Disparities in Clinical Research and Cancer Treatment
In this section, you will learn:
- Clinical trials are vital for progress against cancer because they translate medical discoveries into meaningful advances in patient outcomes; lack of sociodemographic diversity among clinical trial participants represents a major barrier to advancing cancer care for all patient populations.
- Improved representation among clinical trial participants requires health care providers to offer clinical trial options to all patients regardless of race, ethnicity, geography, or other sociodemographic factors such as health insurance.
- Enhancing diversity among clinical trial participants will require intentional strategies, including broadening overly restrictive eligibility criteria; expanding accrual sites; conducting community outreach and engagement; fostering a cancer research and care workforce that reflects the patients it serves; deploying patient navigation; using culturally tailored patient education; and minimizing the costs associated with trial participation.
- Despite many advances in cancer treatment, including rapid progress in precision medicine, patients from racial and ethnic minority groups, low-income, and other medically underserved populations are less likely to receive the recommended standard of care for their cancer.
- Recent studies have shown that disparities in outcomes for several cancer types can be substantially reduced when all patients have access to and receive guideline-adherent treatments.
- Addressing disparities in treatment and improving the health of medically underserved populations can enhance the quality of care for all and advance population health.
Contents
In the United States (US), the overall cancer death rate is declining steadily, and more individuals are living longer and fuller lives after a cancer diagnosis (274)American Association for Cancer Research. AACR Cancer Progress Report 2025. Accessed: March 31, 2026. . This progress is attributable, in part, to the rapid advances in cancer treatment propelled by breakthroughs in medical research (see Sidebar 22).
Medical research is an iterative process that is set in motion when a discovery with the potential to affect the practice of medicine or public health is made in any area of research or clinical practice. One way that researchers build on a discovery is by asking questions that can be tested through experiments in a wide range of models that mimic healthy and diseased conditions, such as cancer (see Sidebar 9). Results from these experiments can lead to the identification of a potential preventive intervention or therapeutic target, or to the identification of a potential biomarker that can predict how a cancer might behave or how well a treatment might work. They also can feed back into the medical research cycle by providing new discoveries that lead to more questions or hypotheses.
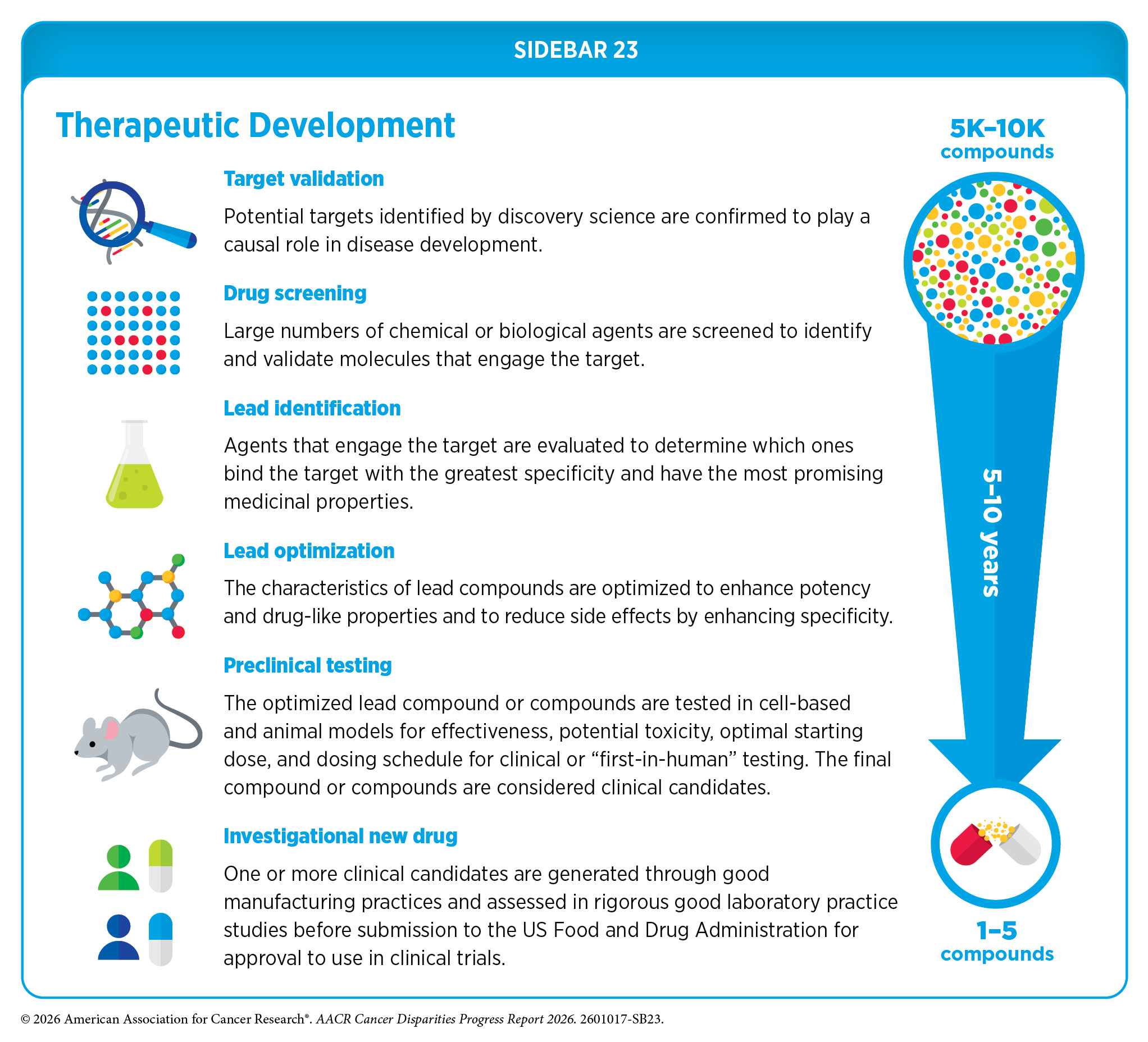
Once a potential therapeutic target is identified, it takes many more years of preclinical cancer research before a candidate therapeutic is developed and ready for testing in clinical trials (see Sidebar 23). During this time, several candidates are rigorously evaluated to identify any potential toxicity and to determine the appropriate doses and dosing schedules for testing in the first clinical trial.
Clinical Research
Clinical research, also known as clinical studies or clinical trials, evaluates the safety and efficacy of candidate agents before they can be approved by the US Food and Drug Administration (FDA) and used as part of routine patient care. There are several types of cancer clinical trials, including prevention trials, screening trials, treatment trials, and supportive or palliative care trials, each designed to answer different research questions. Clinical studies in which participants are randomly assigned to receive an investigational agent or the standard care are called randomized clinical trials and are considered the most rigorous.
Clinical trials are vital for progress against cancer because they translate medical discoveries into meaningful advances in patient outcomes. Therapeutics that constitute today’s standard of care are the direct result of discoveries and evidence generated through past clinical trials. Cancer treatment trials conducted by the Children’s Oncology Group, along with high engagement of pediatric patients in those trials, drove dramatic improvements in outcomes, increasing 5-year survival rates for children with cancer from 60 percent in the 1970s to greater than 80 percent in the 2000s (563)American Association for Cancer Research. AACR Pediatric Cancer Progress Report 2025. Accessed: March 17, 2026. . Similarly, clinical trials conducted over the past decade for previously intractable cancers in adults, including advanced non–small cell lung cancer (NSCLC) and melanoma, have led to transformative advances in clinical practice and patient outcomes (274)American Association for Cancer Research. AACR Cancer Progress Report 2025. Accessed: March 31, 2026. .
Participating in a clinical trial has many benefits. These include access to the latest and potentially more effective treatments before they are widely available, active involvement in making health care decisions, and a direct contribution to lifesaving cancer research for future patients (565)Abu Rous F, et al. (2024) JAMA Oncol, 10: 416. . Institutional review boards critically evaluate and approve the design of all clinical studies before they can begin, and trials are carefully monitored throughout their duration. Patient safety and understanding of the clinical trial are prioritized through the informed consent process, which involves a discussion between the clinical research team and the patient about the trial’s purpose and what is expected of the patient, potential benefits and risks, alternative treatments, and the patient’s right to withdraw at any time.
Clinical trials evaluating potential new cancer treatments have traditionally been conducted in successive phases, each involving more patients and typically focusing on a specific cancer type (e.g., breast cancer or prostate cancer). Phase I studies are designed to determine the optimal dose of an investigational anticancer therapeutic, how patients process it, and potential toxicities. Historically, phase I trials were not designed to evaluate anticancer efficacy of a therapeutic.
However, because of rapid progress in medical research, including clinical trial design and conduct, researchers are increasingly able to incorporate a preliminary evaluation of efficacy from phase I trials (566)Adashek JJ, et al. (2019) Nat Rev Clin Oncol, 16: 773. . Thanks to extraordinary advances in our understanding of cancer biology, patient responses to investigational therapies in phase I studies have also nearly doubled over the past two decades (567)Kingwell K (2022) Nat Rev Drug Discov, 21: 702. .
Phase II trials are designed to determine the initial efficacy of investigational therapy, in addition to continually monitoring for potential toxicities. Phase III studies are large trials designed to determine therapeutic efficacy as compared to current standard of care; when successful, the results of these trials have traditionally been used by FDA to approve new therapeutics or new indications for previously approved therapeutics. Phase IV trials are conducted after a therapeutic is approved by FDA and provide additional effectiveness or real-world data on the therapy. Sometimes phase 0 clinical studies are performed prior to traditional clinical trials wherein low doses of potential therapeutics are administered to a small number of patients to determine whether such treatments may have the desired effect.
The traditional, cancer-specific, multiphase clinical trial process requires large numbers of patients and takes many years to complete. However, this approach is not well suited to the current molecular era—in which the genetic alterations that drive cancer are being identified with greater precision and frequency (see Genetic Alterations), and therapies designed to target those alterations are being actively evaluated in clinical trials. Identifying and implementing more efficient clinical development strategies are areas of extensive investigation.
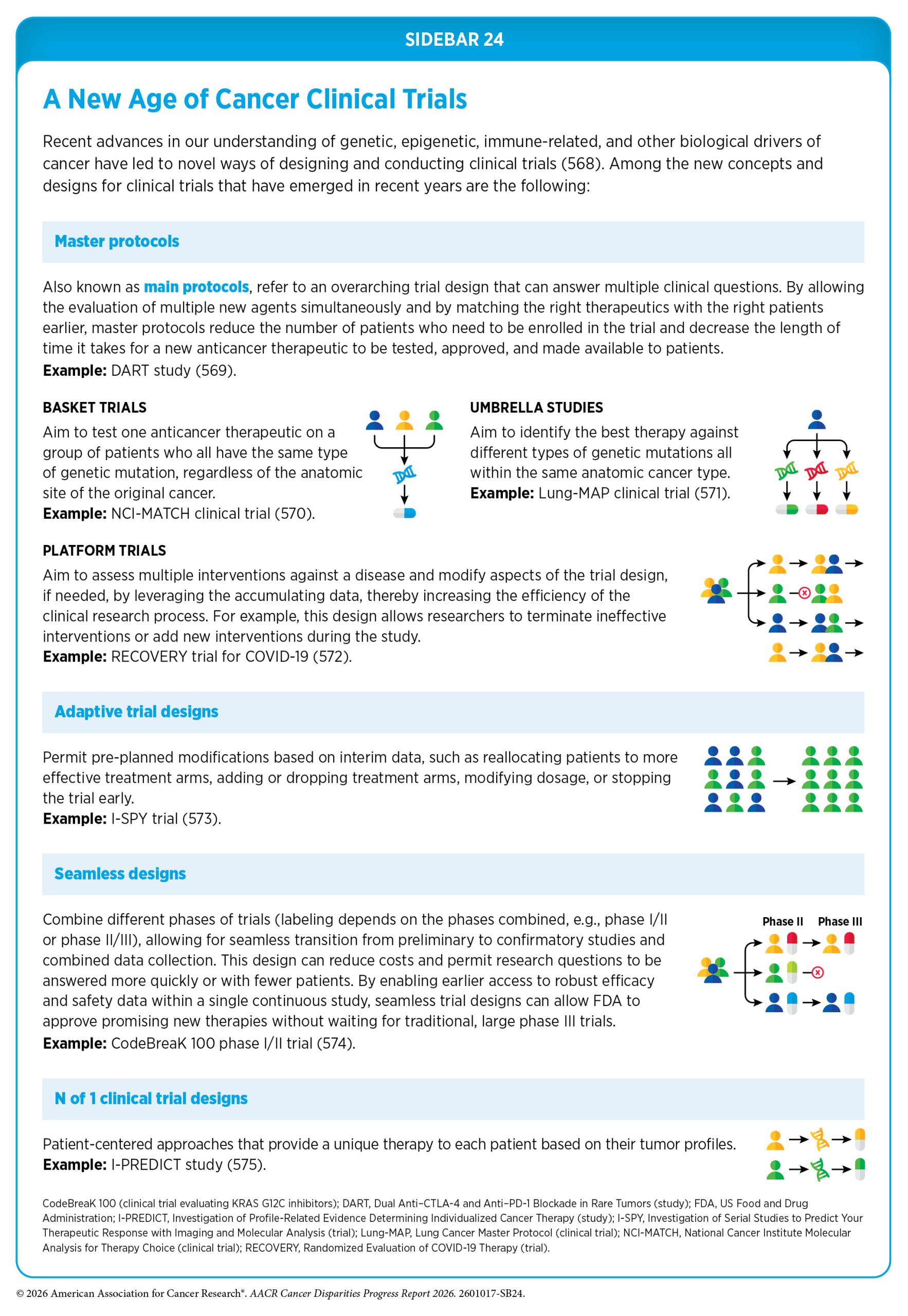
Advances in cancer genomics and related technologies are transforming clinical trials by providing deeper insight into the molecular drivers of cancer and enabling researchers to identify patients most likely to benefit from specific therapies (see Sidebar 24). As a result, clinical research is also evolving from the traditional tissue-based trials to a biomarker-driven and tissue-agnostic approach that involves targeting cancers based on shared molecular features rather than where they originate in the body. Emerging trial designs are therefore increasingly patient-centric, leveraging tools such as advanced gene sequencing, liquid biopsies, and digital monitoring to track tumor evolution and adapt treatments over time (see Understanding Cancer Development in the Context of Cancer Disparities). Additionally, optimized dosing strategies, use of precision medicine earlier in the course of disease, and the integration of large clinical datasets with artificial intelligence (AI) are reshaping clinical research to make trials more efficacious, personalized, and reflective of real-world patient populations.
Challenges in Cancer Clinical Trials
Researchers are continually identifying and implementing new ways to conduct clinical trials that are yielding advances in patient care, but there are numerous opportunities for improvement. Despite major advances in medical research, adult patient participation in cancer clinical trials continues to be extremely low. Based on recent estimates, only 7 percent of adult cancer patients in the United States participate in clinical trials (576)Unger JM, et al. (2024) J Clin Oncol, 42: 2139. . As a result, many studies fail to enroll enough patients to draw meaningful conclusions about the effectiveness of the investigational therapeutic.
Clinical trial participants often do not reflect the broader population of patients receiving cancer care in the United States (577)Balogh EP, et al. (2025) JCO Oncol Pract, 21: 1746. . Patients who participate in clinical trials tend to be younger, healthier, and racially, ethnically, and geographically less diverse compared to the observed national demographics of the cancer burden under study. Diversity among participants is critical because the efficacy and safety of an intervention may differ across populations—for example, among individuals from different ancestral backgrounds, age groups, or biological sexes. Underrepresentation in clinical trials compromises the generalizability of trial findings to the real-world patient population. In this regard, it should be noted that in recent years FDA has decided not to approve cancer therapies when clinical trial participants were not representative of the US patient population due to concerns about applicability to the US population (578)US Food & Drug Administration. July 17, 2025: Meeting of the Oncologic Drugs Advisory Committee – 07/17/2025. Accessed: March 31, 2026. (579)US Food & Drug Administration. May 20-21, 2025: Meeting of the Oncologic Drugs Advisory Committee – 05/20/2025. Accessed: March 31, 2026. .
