bitler M, Currie J. Leveraging the Urgency of Economic Disparities Driven by the COVID-19 Pandemic to Strengthen the U.S. Safety Net. NAM Perspect 2022. [LINK NOT AVAILABLE]. Recovery from the recession has lagged for marginalized communities, further compounding the existing cancer health disparities.
Lack of comprehensive health insurance or any insurance at all disproportionally and adversely affects patients with cancer. The reason is that patients with cancer often receive a combination of different types of treatment—surgery, radiotherapy, chemotherapy, molecularly targeted therapy, and immunotherapy—each of which is costly, even with health insurance. A recent study found that, compared to the privately insured, the risk for advanced breast cancer diagnosis and death from breast cancer was more than double in uninsured women (141)Berrian JL, Liu Y, Lian M, Schmaltz CL, Colditz GA. Relationship between Insurance Status and Outcomes for Patients with Breast Cancer in Missouri. Cancer 2021;127:931-7. [LINK NOT AVAILABLE]. Combined with the higher proportion of uninsured individuals among racial and ethnic minorities and other medically underserved populations, a cancer diagnosis can lead to debilitating financial hardship and adverse health outcomes, further contributing to cancer health disparities (see Financial Toxicity) (139)Hao S, Snyder RA, Irish W, Parikh AA. Association of Race and Health Insurance in Treatment Disparities of Colon Cancer: A Retrospective Analysis Utilizing a National Population Database in the United States. PLOS Medicine 2021;18:e1003842. [LINK NOT AVAILABLE](142)Ko NY, Hong S, Winn RA, Calip GS. Association of Insurance Status and Racial Disparities with the Detection of Early-Stage Breast Cancer. JAMA Oncol 2020;6:385-92. [LINK NOT AVAILABLE](143)Panzone J, Welch C, Pinkhasov R, Jacob JM, Shapiro O, Basnet A, et al. The Influence of Race on Financial Toxicity among Cancer Patients. J Clin Oncol 2021;39:1525. [LINK NOT AVAILABLE].
In addition to the lack of access to quality health care, there are other factors associated with interactions of minority individuals with the health care system that contribute to cancer health disparities. For example, a 2020 survey of 1,769 U.S. adults found that Black and Hispanic adults were more likely to report some negative experiences with health care providers, including providers not believing they were telling the truth or refusing to provide pain medication or other treatments they thought they needed (145)Kaiser Family Foundation. KFF/the Undefeated Survey on Race and Health. [updated October 14, 2020, cited 2022 April 22].. Furthermore, historical atrocities, such as experimental gynecological surgeries performed by the Alabama physician James Marion Sims on enslaved Black women in the nineteenth century (146)A Medical Hell Recounted by Its Victims. [updated February 26, 2019, cited 2022 April 22].; the Tuskegee Study in the early twentieth century conducted in Black people by the medical establishment of the time (147)Centers for Disease Control and Prevention. The Tuskegee Timeline. [updated April 22, 2021, cited 2022 April 22].; or in the 1950s, the development of the first cancer cell line, extensively used in biomedical research, without the consent of a Black woman with the name of Henrietta Lacks (148)Henrietta Lacks: Science Must Right a Historical Wrong. Nature 2020;585:7. [LINK NOT AVAILABLE], all collectively provide important context for understanding the present-day mistrust of the health care system among racial and ethnic minorities. Thus, it is the responsibility of the medical research community and the health care establishment to take proactive and effective measures to alleviate mistrust in the health care system among racial and ethnic minorities. Research also indicates that communication and interaction barriers, such as limited health literacy and limited English language proficiency, contribute to cancer disparities. Racial and ethnic minorities and other medically underserved populations are also underrepresented in clinical studies evaluating the efficacy of anticancer treatments (see Disparities in Cancer Clinical Trial Participation), which can potentially contribute to higher cancer mortality and morbidity. Among the many reasons for low participation—fear of taking an experimental drug, time commitment, travel to the site where study is taking place, out-of-pocket costs—researchers have found that physicians are less likely to discuss clinical studies with minority patients (149)Niranjan SJ, Wenzel JA, Martin MY, Fouad MN, Vickers SM, Konety BR, et al. Perceived Institutional Barriers among Clinical and Research Professionals: Minority Participation in Oncology Clinical Trials. JCO Oncol Pract 2021;17:e666-e75. [LINK NOT AVAILABLE]. When offered, Black patients participate in clinical studies at similar rates compared to White patients (150)Unger JM, Hershman DL, Till C, Minasian LM, Osarogiagbon RU, Fleury ME, et al. “When Offered to Participate”: A Systematic Review and Meta-Analysis of Patient Agreement to Participate in Cancer Clinical Trials. JNCI: Journal of the National Cancer Institute 2020;113:244-57. [LINK NOT AVAILABLE].
Continued and concerted efforts to understand and address the root causes of cancer health disparities are pivotal to realize the bold vision of achieving health equity for all. At the level of the health care system, these efforts must include eliminating gaps in health insurance, increasing access to quality health care, and eradicating discrimination and bias across the cancer care continuum. At the population level, these efforts must include addressing broader structural and socioeconomic factors (151)Thornton RL, Glover CM, Cené CW, Glik DC, Henderson JA, Williams DR. Evaluating Strategies for Reducing Health Disparities by Addressing the Social Determinants of Health. Health Aff (Millwood) 2016;35:1416-23. [LINK NOT AVAILABLE].