Disparities in Participation in Adult Cancer Clinical Trials
Recent studies highlight that many segments of the US population, including racial and ethnic minority populations, sexual and gender minority (SGM) populations, individuals living in rural areas and poorer neighborhoods, adolescents and young adults, people with disabilities, and older adults, are underrepresented in cancer clinical trials (72)Unger JM, et al. (2025) CA Cancer J Clin, 75: 341. (577)Balogh EP, et al. (2025) JCO Oncol Pract, 21: 1746. (580)Hanshaw BD, et al. (2025) Nat Med, 31: 720. . Despite the landmark National Institutes of Health (NIH) Revitalization Act of 1993 to improve representation of women and minority populations in clinical trials—and numerous initiatives from FDA and the National Cancer Institute (NCI) since then—progress in increasing diversity has been limited, and underreporting of participants’ race, ethnicity, and age is a persistent challenge.
Most clinical trials in the United States are conducted in large academic cancer centers, which are located in major metropolitan areas. However, nearly 80 percent of US cancer patients are treated at community-based hospitals (581)IQVIA. Advancing Precision Oncology. Trends in Oncology Biomarker Testing in the U.S. Accessed: March 31, 2026. . Based on recent estimates, only 4 percent of patients treated at community cancer clinics participate in clinical trials, compared to greater than 20 percent treated at large, urban academic research institutions (576)Unger JM, et al. (2024) J Clin Oncol, 42: 2139. . Research also shows that US clinical trials are preferentially conducted, and also have higher success rates, in middle- to high-income ZIP codes compared to lower-income ZIP codes (582)Patiyal S, et al. (2026) Sci Rep, 16. . Clinical trial participation is low among patients receiving care at the Veterans Health Administration (VHA) due to multilevel barriers, including limited availability of appropriate trials, complex referral processes outside the VHA system, logistical and financial challenges, and higher rates of medical and psychological comorbidities in the patient population which result in the exclusion of veterans (583)Monreal I, et al. (2025) Mil Med, 190: e891. .
NCI-designated cancer centers are required to report on the racial and ethnic distribution of the area they serve as well as that of their clinical trial participants. Despite these requirements, there is evidence of a persistent lack of racial and ethnic reporting and sociodemographic diversity among US clinical trial participants. A recent study found that only 8.5 percent of cancer clinical trials reported participants’ race or ethnicity (188)Luo M, et al. (2025) Cancer Discov, 15: 511. . Among these trials, White individuals were overrepresented (78 percent to 84 percent); Asian individuals’ representation was 7 percent to 16 percent, Black individuals accounted for less than 7 percent, and Hispanic individuals were also underrepresented (188)Luo M, et al. (2025) Cancer Discov, 15: 511. . Another study that reviewed 471 clinical trials evaluating immune checkpoint inhibitors—one of the most transformative advances in cancer therapy—further highlighted persistent inequities in both reporting and enrollment. Race was not reported in 31 percent and ethnicity in 59 percent of studies, and only 6 percent reported race- or ethnicity-specific outcomes (585)Chua AV, Jr., et al. (2025) JCO Oncol Pract, 21: 408. . Among US-based trials, White patients were overrepresented, whereas Black and Hispanic patients were underrepresented relative to their disease burden.
Encouragingly, an analysis of more than 16,000 participants in NCI Cancer Therapy Evaluation Program early-phase clinical trials from 2000 to 2023 found modest increases in enrollment of Hispanic (from 4.5 percent to 7.7 percent), Asian or Pacific Islander (from 2.2 percent to 4.4 percent), and Black patients (from 6.1 percent to 7.2 percent), particularly following the establishment of the Experimental Therapeutics Clinical Trials Network, which was created in 2014 to accelerate evaluation of innovative therapies using a coordinated, collaborative, and inclusive team-based approach (586)Farooq M, et al. (2025) Cancer Discov, 15: 2251. . During the same period, participation among older adults also improved, with enrollment of patients ages 65 to 74 increasing from 24.6 percent to 32.3 percent and those ages 75 to 84 rising from 6.2 percent to 12.4 percent. However, participation of Hispanic and Black patients was still below their cancer incidence rates in the United States, and enrollment of American Indian or Alaska Native (AIAN) patients remained negligible.
Adults age 65 and older experience the highest cancer incidence, yet they remain underrepresented in clinical trials. As one example, analysis of phase III clinical trials evaluating interventions for acute myeloid leukemia (AML) from the past decade showed that more than 70 percent of participants were less than 65 years old, despite AML being a disease primarily encountered in older patients (587)Gopishetty S, et al. (2020) Am J Transl Res, 12: 5977. Even in trials enrolling only older adults, participation is progressively lower among the oldest patients, those with preexisting medical conditions, and those living far from NCI-designated cancer centers, highlighting the need for targeted strategies to improve enrollment (588)Gong IY, et al. (2025) Cancer, 131: e70204. . Exclusion of older adults is partly attributable to restrictive eligibility criteria, such as presence of comorbidities, use of concomitant medications, prior malignancies, or poor performance status—meaning the lack of ability to carry out daily activities. Underrepresentation of older adults limits the generalizability of clinical trial findings and contributes to evidence gaps for this patient population.
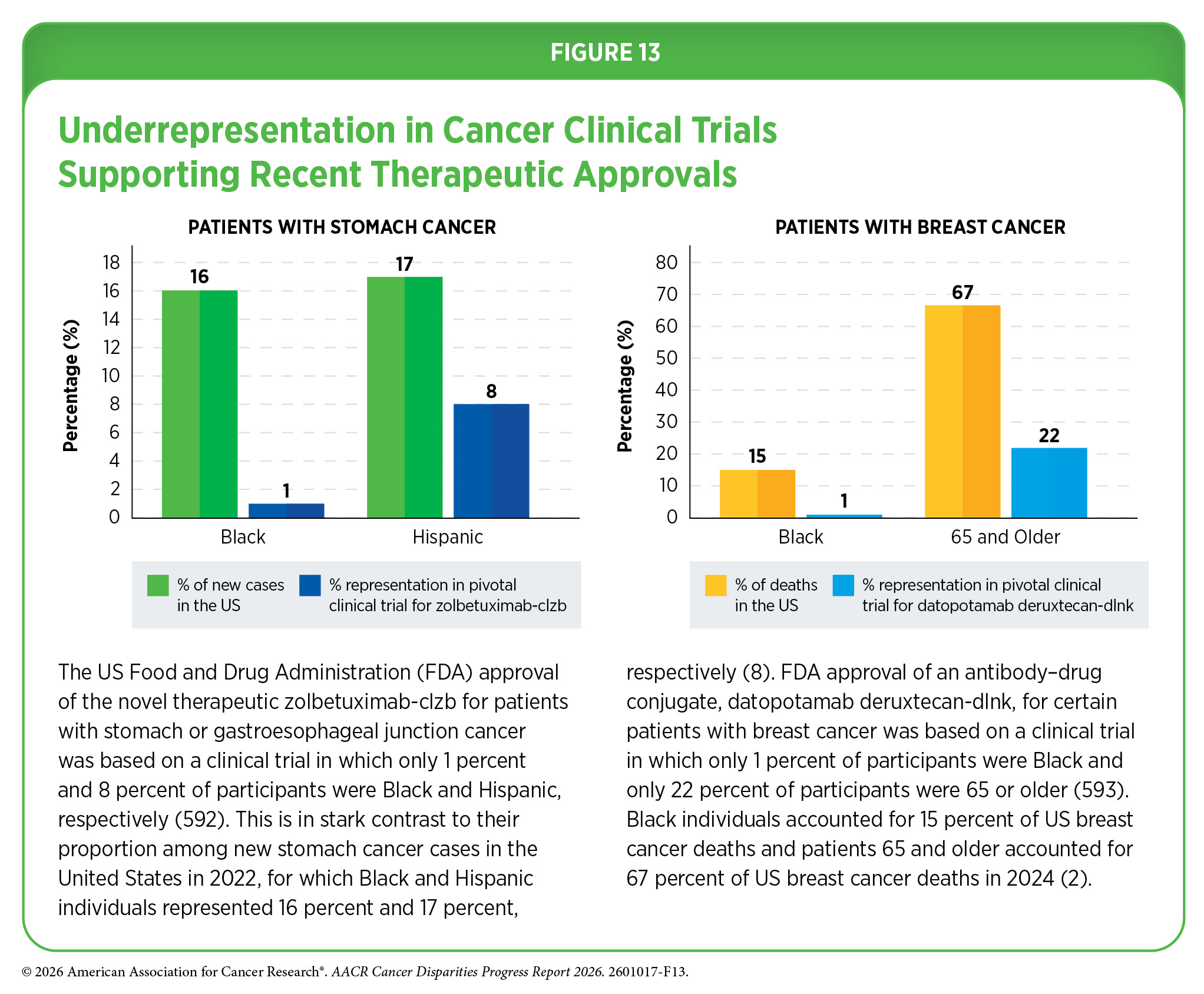
Analysis of FDA’s Drug Trials Snapshots website, which was created to improve transparency regarding participant diversity of pivotal clinical trials of newly approved drugs, indicates that many of the recently approved therapeutics were based on trials with inadequate representation (see Figure 13). According to one study, clinical trials that led to FDA approvals for gynecologic cancer drugs between 2010 and 2024 significantly underenrolled Black and Hispanic women, even though Black and other minority women experience a higher burden of cervical and endometrial cancers (589)Levin G, et al. (2025) Am J Obstet Gynecol, 233: 110 e1. . Another study showed that Native Hawaiian or Pacific Islander (NHPI) patients were rarely included or even identified in clinical trials for cancer therapeutics approved between 2006 and 2021 (590)Taira DA, et al. (2024) JAMA Netw Open, 7: e2442204. .
US lawmakers and FDA were working on legislation and guidelines intended to increase the diversity of clinical trial participants (274)American Association for Cancer Research. AACR Cancer Progress Report 2025. Accessed: March 31, 2026. . These included a diversity action plan that would require researchers and funders of clinical trials to submit concrete goals and needed steps for enrolling specific demographic groups in pivotal studies that are used by FDA to make regulatory decisions on new drugs (591)US Food & Drug Administration. Diversity Action Plans to Improve Enrollment of Participants from Underrepresented Populations in Clinical Studies. Accessed: March 31, 2026. . However, this guidance has now been removed due to a change in federal policy. Other recent policy changes have also jeopardized progress in this critical area of cancer research. Reductions in FDA staffing and federal funding for medical research, along with the elimination of clinical trial diversity initiatives, threaten to delay innovations and treatments that are essential not only for advancing care, but also for ensuring all patients have equitable access to lifesaving therapies.
Representative study populations in clinical trials are essential to accurately assess the efficacy and safety of new treatments, especially for cancers that disproportionately burden specific populations, including those defined by ancestry or racial and ethnic background. Recent analyses of cancer clinical trial outcomes among patients from racial and ethnic minority groups show that Hispanic and Black patients may experience benefits similar to those of White patients despite low participation, emphasizing the importance of diversifying enrollment to ensure an equitable impact of research advances (594)Goel S, et al. (2024) JAMA Netw Open, 7: e2421485. .
Reporting the benefits and potential risks for specific population groups is also critical in evaluating cutting-edge precision medicine, such as molecularly targeted therapies or immunotherapies, because these treatments depend on cancer characteristics, immune system, lifestyle, microbiome, family history, and other personalized attributes of a patient (see Understanding Cancer Development in the Context of Cancer Disparities).
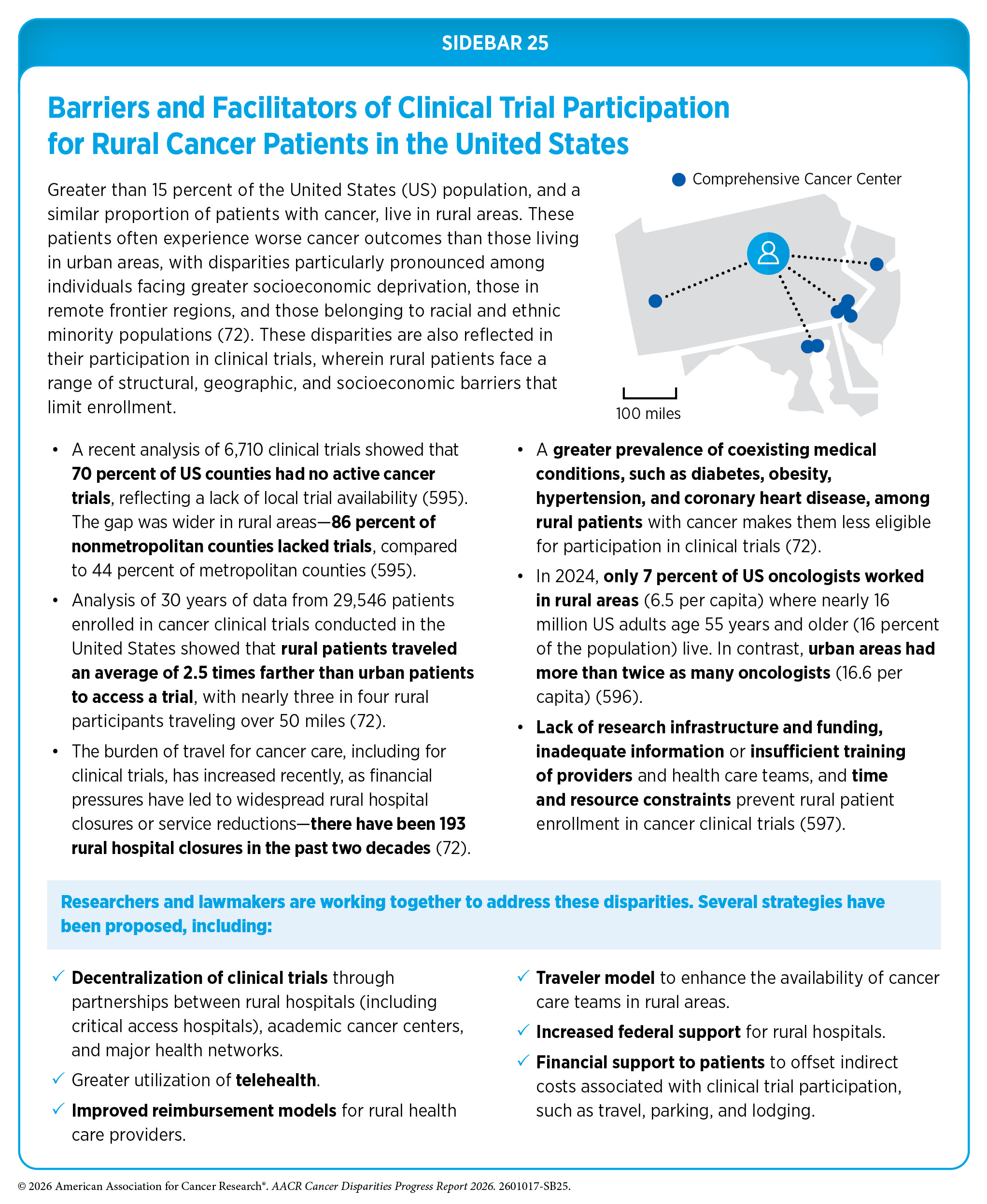
Patients living in rural areas face significant impediments to participating in clinical trials attributable, in large part, to geographic isolation and lack of access to care facilities (see Sidebar 25). Participation in clinical trials can help reduce disparities in cancer outcomes for rural patients due to a greater likelihood of receiving evidence-based standard of care treatments and greater attention to overall health. Understanding the barriers that residents of rural areas face in accessing trials can inform whether the health care system is adequately resourced, comprehensive, affordable, and accessible by the communities it serves (72)Unger JM, et al. (2025) CA Cancer J Clin, 75: 341. .
Barriers to Clinical Trial Participation
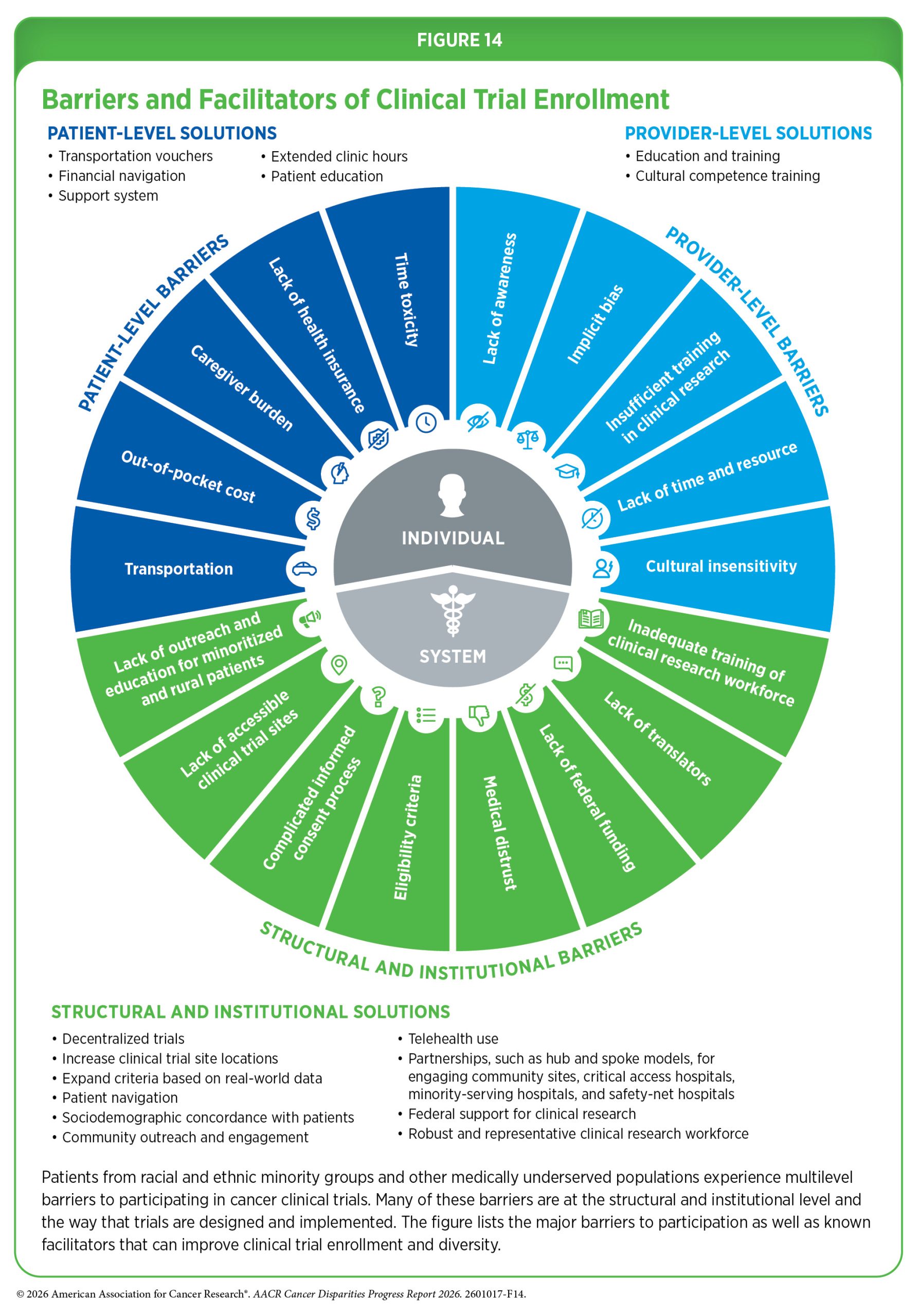
Numerous challenges limit patient participation in cancer clinical trials. While some barriers operate at the individual level for patients and health care providers, most arise from suboptimal clinical trial design and the ways in which trials are implemented within the broader health care system (see Figure 14). It is important to note that the barriers to participation are often unique for distinct populations. For example, racial and ethnic minority populations and rural residents may face barriers created by decades of systemic injustices and structural inequities that persist because of the continued failure of health care systems to address them. These include limited outreach and education of clinical research in communities, lack of sociodemographic concordance with providers, and medical mistrust. SGM populations may encounter barriers caused by societal stigma and the absence of standardized protocols and inclusive recruitment strategies (580)Hanshaw BD, et al. (2025) Nat Med, 31: 720. (598)Akimoto K, et al. (2023) Cancer J, 29: 310. (599)Rosser BRS, et al. (2023) J Clin Oncol, 41: 5093. . Interventions to address barriers to clinical research must therefore take into consideration the unique and specific experiences of the target populations.
Major patient-level barriers include financial and time-related burdens, such as costs of cancer treatment and other medication, transportation, childcare, costs associated with work disruptions and lost wages, and inadequate insurance or complete lack of it (577)Balogh EP, et al. (2025) JCO Oncol Pract, 21: 1746. . Studies have shown that financial factors—in particular, income and property ownership—are among the strongest predictors of clinical trial participation (600)Dong W, et al. (2025) J Natl Compr Canc Netw, 24. (601)Chen N, et al. (2025) JAMA Netw Open, 8: e2515205. . Although the cost of study drugs and research-related expenses are usually covered by clinical trial sponsors, routine care costs must be covered by the patient’s health insurance, and participants may still face out-of-pocket expenses for additional trial-specific activities. Based on one analysis, patients insured through Medicaid were 29 percent less likely to enroll than those with private insurance (600)Dong W, et al. (2025) J Natl Compr Canc Netw, 24. . Another study found that among patients who declined participation in a clinical trial, about 10 percent cited concerns about the extra time required as a reason for not enrolling (601)Chen N, et al. (2025) JAMA Netw Open, 8: e2515205. .
Financial and transportation barriers are heightened in low-income as well as racial and ethnic minority populations, who are more likely to live in economically deprived or socially marginalized areas, have limited English proficiency, and have low vehicle ownership (602)Guadamuz JS, et al. (2024) JNCI Cancer Spectr, 8. . These patients are more likely to be uninsured and self-pay for care (603)Zhao Y, et al. (2025) Cancer, 131: e35944. . Minority patients also frequently report childcare and family-related responsibilities, limited time away from work or school, and greater difficulties paying for health care, transportation, and other costs related to trial participation (603)Zhao Y, et al. (2025) Cancer, 131: e35944. . Transportation vulnerability is more common also among rural patients who often live disproportionately further away from cancer centers and may suffer from financial hardships.
Many barriers exist at the provider level, including lack of knowledge of clinical trials, insufficient training, and implicit biases, such as perceptions that certain patients are less interested in participating (598)Akimoto K, et al. (2023) Cancer J, 29: 310. (604)Coley AK, et al. (2023) JCO Oncol Pract, 19: 154. (605)Castillo BS, et al. (2024) Curr Oncol, 31: 3017. . Lack of dedicated staff to engage with and serve minority patient populations, time constraints for clinicians, and lack of cultural competence and effective communication skills are among the other provider-level factors that hinder representation in clinical trials. Considering that physicians are a trusted source of clinical trial information for most racial and ethnic minority patients (606)Mesa R, et al. (2023) Trans Am Clin Climatol Assoc, 133: 149, identifying ways to enhance physician motivation is vital for patient recruitment in clinical studies. In this regard, performance-based audits and feedback reports that compared an oncologist’s clinical trial recruitment to their peers failed to improve enrollment in one study, highlighting the need for continued efforts to identify new strategies for changes in practice (607)Verdini NP, et al. (2024) Int J Radiat Oncol Biol Phys, 119: 11. .
Primary care providers play a critical role in the health care journey of patients with cancer, with their expertise in early detection, diagnosis, and risk identification laying the foundation for effective treatment and risk reduction. Unfortunately, many primary care providers are not well informed about available clinical trials or the latest advances in cancer research (608)Bylund CL, et al. (2017) Clin Trials, 14: 518. . However, based on a survey of primary care providers, over 90 percent of respondents supported patient participation in an early detection clinical trial (609)Myers R, et al. (2023) Contemp Clin Trials Commun, 34: 101183. .
Beyond individual-level factors, there are barriers that operate at the level of the health care systems, as well as at the community and/or society. Many of these barriers are driven by structural inequities. Some of the major system-level and structural barriers include lack of trial availability for patients, particularly those who live in rural and low socioeconomic areas, or in states and territories that are far from mainland United States. Additional structural barriers include complexity of the clinical trials and consent documents; time constraints for informed consent and clinical trial paperwork; patient exclusion due to strict eligibility criteria; medical distrust; lack of facilitators, such as translators or patient navigators; limited health system capacity to ensure consistent awareness of clinical trials, particularly among medically underserved populations; and lack of community engagement in low-resource settings.
Lack of available trials, long travel distance to study sites, and lack of involvement of community, minority-serving, and safety-net hospitals, where most underserved patients receive care, are major hurdles to enrollment (610)Saez-Ibanez AR, et al. (2022) Nat Rev Drug Discov, 21: 870. . Unfortunately, 70 percent of US counties reported not having any active trials in 2022 (595)Kirkwood MK, et al. (2025) JCO Oncol Pract, 21: 427. . This disparity was greater in counties that are nonmetropolitan and that have high social vulnerability and high cancer mortality. Lack of clinical trial availability in rural areas is especially concerning, given that residents in rural areas have a greater burden of many cancer types. Nearly 17 percent of the US population over 35 years old would have to drive over 100 miles to obtain care at an NCI-funded cancer care facility (611)Shriver SP, et al. (2025) J Clin Transl Sci, 9: e218. . Based on a recent study, 78 major US cancer centers that conduct 94 percent of all cancer clinical trials are located in areas that are socioeconomically more affluent and have higher proportions of White individuals compared to the national average (612)Lee H, et al. (2024) JAMA Oncol, 10: 652. .
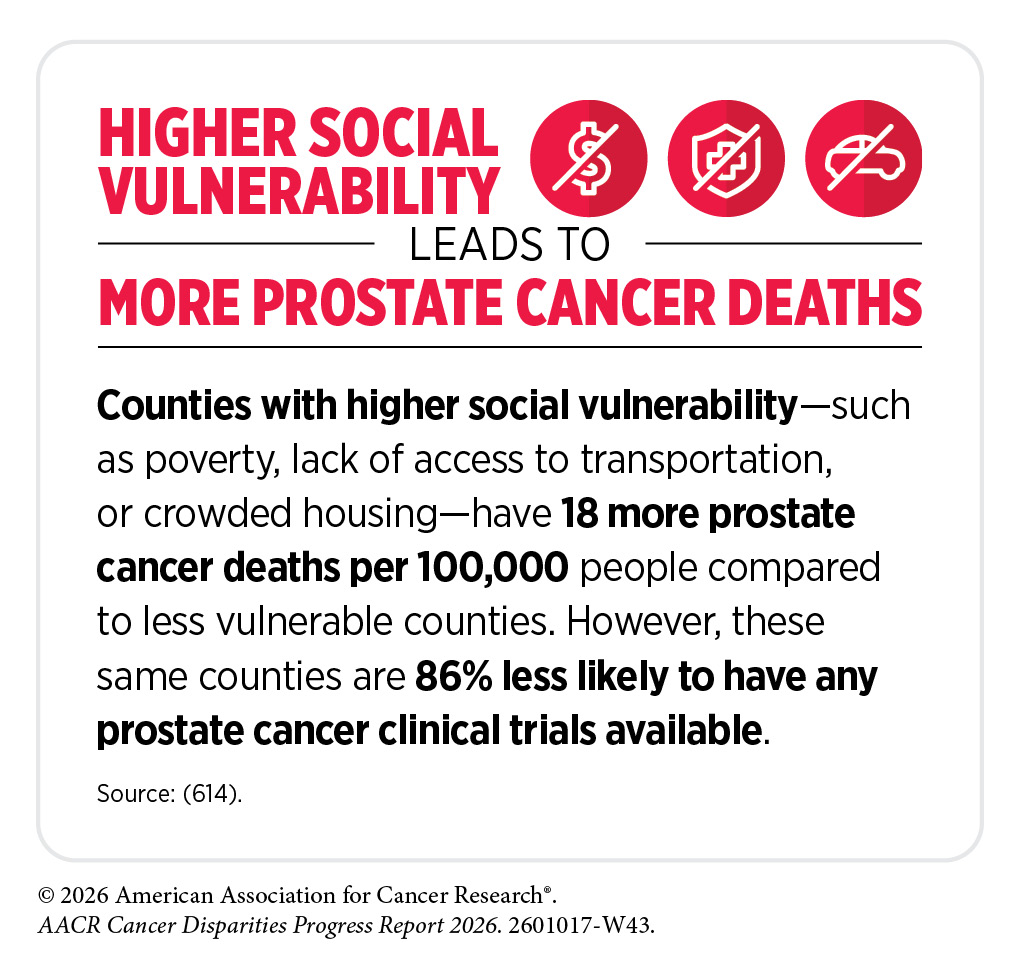
Patients in socioeconomically disadvantaged areas are less likely to participate in clinical studies, and these areas often have a higher proportion of racial and ethnic minority residents. One study showed that patients living in the most vulnerable neighborhoods, lacking education, transportation, and other neighborhood resources, were 20 percent less likely to participate in clinical trials and this association was stronger among Black patients (613)Perati SR, et al. (2025) J Natl Cancer Inst. . Factors related to structural and social drivers of health (SDOH), such as residential segregation, limited transportation, and language barriers, can explain much of the gap in participation between Black, Hispanic, and White patients with cancer (602)Guadamuz JS, et al. (2024) JNCI Cancer Spectr, 8. .
Overly restrictive eligibility criteria related to patient age, comorbidities, prior cancers, and ability to perform normal daily tasks are major barriers to clinical trial participation and disproportionally exclude medically underserved populations (615)Jin S, et al. (2017) J Clin Oncol, 35: 3745. . As one example, common eligibility criteria for phase II and III clinical trials differentially exclude Black patients from participating in pancreatic cancer clinical trials (616)Riner AN, et al. (2022) J Clin Oncol, 40: 2193. .
Stringency in criteria related to comorbidities often leads to exclusion of veteran and racial and ethnic minority patients from cancer studies. Research has shown that Black patients have higher rates of diabetes, human immunodeficiency virus (HIV) infection, and abnormal laboratory results than White patients; Hispanic patients have slightly higher rates of HIV infection and prior organ transplants than non-Hispanic patients; and older adult patients have more non-cancer coexisting health conditions than younger patients (603)Zhao Y, et al. (2025) Cancer, 131: e35944. .
Studies have shown that eligibility criteria do not vary much between different clinical trials for cancer therapies, suggesting that they may be carried from trial to trial without careful consideration of which comorbidities may actually pose a risk. Further, reference ranges for “normal” laboratory values may differ based on age, race, and ethnicity, which may enhance disparities in enrollment if these differences are not accounted for in eligibility criteria (617)Lim E, et al. (2015) Hawaii J Med Public Health, 74: 302. To address this issue, FDA proposes that clinical researchers provide a clear scientific rationale for each restriction in eligibility and review them as additional data become available. FDA also recommends accounting for disease-relevant changes to organ function. For instance, since liver dysfunction may be more prevalent among patients with liver cancer it should not preclude enrollment. However, despite FDA’s efforts to expand certain eligibility criteria to improve diversity in patient enrollment, compliance with revised criteria remains poor (618)Riner AN, et al. (2023) JNCI Cancer Spectr, 7. .
Gaps in ensuring broad awareness of clinical trials across the health care system disproportionately affect medically underserved populations, leading to lack of knowledge, misconceptions, medical mistrust, and concerns about randomization (597)Thapar R, et al. (2025) Proc (Bayl Univ Med Cent), 38: 929. . Encouragingly, recent findings demonstrate that when offered the opportunity, patients across racial and ethnic groups are equally likely to participate in clinical trials (601)Chen N, et al. (2025) JAMA Netw Open, 8: e2515205. . These findings align with and reinforce prior data showing patients with cancer from racial and ethnic minority backgrounds express a consistently high willingness to participate in clinical trials when they are asked (619)Unger JM (2025) JAMA Netw Open, 8: e2515210. . NCI-supported clinical trials are a critical component of the overall clinical research enterprise in the United States and play a vital role in the development of novel anticancer treatments. Researchers estimate that NCI-funded clinical trials over the past four decades contributed to 14 million additional years of life for cancer patients in the United States (620)Unger JM, et al. (2023) J Clin Oncol, 41: 2020. . NCI funding for clinical research has been critical in advancing our knowledge in key areas, such as palliative and supportive care and improving quality of life (see Integrating Supportive Care) (621)Abdou Y, et al. (2024) J Clin Oncol, 42: 3887. . NCI-supported clinical trials often investigate novel treatment approaches using existing therapies such as optimizing multimodality care, treatment sequencing, duration, and de-escalation or identifying appropriate standards of care treatments, which are critical research questions less likely to be prioritized by private sector–supported studies (622)George TJ, et al. (2025) J Natl Cancer Inst, 117: 1533. .