Achieving Health Equity: A Vital Investment for the U.S. Public Health and Economy
Cancer takes its toll on individual patients, communities, and the society as a whole. It is instructive to examine the economic burden of cancer and cancer health disparities so that evidence-based strategies can be developed and implemented.
In 2020, the U.S. spending on cancer-related health care was $200.7 billion, accounting for nearly five percent of all health care spending that year (152)American Cancer Society. The Costs of Cancer 2020. [updated October 2020, cited 2022 April 22].(153)153.Centers for Medicare & Medicaid Services. Nhe Fact Sheet. [updated December 15, 2021, cited 2022 April 22].. The cost of cancer care is projected to reach $246 billion by 2030 (152)American Cancer Society. The Costs of Cancer 2020. [updated October 2020, cited 2022 April 22].. These costs are paid by many entities and people including employers, insurance companies, taxpayers, and cancer patients and their families and do not include the indirect cost of lost productivity. According to NCI’s 2021 Annual Report to the Nation on the Status of Cancer, the economic burden associated with cancer care on patients in the U.S. in 2019 was an estimated $21.09 billion, including $16.22 billion in out-of-pocket costs and $4.87 billion in time costs, i.e., the value of time patients spent traveling to and from health care facilities, and waiting for and receiving care (154)Yabroff KR, Mariotto A, Tangka F, Zhao J, Islami F, Sung H, et al. Annual Report to the Nation on the Status of Cancer, Part 2: Patient Economic Burden Associated with Cancer Care. JNCI: Journal of the National Cancer Institute 2021;113:1670-82. [LINK NOT AVAILABLE].
Not surprisingly, racial and ethnic minorities and other medically underserved populations also share a disproportionate economic burden associated with cancer. According to one estimate examining the direct cost of cancer health disparities during 2002-2007, eliminating racial disparities in incidence of the four most common types of cancer—lung, colorectal, breast, and prostate—would have resulted in $2.3 billion in savings on annual medical expenditures by patients with cancer (155)C-Change. The Societal and Economic Impact of Cancer Health Disparities. [updated December 8, 2021, cited 2022 April 22].. Compared to NHW individuals, racial and ethnic minorities also suffer substantially higher person-years of life lost, which is an estimate of the average years a person would have lived if they had not died prematurely. Person-years of life lost is often used by public health experts to determine the economic cost of premature mortality because of a disease or another cause. One study found that lost earnings from cancer deaths in the U.S. in 2015 were $94.4 billion (156)Islami F, Miller KD, Siegel RL, Zheng Z, Zhao J, Han X, et al. National and State Estimates of Lost Earnings from Cancer Deaths in the United States. JAMA Oncol 2019;5:e191460. [LINK NOT AVAILABLE]. Findings from another study indicate that, compared to NHW individuals, person-years of life lost and rates of lost earnings for Black individuals were more than double because of premature deaths related to prostate and stomach cancers and multiple myeloma (157)Zhao J, Miller KD, Islami F, Zheng Z, Han X, Ma J, et al. Racial/Ethnic Disparities in Lost Earnings from Cancer Deaths in the United States. JNCI Cancer Spectrum 2020;4. [LINK NOT AVAILABLE].
In the past decade, there has been some promising progress toward reducing cancer health disparities among racial and ethnic minorities and other medically underserved populations, as is evident by the narrowing gaps in overall cancer incidence and deaths among different populations (Figure 2). It is also reassuring that there is an increased urgency within the cancer community to understand and address cancer health disparities. Among the many federal agencies addressing the health disparities, National Institute on Minority Health and Health Disparities (NIMHD) and NCI, specifically its Center to Reduce Cancer Health Disparities (CRCHD), are key institutes primarily focused on reducing disparities in the burden of cancer. Both institutes and CRCHD spearhead numerous programs and offer many funding opportunities to address cancer health disparities (see sidebar on NCI Programs that Address Disparities in Cancer Prevention and Care). These include basic research on the biology behind disparities; large studies examining the factors that contribute to disparities; programs at the community level that are aimed at overcoming barriers to cancer care; and population-based registries that help to document the extent of the problem and highlight areas for further research.

Cancer health disparities stem from complex and intersecting factors, and thus require comprehensive and multidisciplinary strategies to eliminate them. With the accruing evidence that the COVID-19 pandemic has further exacerbated many of the existing cancer health disparities (7)American Association for Cancer Research. Aacr Report on the Impact of COVID-19 on Cancer Research and Patient Care. [updated February 10, 2022, cited 2022 April 22]., it is all the more important that Congress continue to provide sustained, robust, and predictable increases in funding for the federal agencies, such as NIH, NCI, CDC, and NIMHD, that are at the forefront of addressing the menace of cancer health disparities so that the bold vision of health equity can be realized (see The AACR Call to Action).
Next Section: Understanding Cancer Development in the Context of Cancer Health Disparities