Unfortunately, enrollment in federally funded cancer clinical trials remained unchanged between 2008 and 2022, while enrollment in private sector–sponsored trials doubled (623)Unger JM, et al. (2024) J Clin Oncol, 42: 3917. . Although industry investment has accelerated the development of breakthrough cancer treatments, these data highlight the growing reliance on the private sector and concerning underinvestment in publicly sponsored research. It is also important to note that the cost of conducting clinical research is rising, driven by inflation and the increasing complexity of clinical trials, which often require advanced technologies and highly trained personnel.
Any reductions to NIH and NCI funding, particularly cuts to indirect cost support, threaten the infrastructure needed to conduct cancer clinical trials and may limit patient access to research, especially in community settings. There are additional concerns that the clinical research workforce is shrinking, with fewer clinicians pursuing or remaining in research careers due to funding uncertainty, workload pressures, and limited institutional support (577)Balogh EP, et al. (2025) JCO Oncol Pract, 21: 1746. . Robust federal funding for clinical research is vital to safeguard progress against cancer, ensure that these advances reach all populations, and support future clinical researchers.
Disparities in Outcomes in Pediatric and Adult Cancer Clinical Trials
Children with cancer are treated on a clinical trial when one is available, typically through the Children’s Oncology Group (COG). A higher proportion of children and adolescents with cancer, ranging from 20 percent to over 30 percent, depending on cancer type, participate in clinical trials in the United States, compared to only 7 percent of adult patients (623)Unger JM, et al. (2024) J Clin Oncol, 42: 3917. (624)Lupo PJ, et al. (2025) J Natl Cancer Inst, 117: 1868. . Enrollment of pediatric patients from racial and ethnic minority groups is also higher than that of adult patients (625)Fashoyin-Aje LA, et al. (2024) JAMA Oncol, 10: 380. (626)Faulk KE, et al. (2020) PLoS One, 15: e0230824. . However, a lack of diversity still exists in certain cancer studies (627)Wyatt KD, et al. (2024) JCO Oncol Pract, 20: 603. . For example, a retrospective analysis of clinical trial participation among children and adolescents with blood cancer showed that Black patients were 60 percent less likely to enroll than White patients (628)Monroe C, et al. (2025) Pediatr Blood Cancer, 72: e31641. . Additionally, there are challenges when parents use languages other than English (629)Santacroce SJ, et al. (2024) Pediatr Blood Cancer, 71: e31321. . A survey of COG–affiliated institutions found that limited translation resources, insufficient funding, and lack of interpreter access create significant barriers for these patients and family members (630)Beauchemin MP, et al. (2024) JNCI Cancer Spectr, 8. .
Research increasingly shows that children from low-income families and those who are Black or Hispanic experience higher relapse and mortality rates even when treated on clinical trials and receiving care at major academic centers. An analysis of 935 children with high-risk neuroblastoma—the most common pediatric solid tumor that is not a brain tumor—found that Black children had a 54 percent higher risk of death and Hispanic children had a 63 percent higher risk of death compared to White children, despite all being enrolled in a clinical trial (631)Umaretiya PJ, et al. (2025) JAMA Netw Open, 8: e2458531. . Emerging evidence suggests that differences in treatment-related toxicity, particularly among Hispanic children, may represent one modifiable mechanism contributing to persistent disparities in outcomes in clinical trials (632)Shoag J, et al. (2024) Pediatr Blood Cancer, 71: e31192. .
Similar disparities in outcomes have also been observed in adult clinical trials with research showing that cancer patients from medically underserved populations experience worse outcomes. As one example, in phase II and III cancer clinical trials conducted between 1985 and 2012, participants from the most disadvantaged areas had a 28 percent higher risk of death, compared to those from the most affluent areas (633)Unger JM, et al. (2021) J Clin Oncol, 39: 1339. . Another study showed that among patients with breast cancer who participated in clinical trials, young Black and Hispanic patients experienced worse outcomes, compared to their White counterparts (634)Lipsyc-Sharf M, et al. (2023) JAMA Netw Open, 6: e2339584. .
These findings indicate that structural and social drivers of health may continue to influence survival even in a controlled clinical trial setting. Additionally, there may be potential contributions of differences in cancer biology as well as other biologic predictors of toxicity, treatment resistance, differences in drug metabolism, and other factors independent of patient socioeconomics. These data further highlight the need for clinical trials to be representative of all patient populations.
Facilitating Equity in Clinical Cancer Research
Overcoming barriers to clinical trial participation and disparities in clinical trial outcomes will require coordinated action across all stakeholders from academia, the biopharmaceutical industry, nonprofit organizations, and federal agencies. Research has identified numerous facilitators that enhance participation of patients from diverse backgrounds. These include physicians’ recommendations to enroll, education and awareness of trials among patients and providers, implementation of remote technologies and other approaches to reduce the need to travel to a trial site. All sectors must work together to build on these strategies to design and implement evidence-based interventions that facilitate clinical trial enrollment. Such approaches must focus on improving patient and provider education, building trust within communities, strengthening partnerships between large cancer centers and community hospitals, enhancing clinical trial infrastructure and the research workforce, and ensuring transparent reporting of race and ethnicity in clinical trial publications.
Concurrently, coordinated efforts to identify mechanisms underlying differences in cancer biology and disparities in toxicity, relapse, and survival are essential to achieve equity in cancer outcomes for clinical trial participants. Integrating social care along with clinical care to address unmet socioeconomic and psychosocial needs of patients is key to improving care delivery and outcomes for all patients participating in clinical trials (635)Tucker-Seeley R, et al. (2024) JCO Oncol Pract, 20: 621. . Although challenges in measuring and addressing SDOH are well documented, overcoming these barriers is critical to ensure that all patients benefit from the unprecedented advances that are being made in clinical cancer research.
Community Engagement and Patient Navigation
Research has shown that community outreach and patient navigation can enhance awareness of clinical trials and increase participation of racial and ethnic minority patients (637)Nouvini R, et al. (2022) Cancer, 128: 3860. (638)Guerra CE, et al. Journal of Clinical Oncology, 39: 100. . Clinical researchers and institutions must implement strategies to include community-based partners in the design and execution of clinical trials and integrate patient and community feedback into clinical research design. These efforts can build trust and credibility and facilitate relationship building and bidirectional communication, especially for populations that experience systemic injustices and discrimination and do not trust the clinical system. Community engagement is particularly important for the inclusion of patients from racial and ethnic minority groups, including Indigenous populations and Tribal Nations, as well as those from SGM populations.
One multilevel intervention currently being evaluated involves the implementation of Community Advisory Boards, deploying health navigators, creating culturally sensitive research spaces, building community-partnered training pipelines, enhancing staff training, assessing community trust, and supporting pilot projects to determine success (639)Taylor S, et al. (2025) J Clin Transl Sci, 9: e156. (640)Muhigaba PB, et al. (2025) J Clin Transl Sci, 9: e221. . Over time, this effort aims to increase the diversity of clinical trial participants and the research workforce while strengthening community trust in research, ultimately contributing to reductions in cancer disparities.
In building on these efforts, it is also critical to train the clinical research workforce in the science of community outreach and engagement so that investigators are better equipped to recruit and retain diverse participants in clinical trials. Early data from the Robert A. Winn Excellence in Clinical Trials Award Program, an initiative designed to address this need, indicate that structured training and mentorship can help early-career investigators effectively incorporate community-engaged approaches into clinical research. As reported recently, the program has begun to show promising impact, including better recruitment of underrepresented patients in clinical trials that are conducted by Program graduates, when compared to industry trials and national averages (641)Becker M, et al. (2025) Cancer Epidemiology, Biomarkers & Prevention, 34: B094. . Although these findings are preliminary, they highlight the potential of workforce training in community outreach and engagement to advance equity in clinical trial participation.
Clinical institutions, sponsors, and researchers must support an infrastructure that sustains long-standing partnerships with communities, patients, and patient advocates. Maintaining ongoing communication with the communities they serve and disseminating clinical trial results back to those communities are also critical. Policies that integrate community-based clinical partners, such as local health care providers including primary care physicians, who may not traditionally participate in research, can further improve access to studies at the population level in underserved areas.
Engaging primary care physicians may be one approach to increasing participation and diversity in clinical trials. Strengthening partnerships between primary care providers and cancer research specialists can help determine whether patients are appropriate candidates for clinical trials, particularly prevention and screening-focused studies, and facilitate timely referrals. As the landscape of cancer clinical trials continues to evolve, it is essential for primary care providers to remain informed. By dispelling misconceptions, addressing barriers, and staying current with emerging developments, primary care providers can play a pivotal role in guiding patients toward appropriate clinical trial options.
A new report from the National Academies of Sciences, Engineering, and Medicine emphasizes that communities are central to achieving health equity, noting that all aspects of health systems ultimately intersect within communities and that effective, equitable care depends on approaches such as community-based and community-engaged research and the use of interprofessional teams that include community health workers who can tailor services to local needs (642)National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Board on Population Health and Public Health Practice; Board on Health Care Services; Committee on Unequal Treatment Revisited: The Current State of Racial and Ethnic Disparities in Health Care. Ending Unequal Treatment: Strategies to Achieve Equitable Health Care and Optimal Health for All. Nass SJ, Amankwah FK, DeVoe JE, Benjamin GC, editors. Washington (DC): National Academies Press (US); 2024 Aug 23. PMID: 38924457. The report underscores that health systems must be accountable to the communities they serve, drawing on community partnerships to shape priorities, guide interventions, and ensure sustainable progress toward eliminating racial and ethnic health care inequities.
Patient navigators can provide social, emotional, financial, and logistical support and act as a potential facilitating factor for clinical trial participation. Research has shown that patient navigation programs to improve enrollment and retention of diverse patients in trials are feasible to implement, are highly acceptable to patients, and can reach patient populations generally underrepresented in cancer clinical trials (643)Makhnoon S, et al. (2025) Cancer Med, 14: e71125. . A study of women with gynecologic cancers found that a dedicated research navigator team who approached and discussed potential trials with patients improved overall participation in clinical trials, particularly among underrepresented groups (644)Boitano TKL, et al. (2025) Int J Gynecol Cancer, 35: 100066. . As a result, enrollment of patients from racial minority populations increased from 12.5 percent to 35.3 percent.
Improving survival for all patients in cancer clinical trials will require systematically collecting data on SDOH; using this information to better tailor treatment and supportive care; and testing interventions that address adverse SDOH, including poverty, food insecurity, housing insecurity, and transportation barriers during and after the clinical trial. Emerging data indicate that collecting patient-reported SDOH data in clinical trials is feasible and acceptable by patients (230)Monge C, et al. (2025) Cancers (Basel), 17. . By addressing the various socioeconomic needs of participants, patient navigation may reduce the inequities in clinical trial outcomes.
Addressing System-level and Structural Barriers
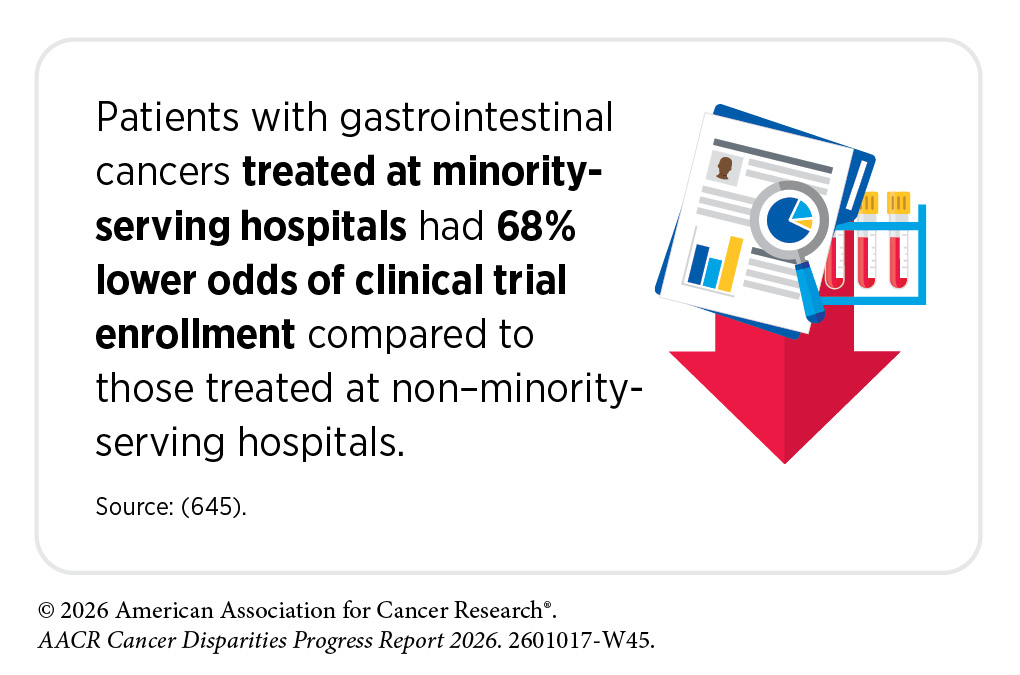
While certain system-level barriers to clinical trial participation may require long-term strategies and policy changes, some could be addressed in the short term. One immediate approach could be to conduct clinical trials at facilities that treat a high percentage of minority and medically underserved patient populations. Currently, many late-phase clinical trials are conducted outside the United States attributable, in part, to challenges related to trial design and regulatory expectations, and those within the United States are often limited to the high-volume cancer centers—facilities that treat higher numbers of patients, have specialty surgeons, and perform greater numbers of procedures. It is, therefore, crucial that clinical studies be available to patients at Minority-Serving Institutions (MSIs) including safety-net hospitals, which often operate in inner-city communities and provide a larger share of care to low-income, minority, and uninsured populations.
Partnerships between large academic hospitals and community cancer centers have been proposed as a strategy to improve access for underrepresented patient groups. As one example of success, a community-academic partnership that implemented targeted strategies at both the practice and provider levels increased clinical trial enrollment at the community-based sites (646)Ledesma Vicioso N, et al. (2022) JCO Oncol Pract, 18: e780. . Hispanic representation in these trials ranged from 12 percent to 36 percent, compared to just 4 percent to 6 percent in trials limited to the academic center. Partnership efforts are underway across the VHA health systems to expand trial availability, improve referral pathways, and address logistical barriers to increase veteran access to cancer clinical trials.
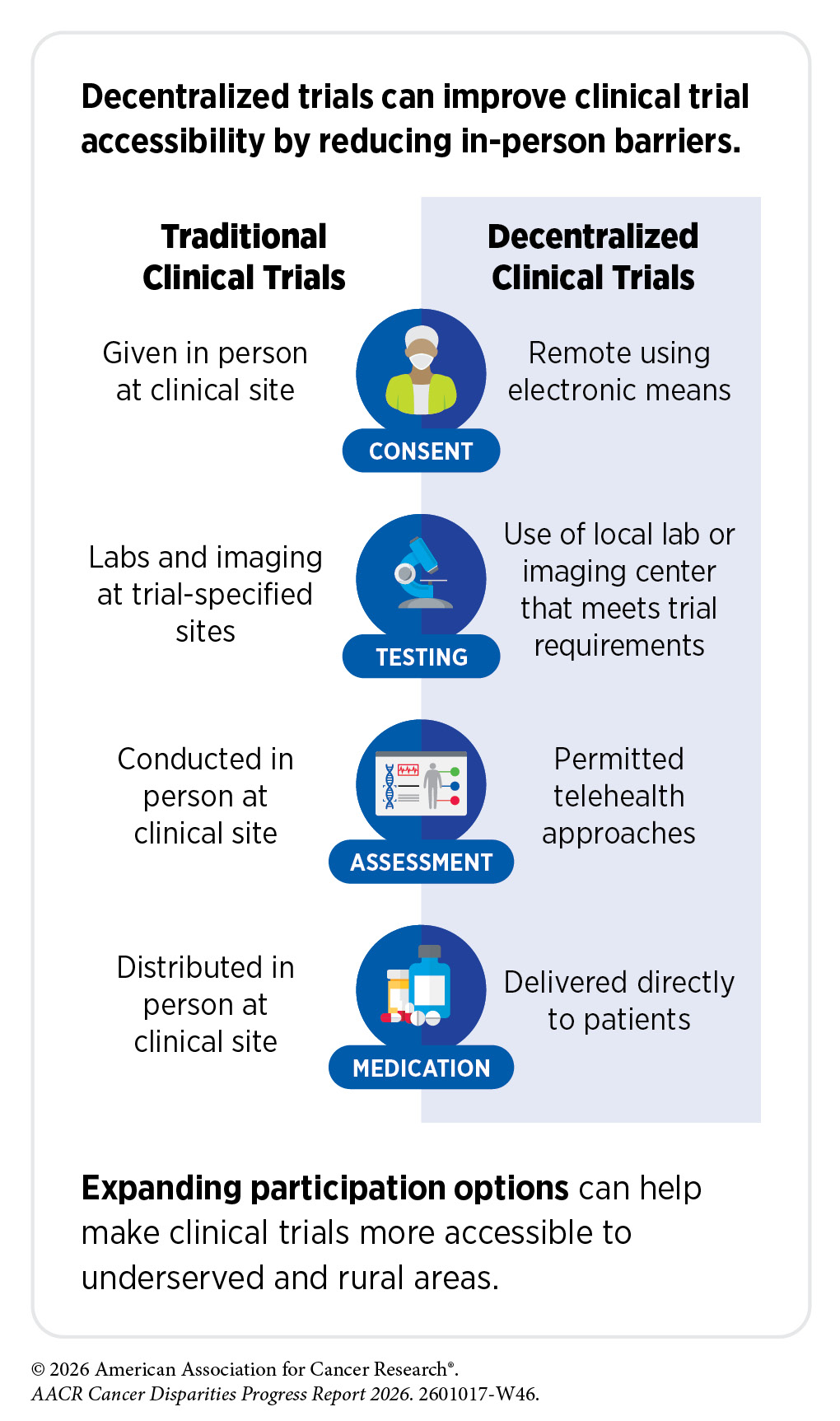
The COVID-19 pandemic, despite its adverse effects on all aspects of cancer research and patient care, forced researchers to decentralize certain aspects of clinical trials so that lifesaving therapeutics could be brought quickly to as many patients as possible (647)American Association for Cancer Research. AACR Report on the Impact of COVID-19 on Cancer Research and Patient Care. Accessed: March 31, 2026. . Adaptations implemented during the pandemic, including consenting patients remotely, permitting telehealth for routine clinical assessments, delivering experimental drugs to patients, and allowing the use of local laboratory, imaging facilities, or community health centers accessible to patients, offered a blueprint to further reform clinical trials. It is, therefore, not surprising that the number of decentralized trials rose sharply beginning in 2020, following only modest growth from 1998 to 2019 (648)Aiyegbusi OL, et al. (2024) Nat Med, 30: 3075. .
Emerging data indicate that decentralized approaches are feasible and can improve outcomes for patients. As an example, an academic cancer center–led initiative in North Carolina demonstrated that a hybrid decentralized approach is feasible in community settings, with success driven by motivated local champions, supportive leadership, and infrastructure for remote visits (649)Morrison JK, et al. (2026) The Oncologist: oyag118. . In another study, a supportive care clinical trial that involved partnerships between leading academic centers and community health centers reduced early deaths in patients with acute promyelocytic leukemia (APL), from an expected 30 percent to just 3 percent, across all care settings (650)Jillella AP, et al. (2025) JAMA Oncol, 11: 400. . Patients at community centers were treated locally using a consensus treatment plan developed through collaboration between the community oncologist and one of seven APL experts available from six leading academic centers.
Ongoing research must continue to evaluate the impact of decentralized approaches on advancing clinical research and improving patient outcomes. It is important to rigorously examine whether decentralized clinical trials can ensure access to trial participation for all population groups to avoid widening existing disparities.
Clinical trial infrastructures must also be set up to address social needs and alleviate common barriers such as food and housing insecurity, out-of-pocket costs, time off from work, and child and elder care. To encourage patients with cancer to participate in clinical studies, research teams need to engage with minority patient populations. Federal funding is critical to support infrastructures that enhance the accrual of minority patients on clinical trials. The NCI Community Oncology Research Program (NCORP) is one example of federal efforts to reduce structural barriers for patients. NCORP is a national network successfully bringing cancer clinical trials and care delivery studies to people in their own communities in diverse settings. The program focuses on increasing clinical trial participation by addressing the structural and social drivers of disparities and evaluating differential outcomes in racial and ethnic minority groups and other medically underserved populations.
A key strategy to diversify clinical trial participation is to simplify and broaden eligibility criteria. These criteria should keep pace with scientific innovation; be pragmatic, inclusive, and informed by real-world evidence; and allow flexibility for patients with clinical or functional limitations. If anticancer therapies are intended for use in a broad patient population after approval, they should be evaluated in diverse populations, including those with coexisting medical conditions.
In this regard, researchers using a large nationwide health record dataset demonstrated that under typical strict eligibility criteria, only about half of cancer patients would qualify for participation in clinical trials (651)Kaur M, et al. (2024) NEJM Evid, 3: EVIDoa2300236. . Patients who were older than 75, from racial and ethnic minority populations, and of low socioeconomic backgrounds were more likely to be excluded. Broadening criteria increased the number of eligible patients by 78 percent, with the greatest gains observed among older, Black, and socioeconomically disadvantaged patients (651)Kaur M, et al. (2024) NEJM Evid, 3: EVIDoa2300236. . Notably, a precision medicine clinical trial that evaluated the impact of protocol exceptions that allowed patients who did not meet standard eligibility criteria to participate, found no significant differences in safety or clinical benefit between those patients and trial-eligible participants, suggesting that more flexible trial designs can safely expand access (652)van Berge Henegouwen JM, et al. (2024) Clin Cancer Res, 30: 3937. .
Future interventions to improve clinical trial accessibility should also enhance and improve data collection, leverage AI, digital technologies, and patient-reported outcomes (PROs), and strengthen patient–provider communication. PROs can support and facilitate recruitment, especially among underserved populations. In a clinical trial evaluating an intervention for cancer-related fatigue, inviting eligible patients screened through PROs using portal messages led to 20.0 percent enrollment, compared to zero enrollment through standard of care (653)Verdini NP, et al. (2024) JAMA Oncol, 10: 784. . Harnessing AI and machine learning trained on diverse datasets has the potential to improve clinical trials. Researchers are evaluating whether AI can be leveraged to increase clinical trial participation and diversity by improving patient matching, identifying underserved populations, and streamlining recruitment processes (654)Abbidi SR, et al. (2026) Trials, 27. (655)Chow R, et al. (2023) J Natl Cancer Inst, 115: 365. (656)Gong G, et al. (2026) JCO Clin Cancer Inform, 10: e2500262. .
Improving health care coverage through public health policies and fostering greater representation of all populations within the clinical research workforce are vital for future progress in clinical trials (see Disparities in the Cancer Training Pathway and Cancer Research and Care Workforce). Based on recent data, while Medicaid expansion was not associated with a significant increase in the proportion of Black or Hispanic patients in cancer clinical trials, it was associated with an increase specifically in states that mandated coverage of the routine costs of trial participation (657)Schpero WL, et al. (2024) J Clin Oncol, 42: 3238. . A representative workforce that reflects the populations it serves is critical, as studies show that racial concordance between patients and providers can improve communication, build trust, and increase adherence to care, which may ultimately lead to better outcomes (658)Montano-Campos JF, et al. (2026) J Natl Compr Canc Netw, 24. (659)Loeb S, et al. (2023) JAMA Netw Open, 6: e2324395. (660)Kuri L, et al. (2023) Clin Trials, 20: 585. .
Disparities in Cancer Treatment
The dedicated efforts of individuals working throughout the medical research cycle are constantly translating new research discoveries into advances in cancer treatment that are improving survival and quality of life for people in the United States and around the world. Much of the recent progress, including many new cancer treatments approved by FDA, was highlighted in AACR Cancer Progress Report 2025 and AACR Pediatric Cancer Progress Report 2025 (274)American Association for Cancer Research. AACR Cancer Progress Report 2025. Accessed: March 31, 2026. (563)American Association for Cancer Research. AACR Pediatric Cancer Progress Report 2025. Accessed: March 17, 2026. .
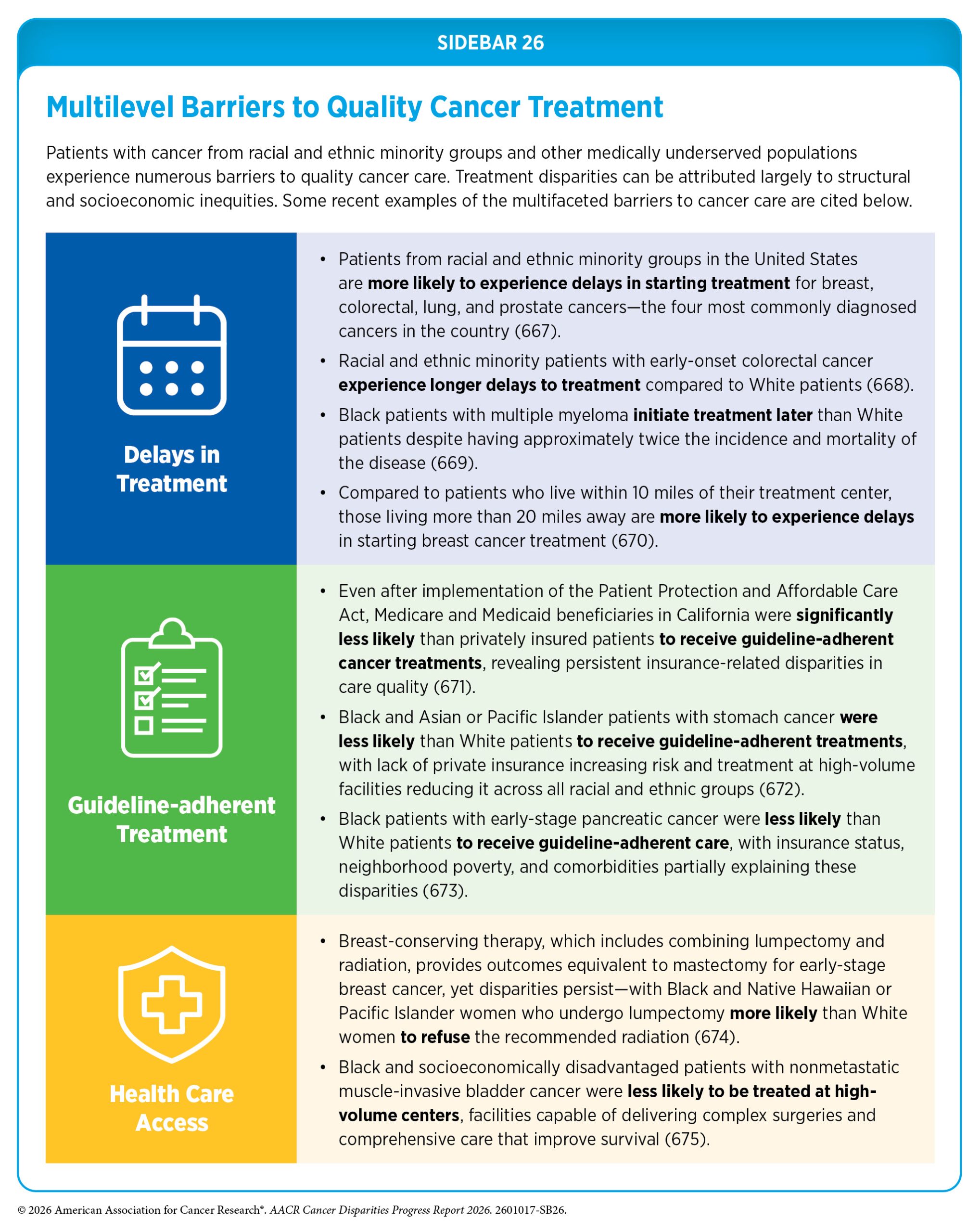
Despite recent advances in cancer treatment, racial and ethnic minority groups and other medically underserved populations continue to experience more frequent and higher severity of multilevel barriers to quality cancer treatment, including treatment delays, lack of access to guideline-adherent curative treatment, undertreatment, refusal or early termination of treatment, treatment receipt at low-volume and community settings rather than comprehensive cancer centers, and higher rates of treatment-related and/or financial toxicities (see Sidebar 26). Disparities in treatment persist across the cancer care continuum, with racial and ethnic minority patients more likely to receive poorer quality end-of-life care (see Integrating Supportive Care). Barriers to quality cancer treatments are compounded for patients living in remote or rural areas (such as Native American populations), those located outside the mainland United States, as well as those who lack health literacy or have language barriers (661)Moen EL, et al. (2025) JAMA Netw Open, 8: e2461021. (662)Leonis R, et al. (2025) Am Surg, 91: 746. (663)Nguyen A, et al. (2025) J Surg Oncol, 131: 1002. .
Based on a recent study that analyzed health care utilization among patients with early-stage NSCLC from 2005 to 2019, Black patients had significantly lower rates of receiving curative therapy compared to White patients (664)Lynch OF, et al. (2026) JAMA Netw Open, 9: e2559845. . In another study of more than 3,000 patients with metastatic HER2-positive breast cancer, those who were older and Black were less likely to receive personalized treatments, despite the substantial survival benefits associated with these treatments (665)Ajjawi I, et al. (2025) Cancers (Basel), 17. . Additionally, rural patients with early-stage genitourinary (kidney, bladder, and prostate) cancers were less likely to receive recommended care despite clear treatment guidelines, highlighting the need for better access to surgery, radiation, and coordinated care to reduce these disparities (666)Dirican CD, et al. (2026) Urologic Oncology: Seminars and Original Investigations: 111088. .
Many of the disparities in cancer treatment can be attributed to structural and social drivers, including systemic injustice, limited access to health care facilities, high costs of cancer care, low income, and lack of health insurance (see Understanding and Addressing Drivers of Cancer Disparities). For example, Black patients living in communities that experience higher structural racism—measured by gaps in housing, education, income, and health care—are more likely to experience delays in initiating breast cancer treatment (676)Reeder-Hayes KE, et al. (2024) J Clin Oncol, 42: 3858. . Similarly, breast cancer patients who are older and living in historically redlined neighborhoods are less likely to receive guideline-adherent treatments (677)Yen TWF, et al. (2025) Breast Cancer Res Treat, 215: 40. . Patients treated for colorectal, breast, gastric, and pancreatic cancers at hospitals serving lower-income populations have significantly worse 5-year survival than those at higher-income-serving hospitals, highlighting how both patient- and facility-level socioeconomic factors compound disparities in cancer outcomes (678)Manisundaram NV, et al. (2025) Ann Surg Oncol, 32: 6807. . Additionally, unmet social needs—particularly challenges related to transportation, housing stability, legal assistance, and caregiving responsibilities—are significantly associated with delays in treatment initiation (679)Zhang FG, et al. (2024) JCO Oncology Practice, 20: 1733. .
Rural US counties have far fewer oncologists compared to urban counties (680)Crowley RJ, et al. (2026) J Cancer Policy, 47: 100704. . Research shows that compared to patients living in urban areas, rural patients are two to four times more likely to cross state lines for surgery, radiotherapy, and chemotherapy (661)Moen EL, et al. (2025) JAMA Netw Open, 8: e2461021. . Similarly, NHPI patients with breast cancer face substantial cancer treatment disparities, including lower likelihood of breast reconstruction after removal, more frequent surgical delays, and higher radiation therapy refusal, driven by geographic isolation, limited access to specialized care, and cultural perceptions, which together increase their risk of mortality (663)Nguyen A, et al. (2025) J Surg Oncol, 131: 1002. .

Receiving health care from a provider who is of the same race and/or ethnicity or speaks the same language as the patient, can improve patient satisfaction and quality of care, as highlighted in the cancer journey of Vanessa Bañuelos. One study showed that among patients with chronic myeloid leukemia, shared identity with clinicians influenced long-term treatment adherence, albeit the effects differed by clinician type: Patient–oncologist race, ethnicity, and gender concordance was associated with modestly higher adherence to personalized treatments, while patient–primary care physician concordance, particularly with historically disadvantaged patients, was linked to higher adherence to guideline-recommended biomarker testing (658)Montano-Campos JF, et al. (2026) J Natl Compr Canc Netw, 24. (681)Montano-Campos JF, et al. (2025) JAMA Netw Open, 8: e258039. . However, fewer individuals from racial and ethnic minority groups report having the same race and/or ethnicity or language preference as their provider (682)KFF. Survey on Racism, Discrimination and Health: Experiences and Impacts Across Racial and Ethnic Groups. Accessed: . This is attributable, in large part, to the lack of diversity in the cancer science and medicine workforce (see Disparities in the Cancer Training Pathway and Cancer Research and Care Workforce).
Several US states, particularly large, diverse states such as California, Texas, New York, Florida, and New Jersey, have populations in which over 10 percent of residents have limited English proficiency, emphasizing the scale of language-related barriers in cancer care (561)Kim HS, et al. (2025) BJC Rep, 3: 80. . Patients with limited English proficiency face major challenges, including inconsistent and difficult communication with the health care system, delays in diagnosis and treatment, and lower treatment adherence. Evidence shows that professional interpreter services, language-concordant care, and culturally tailored communication can significantly improve cancer care quality.
Dissatisfaction with their health care due to experiences of discrimination and cultural incompetency is a major barrier for patients from SGM populations and often leads to avoidance of care. Based on a recent report, SGM cancer survivors and caregivers experience “minority stress,” which is described as the fear of discrimination or substandard care, while culturally humble, inclusive, and patient-centered provider practices, such as affirming communication, visible inclusivity, and tailored resources, are essential to improving cancer care experiences and outcomes for this population (683)Insalaco ME, et al. (2026) Oncologist, 31. . Data from the All of Us Research Program show substantial heterogeneity within SGM cancer survivors, with bisexual and transgender/gender-expansive individuals facing the greatest structural and psychosocial barriers to care, including cost-related delays, discrimination, and stress, highlighting the need for targeted, data-driven interventions to reduce inequities within this population (see Challenges Faced by Cancer Survivors)(684)Brown-Savita M, et al. (2026) Cancers (Basel), 18. .
It should be noted that patients with intersectional identities often face multilevel barriers to cancer care that adversely affect screening, diagnosis, treatment, and survivorship. Therefore, additional research is needed to better understand how intersecting factors, such as geography, race and ethnicity, socioeconomic status, sexual orientation, and gender identity, may contribute to disparities in cancer treatment, and mitigate these inequities through reducing structural and interpersonal biases, improving access to care, and implementing evidence-based interventions.
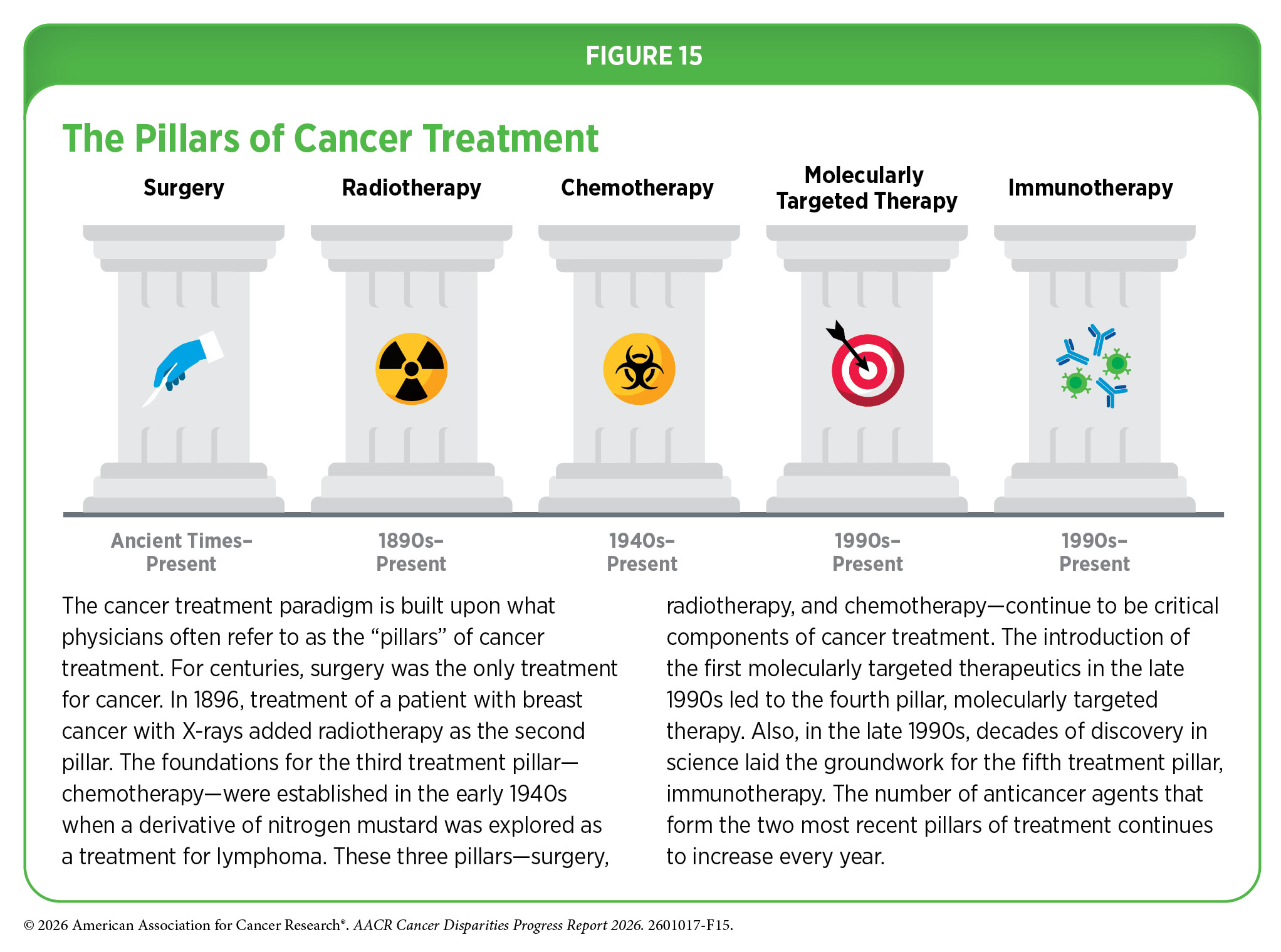
In the following sections, we highlight recently documented disparities among cancer patients in the use of the main pillars of cancer treatment (see Figure 15), and emphasize areas where advances have been made in achieving equity in cancer treatment. Importantly, several recent studies have pointed out that disparities in the receipt of care, as well as outcomes for many cancers, can be eliminated if every patient has equitable access to quality health care services.
Treatment With Surgery
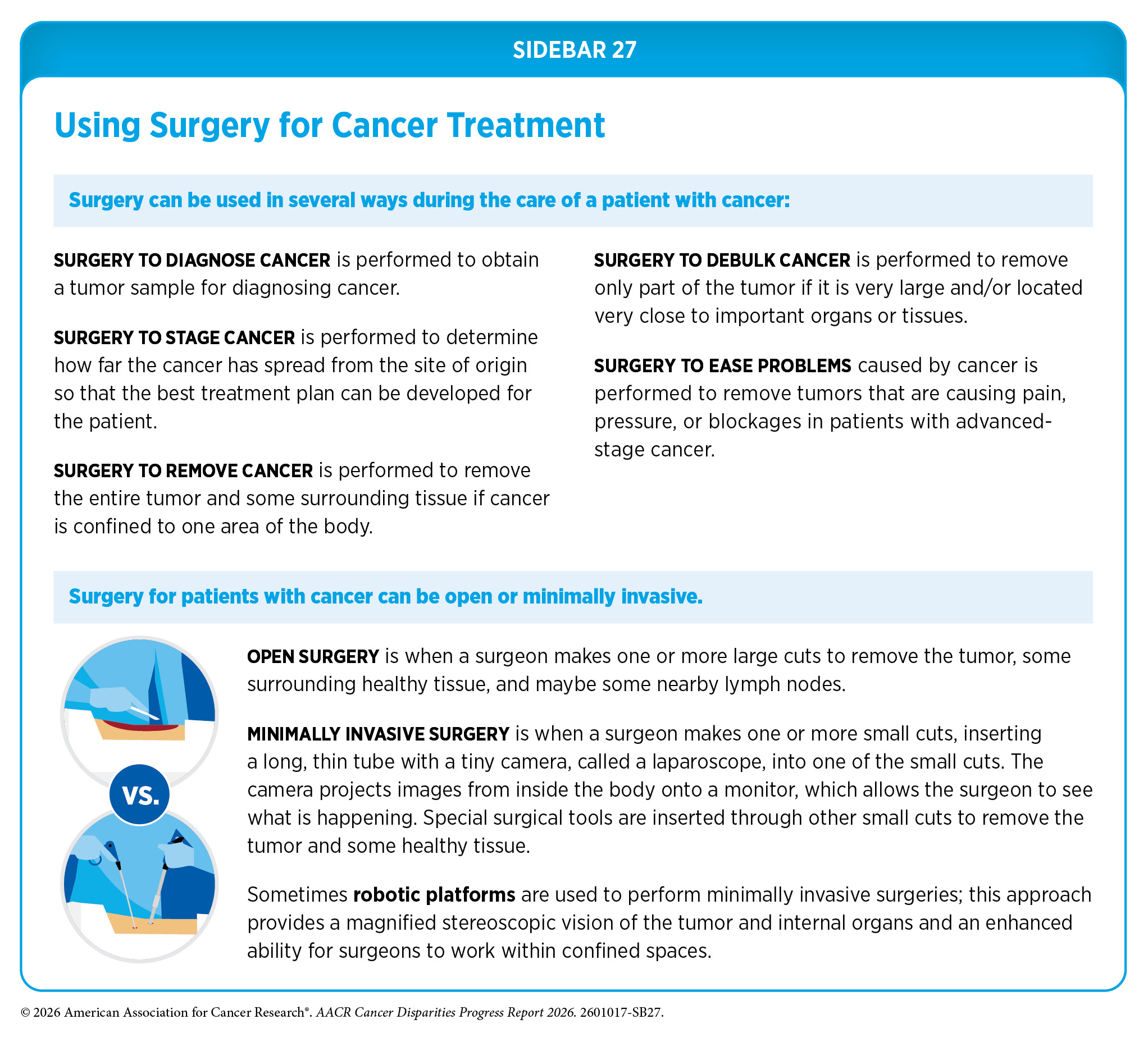
For centuries, surgery was the only way to treat cancer. Today, surgery remains the foundation of curative care for many cancer types, including those with pronounced disparities in morbidity and mortality among racial and ethnic minority groups and other medically underserved populations. Surgery is used in several ways during the care of a patient with cancer (see Sidebar 27).
For cancers associated with high mortality, such as lung, liver, and pancreatic cancers, surgical resection is key to survival when these tumors are detected at an early stage. For cancers with better prognosis, specialty surgeries are necessary to optimize quality of life after the treatment, such as minimally invasive surgery for gastrointestinal cancers, reconstruction surgery for certain breast cancer patients requiring mastectomy, and sphincter-preserving surgery for rectal cancer patients. Researchers are continuously innovating new and improved strategies to maximize benefit and minimize harm from surgery.
Sometimes, additional therapy is given before, after, or around the time of surgery based on the specific features of a patient’s tumor (see Sidebar 28). Researchers have found that this approach not only improves the surgeon’s ability to remove the tumor (e.g., by shrinking the tumor when given before the surgery) but also increases the patient’s overall survival and/or quality of life (685)Burotto M, et al. (2019) Semin Oncol, 46: 83. .
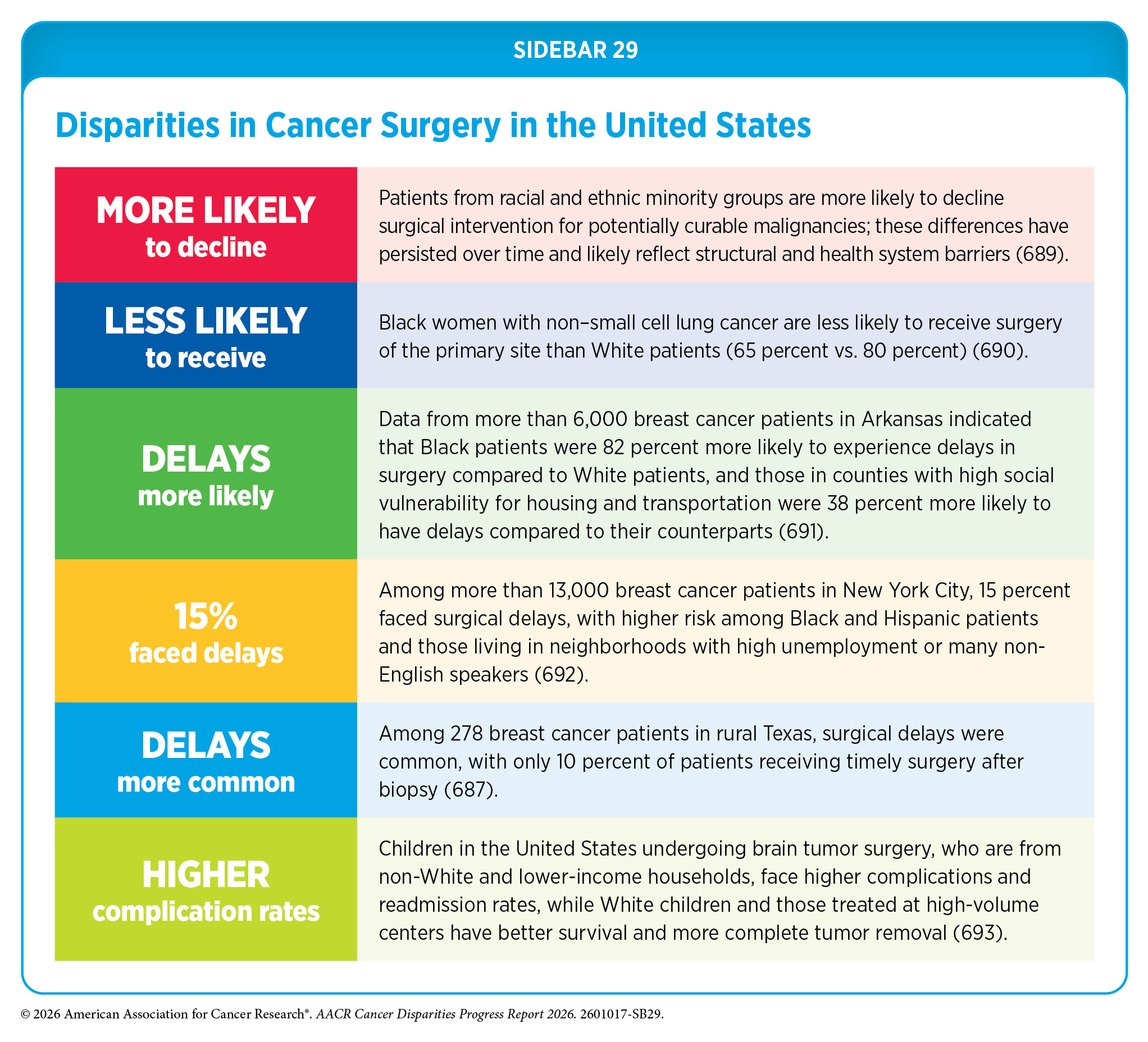
Disparities in surgical management of cancer, including treatment delays, forgoing potentially curative cancer surgery, and non-adherence to guideline-recommended surgery, are experienced by many populations (see Sidebar 29). These disparities, driven by structural and social factors, are seen across cancer types, including the most diagnosed cancers in the United States, and contribute to worse outcomes. As one example, striking disparities exist in the surgical treatment for breast cancer, the most common cancer in US women. Surgery is the first line of treatment for most patients with early-stage breast cancer, and treatment initiation longer than 60 days after diagnosis is associated with worse survival (686)De Jesus EM, et al. (2025) Ann Surg Oncol, 32: 8621. .
Evidence shows persistent disparities in time to breast cancer surgery, surgical outcomes, and postoperative complication rates. Factors associated with these disparities include low socioeconomic status, lack of private insurance, greater distance to health care facilities, and being from a racial or ethnic minority population. For example, Black and Hispanic patients with breast cancer are at higher risk than White patients to experience treatment delays longer than 60 days (686)De Jesus EM, et al. (2025) Ann Surg Oncol, 32: 8621. . NHPI women with breast cancer are 4.5 times more likely to experience treatment delays and twice less likely to receive reconstruction surgery after mastectomy, compared to White women (663)Nguyen A, et al. (2025) J Surg Oncol, 131: 1002. . Geographic isolation and limited access to specialty care as well as cultural perceptions surrounding treatments contribute to these disparities. Residence in rural areas and being farther away from health care facilities are also associated with delays in surgical care (670)Wang Y, et al. (2025) Cancer Med, 14: e71354. (687)Orsi C, et al. (2025) Ann Surg Oncol, 32: 4883. .
Where patients receive care can contribute to breast cancer disparities. Among patients receiving neoadjuvant chemotherapy, rates of mastectomy and breast reconstruction surgery immediately after mastectomy can vary significantly (688)Keane CA, et al. (2026) Clin Breast Cancer, 26: 45. . Analysis from a safety-net hospital, which primarily serves underserved populations, showed that surgical and reconstruction rates were lower compared to non-safety net hospitals and similar across all racial groups, whereas at a tertiary care center with specialized, high-resource services, White women were more likely to undergo double mastectomy with reconstruction, highlighting how institutional setting can perpetuate treatment disparities.
Research consistently demonstrates significant disparities in surgical care for early-stage NSCLC, the most common type of lung cancer in the United States. Based on a recent study, among Medicare beneficiaries, Black patients had persistently lower rates of receiving curative surgical treatment from 2005 to 2019, compared to White patients (664)Lynch OF, et al. (2026) JAMA Netw Open, 9: e2559845. . Analysis of a large national cancer database demonstrated that sociodemographic factors, such as Black race, lack of insurance, lower income, and lower educational status, were associated with delays to definitive lung cancer surgery, and patients with delayed surgery were more likely to have cancer that was more advanced than initially expected and increased mortality (694)Stuart CM, et al. (2025) Ann Thorac Surg, 119: 1082. . Lack of a robust surgical workforce also contributes to disparities. According to one study, recent declines in the US cardiothoracic surgery workforce may have led to significantly fewer patients undergoing guideline-adherent surgery for early-stage NSCLC and worsening disparities in survival (695)Potter AL, et al. (2024) J Thorac Cardiovasc Surg, 167: 1603. . Researchers estimate that in the United States by 2036, there will be a shortage of between 10,100 and 19,900 surgical specialists (696)Association of American Medical Colleges. The Complexities of Physician Supply and Demand: Projections From 2021 to 2036 Summary Report. Accessed: March 31, 2026. .
Minimally invasive surgeries, such as robotic surgeries, that are performed by highly specialized surgeons may reduce complications during and after surgery and improve quality of life post procedure. Disparities in lung cancer surgery also extend to the surgical approach: Patients from lower-income areas and those treated outside high-resource academic centers are less likely to receive minimally invasive surgeries, such as video-assisted or robot-assisted resection, highlighting how both social drivers and facility characteristics shape access to optimal surgical care (697)Karanth SD, et al. (2026) Cancers (Basel), 18. .
Research similarly demonstrates significant disparities in surgical care for colorectal cancer. A recent population-level study found that structural and social factors, including race and socioeconomic status, are associated with disparities in access to timely and appropriate surgical treatment (698)Doshi RH, et al. (2026) Public Health, 252: 106091. . Higher likelihood of delays occurred among patients who were Black, AIAN, Asian, and Medicaid-insured. Research also shows lower uptake of minimally invasive surgery in minority, rural, and uninsured patients (699)Emile SH, et al. (2025) Am Surg, 91: 528. . Up to one-quarter of colorectal cancer patients present with liver metastases at the time of diagnosis, and about half experience them over time. Although liver surgery or ablation can be curative, access is unequal. According to a new analysis among more than 72,000 colorectal cancer patients with liver metastases, only 18 percent received these treatments, with lower rates among Black and Hispanic patients, uninsured individuals, and those with lower income. Patients treated at academic centers were more than twice as likely to receive these treatments as those treated at community cancer programs (700)Martinez AE, et al. (2026) Ann Surg Oncol. .
Surgery can have lasting side effects, and researchers are evaluating evidence-based alternatives for certain patients. As one example, men with slow-growing prostate cancer may never experience problems during their lifetime. Research has shown that careful observation of disease in these patients, referred to as watchful waiting or active monitoring, is a safe alternative to receiving immediate surgery or radiotherapy (701)Hamdy FC, et al. (2023) N Engl J Med, 388: 1547. (702)Newcomb LF, et al. (2024) JAMA, 331: 2084. . These findings are important because active monitoring can allow patients to avoid treatment-related adverse effects, such as sexual and incontinence problems. However, recent data indicate that disparities persist in active monitoring, with Black men experiencing less adequate follow-up during monitoring and worse prostate cancer–specific mortality compared to White men (703)Finocchiaro A, et al. (2025) J Racial Ethn Health Disparities. .
Surgery is a key component of pancreatic cancer treatment. Guideline-adherent surgery can improve 5-year survival for patients with early-stage disease, yet adherence to guidelines remains low. Unfortunately, numerous disparities in access to surgical resection have been reported. According to a recent review, patients who are Black or Hispanic, are older adults, and are of low socioeconomic status, treated at community hospitals, and not privately insured are less likely to receive surgery (704)Holland MM, et al. (2025) J Gastrointest Surg, 29: 102037. .
Collectively, these data highlight the need for multilevel interventions to ensure equitable delivery of guideline-recommended surgery for all cancer patients. Researchers and policymakers must work together to improve access to quality surgical care for all patients while continuing further research into the mechanisms that perpetuate disparities. In this regard, an urgent unmet need is to capture and integrate sexual orientation and gender identity data in the surgical literature to understand the extent of perioperative disparities SGM patients may experience (705)Broekhuis JM, et al. (2023) JAMA Surg, 158: 111. . Furthermore, concerted efforts from the medical research community and policymakers are needed to enhance and diversify the current surgical oncology workforce, which currently lacks representation from many segments of the US population (706)Webber AA, et al. (2025) Curr Probl Surg, 63: 101697. .
Treatment With Radiation Therapy
Radiotherapy is the use of high-energy rays (e.g., gamma rays and X-rays) or particles (e.g., electrons, protons, and carbon nuclei) to control or eradicate cancer. Discovery of X-rays in 1895 allowed visualization of internal organs at low doses, and the effective use of X-rays at high doses to treat a breast cancer patient a year later established radiotherapy as the second pillar of cancer treatment. Radiotherapy plays a central role in the management of cancer and works primarily by damaging DNA, leading to cancer cell death.
Globally, 50 percent of all patients with a new diagnosis of cancer need radiotherapy as their initial treatment, and 15 percent require follow-up radiotherapy (707)Abdel-Wahab M, et al. (2024) Lancet Oncol, 25: e545. . As cancer cases continue to rise globally, experts predict that by 2050, the need for trained radiotherapy professionals will grow by more than 60 percent (707)Abdel-Wahab M, et al. (2024) Lancet Oncol, 25: e545. .
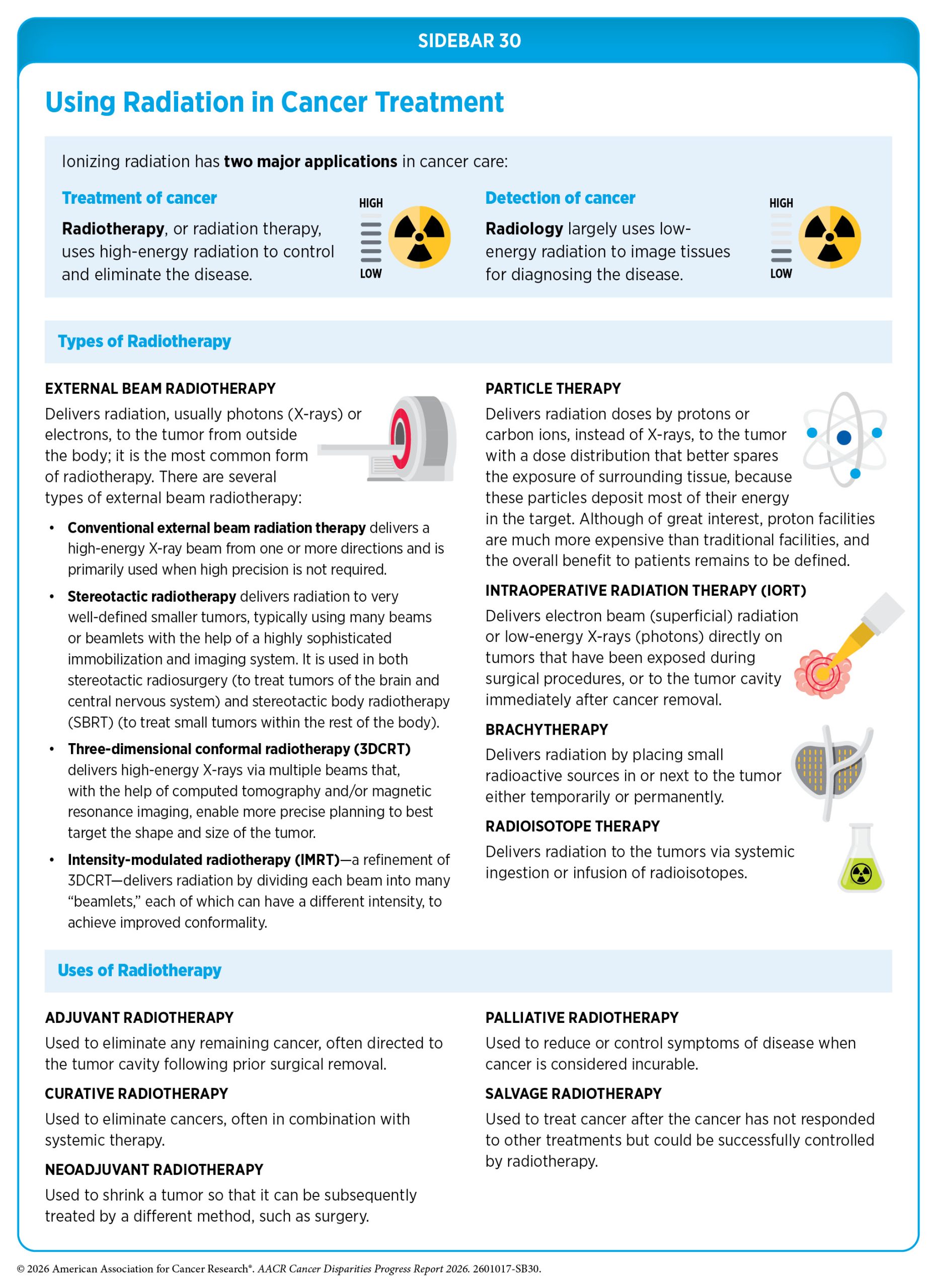
There are many types of and uses for radiotherapy (see Sidebar 30). However, it is important to note that radiotherapy may also have harmful side effects, partly because of the radiation-induced damage to healthy cells surrounding the tumor tissue (708)Wang K, et al. (2021) CA Cancer J Clin, 71: 437. . Because of the central role of radiotherapy in the treatment and management of cancer, researchers are continually innovating radiotherapeutic approaches to maximize the benefits for patients while minimizing potential harm.
Long-term effects of radiation therapy can negatively impact a patient’s quality of life. Researchers are evaluating approaches to make radiotherapy safer and more effective, including using biomarkers to identify patients who are unlikely to benefit from radiation or may be more vulnerable to its toxic effects, allowing radiotherapy to be reduced or even avoided without affecting patient outcomes (709)Kishan AU, et al. (2025) Clin Cancer Res, 31: 2530. (710)Meattini I, et al. (2025) JAMA Oncol, 11: 329. . An exciting new area in radiotherapy is the use of radiopharmaceuticals or molecularly targeted radiotherapeutics—radiation-emitting molecules that are linked to targeting molecules, which steer the radiation specifically to cancer cells. A particularly promising innovation is theranostics, which combines diagnostic imaging and molecularly targeted radiotherapy to deliver personalized treatment based on a patient’s unique tumor characteristics. Several such diagnostic therapeutic pairs have been approved by FDA in recent years for the management of certain patients with neuroendocrine tumors and prostate cancer (285)American Association for Cancer Research. AACR Cancer Progress Report 2023. Accessed: March 31, 2026. (711)American Association for Cancer Research. AACR Cancer Progress Report 2018. Accessed: March 31, 2026. (712)American Association for Cancer Research. AACR Cancer Progress Report 2021. Accessed: March 31, 2026. , and many more are at various stages of preclinical and clinical testing (713)Giugliano F, et al. (2025) Cancer Treat Rev, 136: 102940. (714)Davis RA, et al. (2023) J Med Chem, 66: 9842. (715)Ganguly T, et al. (2023) J Nucl Med, 64: 639. (716)American Association for Cancer Research. AACR Cancer Progress Report 2024. Accessed: June 11, 2025. .
Unfortunately, significant disparities in radiotherapy use exist among US cancer patients, contributing to disparities in cancer outcomes. Reduced access to and utilization of radiation therapy, including as curative treatments, have been well documented. As one example, recent analysis evaluating geographic access to cancer care for patients with early-stage NSCLC demonstrated that older, Hispanic, and uninsured patients in areas with lower access to radiation oncologists were significantly less likely to receive radiotherapy (717)Shrestha P, et al. (2025) JAMA Netw Open, 8: e251061. . Lack of access to radiation oncologists was associated with higher lung cancer mortality.
Breast-conserving surgery followed by radiation is the standard of care for most patients with early-stage invasive breast cancer, as adding radiation reduces recurrence and improves survival. Evidence shows persistent disparities in the use of radiation, with certain populations lacking access to receiving treatment or refusing radiotherapy. Patients who are White and those with private insurance or Medicare are more likely to receive timely radiation after surgery compared to Black patients and those with Medicaid (718)Reyes N, et al. (2026) Breast J, 2026: 9942451. . Black and NHPI women as well as patients who are uninsured or live farther away from treatment facilities are also more likely to refuse radiation therapy (674)Bhadouriya R, et al. (2025) Ann Surg Oncol, 32: 4034. .

Particle therapy is a cutting-edge technology that uses protons or carbon ions to more precisely target tumors and spare surrounding tissue, but its high cost and unclear overall benefit limit widespread use. Moreover, access is unequal, with non-White and lower-income patients less likely to receive proton therapy compared to higher-income and White patients (719)Washington CG, et al. (2024) Cancers (Basel), 16. . The use of other advanced radiotherapy techniques, such as stereotactic radiosurgery or stereotactic radiotherapy, proton radiation therapy, and brachytherapy, is more common in populations with greater socioeconomic advantage, predominantly White individuals and those with higher income and education levels (720)Courtney PT, et al. (2026) Front Oncol, 16: 1694910. . In contrast, three-dimensional conformal radiation therapy, a less advanced technique, is more frequently used in areas with greater socioeconomic disadvantages and in rural settings. These disparities are concerning because evidence indicates that approaches such as brachytherapy can deliver effective treatment in fewer sessions and reduce the travel burden, benefits that are especially important for patients in rural areas, such as Melanie R. Stewart.
Stereotactic radiotherapy is another advanced approach to radiotherapy that can more precisely target radiation to tumors than conventional forms of external beam radiotherapy (see Sidebar 30). As a result, higher doses of radiation can be used without damaging healthy tissues surrounding a tumor, which reduces the long-term adverse effects of radiotherapy. Recent clinical trials have shown that stereotactic radiotherapy targeted at certain metastatic tumors can reduce the chances of disease progression and increase survival for patients who have solid tumors, such as prostate and lung cancers, and gastrointestinal tumors. Stereotactic radiotherapy has increasingly become the preferred approach for many patients with brain metastases, supported by growing evidence favoring its use over whole-brain irradiation. A study of older adult patients with brain metastases indicated that while its use increased from 22 percent in 2010 to 54 percent in 2019, Black and Hispanic patients were 10 percent to 20 percent less likely to receive stereotactic radiotherapy, compared to White patients (721)Grobman B, et al. (2026) JNCI: Journal of the National Cancer Institute. .
Yet another recent advance is hypofractionated radiotherapy, in which patients receive fewer but higher doses of radiotherapy compared to the traditional regimen (722)Cho WK, et al. (2024) JAMA Oncol, 10: 737. . Patients who receive hypofractionated radiotherapy complete their radiotherapy over a shorter period and in fewer treatment sessions. In a recent review, researchers indicate that this approach is just as effective as traditional, longer radiation courses for treating breast cancer, while also offering benefits like fewer side effects, better cosmetic results, improved quality of life, and greater convenience for patients (723)Lee SF, et al. (2024) BMJ, 386: e079089. . Despite established benefits for patients, hypofractionated radiotherapy is underused and there are disparities in its uptake in the United States (724)Booth S, et al. (2024) Pract Radiat Oncol, 14: e305. .
Overall, these findings call for new evidence-based strategies to improve access to radiotherapy services for all patients with cancer. It is imperative that all stakeholders in medical research and public health come together to identify populations and areas with the greatest barriers to radiation care, investigate the underlying barriers, and develop tailored interventions with the goal of reducing health disparities.
Treatment With Chemotherapy
Chemotherapy, which involves the use of chemicals to kill cancer cells, was first introduced as a pillar of cancer treatment in the early to mid-20th century. Chemotherapy remains a backbone of cancer treatment, and its use is continually evolving to minimize potential harm to patients, while maximizing its benefits.
As with surgery and radiotherapy, chemotherapy is more commonly used to treat cancer in combination with one or more additional types of treatments. Newer and more effective chemotherapeutics continue to be evaluated in clinical research. In addition, researchers are continually evaluating the optimal dosage, novel formulations, treatment combinations, and sequence of chemotherapy delivery to improve patient outcomes.
Chemotherapy is an important component of treatment for many patients with breast cancer, particularly those with aggressive disease. Breast cancers are classified by the presence or absence of three key biomarkers—estrogen and progesterone hormone receptors (HR), and HER2 protein—all of which can drive tumor growth. The main subtypes are known as HR-positive/HER2-negative (~70 percent of cases), HER2-positive (~15 percent to 20 percent of cases), and triple-negative (~10 percent to 15 percent of cases) breast cancer (2)SEER*Explorer: An interactive website for SEER cancer statistics [Internet]. Surveillance Research Program, National Cancer Institute; 2026 Apr 22. [cited 2026 May 11]. Data source(s): SEER Incidence Data, November 2025 Submission (1975-2023), SEER 21 registries. . Depending on the subtype diagnosed and additional biomarkers, patients with breast cancer may receive chemotherapy before surgery (neoadjuvant) to shrink tumors or after surgery (adjuvant) to reduce recurrence risk. Studies have consistently shown disparities in chemotherapy use across all phases of treatment.
In HR-positive/HER2-negative disease, chemotherapy is given in the adjuvant setting, is guided by genomic testing, such the 21-gene recurrence score, and is usually reserved for those with a higher likelihood of cancer recurrence. A qualitative study involving interviews with a diverse group of respondents, including patients, caregivers, clinicians, navigators, payers, and policymakers, found uneven access to genomic testing for early-stage HR-positive/HER2-negative breast cancer patients (725)Olomu MUO, et al. (2025) Breast Cancer Res Treat, 215: 47. . Disparities were driven by limited awareness, confusion about testing, and practical barriers such as insurance, cost, and administrative complexity, as well as language and cultural gaps; addressing these challenges will be key to ensuring equitable access to personalized cancer care. Research also shows Black women with HR-positive/HER2-negative cancer who present with high-risk disease based on genomic tests are 16 percent less likely to receive adjuvant chemotherapy compared to White women (726)Freeman JQ, et al. (2025) JAMA Netw Open, 8: e2549109. .
Patients with HER2-positive tumors generally receive chemotherapy with HER2-targeted therapy, often in the neoadjuvant setting, which is continued or escalated after surgery based on response. Among patients with early-stage HER2-positive breast cancer, use of neoadjuvant chemotherapy and pathologic complete response rates (see Sidebar 28) have increased over time and are associated with improved survival, yet Black patients remain less likely to receive neoadjuvant therapy or achieve a complete response compared to White patients (727)Jackson I, et al. (2025) NPJ Breast Cancer, 11: 138. .
Triple-negative breast cancer is a highly aggressive disease, and patients rely mainly on chemotherapy, typically as neoadjuvant treatment, with additional adjuvant therapy for any residual disease. Use of neoadjuvant chemotherapy and complete response rates have risen significantly and are linked to better survival (728)Jackson I, et al. (2025) JCO Oncol Pract, 21: 1618. . Unfortunately, Black women are less likely to receive neoadjuvant chemotherapy or achieve a complete response, despite a higher burden of triple-negative breast cancer (728)Jackson I, et al. (2025) JCO Oncol Pract, 21: 1618. . Patients with lower income, those with non-private insurance, those living in rural areas, and those receiving care at community cancer centers are also significantly less likely to receive neoadjuvant chemotherapy, underscoring persistent inequities in access to guideline-adherent care.
Treatment with chemotherapeutics can have adverse effects on patients. These effects can occur during treatment and continue long term, or they can appear months or even years later (see Challenges Faced by Cancer Survivors). A recent analysis that assessed racial disparities in the use of chemotherapies associated with cardiotoxicity showed that Black women with breast cancer were more likely to be prescribed these treatments, compared to all other racial groups (730)Ho KL, et al. (2026) J Racial Ethn Health Disparities. . Patients with breast cancer receiving chemotherapy who live in racially and economically segregated neighborhoods experience higher rates of hospitalizations and emergency care, highlighting the role of structural inequities in driving disparities in treatment-related adverse events (731)Obeng-Gyasi S, et al. (2026) Cancer Epidemiol Biomarkers Prev, 35: 128. .
A critical area of ongoing research is identifying biomarkers to correctly predict which patients may suffer from chemotherapy-induced toxicities. Chemotherapeutics, such as 5-fluorouracil (5-FU) and capecitabine, may cause serious adverse effects. Dihydropyrimidine dehydrogenase (DPD) is a key enzyme that breaks down 5-FU by converting it into an inactive form for elimination from the body. Research has shown that some individuals may carry genetic changes in the DPYD gene, which encodes the DPD enzyme, resulting in reduced enzyme activity (DPD deficiency) and a higher risk of severe side effects. Importantly, the frequency and types of DPYD variants can vary among populations with different ancestral backgrounds, highlighting the need for more diverse research and testing for DPD deficiency (732)White C, et al. (2021) Pharmgenomics Pers Med, 14: 1603. (733)Chan TH, et al. (2024) Br J Cancer, 131: 498. . To improve patient safety, FDA has recently updated drug labels to include information about this genetic risk and now recommends that clinicians consider testing patients for DPD deficiency before starting treatment.
Treatment With Molecularly Targeted Therapy and Immunotherapy
Remarkable advances in our understanding of cancer biology, including the discovery of numerous cellular and molecular alterations that drive tumor growth, have ushered in a new era of precision medicine. As a result, the standard of care is shifting away from a one-size-fits-all approach toward treatments tailored to the patient and the unique characteristics of their cancer (see Understanding Cancer Development in the Context of Cancer Disparities).
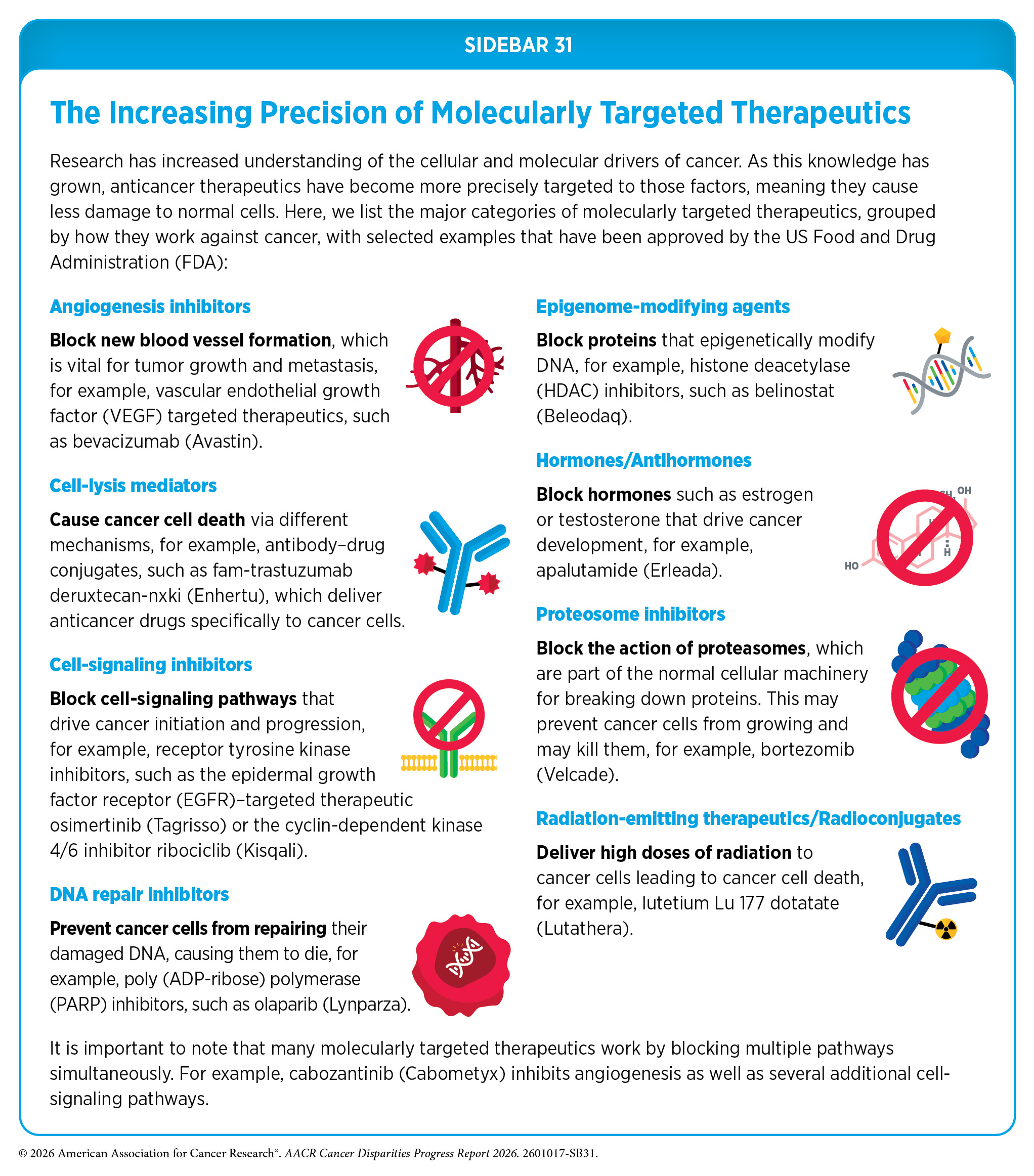
Therapeutics directed to molecules influencing cancer cell multiplication and survival limit damage to healthy tissues by targeting tumor cells more precisely than chemotherapeutics, which generally target all rapidly dividing cells. The greater precision of these molecularly targeted therapeutics tends to make them more effective and less toxic than chemotherapeutics (see Sidebar 31). As a result, they are not only saving lives but also allowing patients with cancer to have a higher quality of life.
In the past two decades, the pace of progress in molecularly targeted therapeutic development has accelerated, with increasingly rapid translation of discoveries from bench to bedside. A growing number of therapies now effectively target cancer-driving proteins once considered undruggable, including KRAS, which is implicated in multiple cancer types such as lung, colorectal, and pancreatic cancers. At the same time, there has been a marked expansion in novel therapeutic modalities, particularly antibody–drug conjugates (ADCs), which deliver cytotoxic agents directly to cancer cells, thereby enhancing efficacy while limiting systemic toxicity. Reflecting this momentum, the number of FDA-approved ADCs has grown substantially—from only one indicated for a type of lymphoma in 2011, to 13 approved for more than 10 cancer types, including both solid tumors and hematologic malignancies, in 2025 (274)American Association for Cancer Research. AACR Cancer Progress Report 2025. Accessed: March 31, 2026. .
The immune system is highly effective in detecting and eliminating cancer cells, a process also known as cancer immune surveillance (734)Hiam-Galvez KJ, et al. (2021) Nat Rev Cancer, 21: 345. . However, as cancer cells acquire new properties during the course of cancer development (see Understanding Cancer Development in the Context of Cancer Disparities), some cells find ways to “hide” from the immune system, such as by decreasing or eliminating the numbers and/or amounts of proteins on the surface of tumor cells that are used by the immune system to recognize cancer cells; triggering certain brakes on immune cells that prevent them from eradicating cancer cells; and releasing molecules that weaken the ability of immune cells to detect and destroy cancer cells (735)Mishra AK, et al. (2022) Diseases, 10. . The field of cancer immunology is focused on better understanding how tumor cells evade the immune system and leveraging this knowledge to develop novel cancer treatments. Unprecedented advances in cancer immunology over the past two decades have firmly established immunotherapy as the fifth pillar of cancer medicine (736)Kaufmann SHE (2019) Front Immunol, 10: 684. .
Immunotherapy harnesses the body’s own immune system to recognize and attack cancer, offering long-lasting responses even in advanced or hard-to-treat diseases. These therapies can work through several approaches, such as the following: Immune checkpoint inhibitors (ICIs) activate cancer-eliminating immune cells by blocking proteins that would otherwise restrain them; adoptive cell therapies, such as chimeric antigen receptor (CAR) T-cell therapy, strengthen a patient’s immune cells to better identify and destroy cancer; bispecific T-cell engagers connect T cells directly to cancer cells, enhancing the immune system’s ability to eliminate tumors. In the past two decades, immunotherapy has advanced rapidly, providing patients with powerful, personalized treatment options. Reflecting this progress, the number of FDA-approved ICIs has increased from just one in 2011 to 15 in 2025, FDA-approved adoptive cell therapies and bispecific T-cell engagers from none to nine over the same period (274)American Association for Cancer Research. AACR Cancer Progress Report 2025. Accessed: March 31, 2026. . Today, immunotherapy treatments are approved for many different types of solid tumors and blood cancers, significantly broadening the range of patients who can benefit from these innovative treatments.
Molecularly targeted therapies and immunotherapies, which together constitute the paradigm of precision medicine, have transformed clinical outcomes for cancers that were once uniformly fatal, including advanced and metastatic lung cancer and melanoma. Diagnostic tests, such as sophisticated DNA sequencing or protein visualizing methods, are commonly used in the clinic to identify molecular changes in patients’ cancers, helping to select those who are most likely to benefit from molecularly targeted therapeutics and immunotherapies, and spare others from unnecessary treatments and side effects. Companion diagnostic tests are required for the safe and efficacious use of certain FDA-approved treatments, while complementary diagnostic tests are not mandatory but provide additional insights on clinical decision-making.
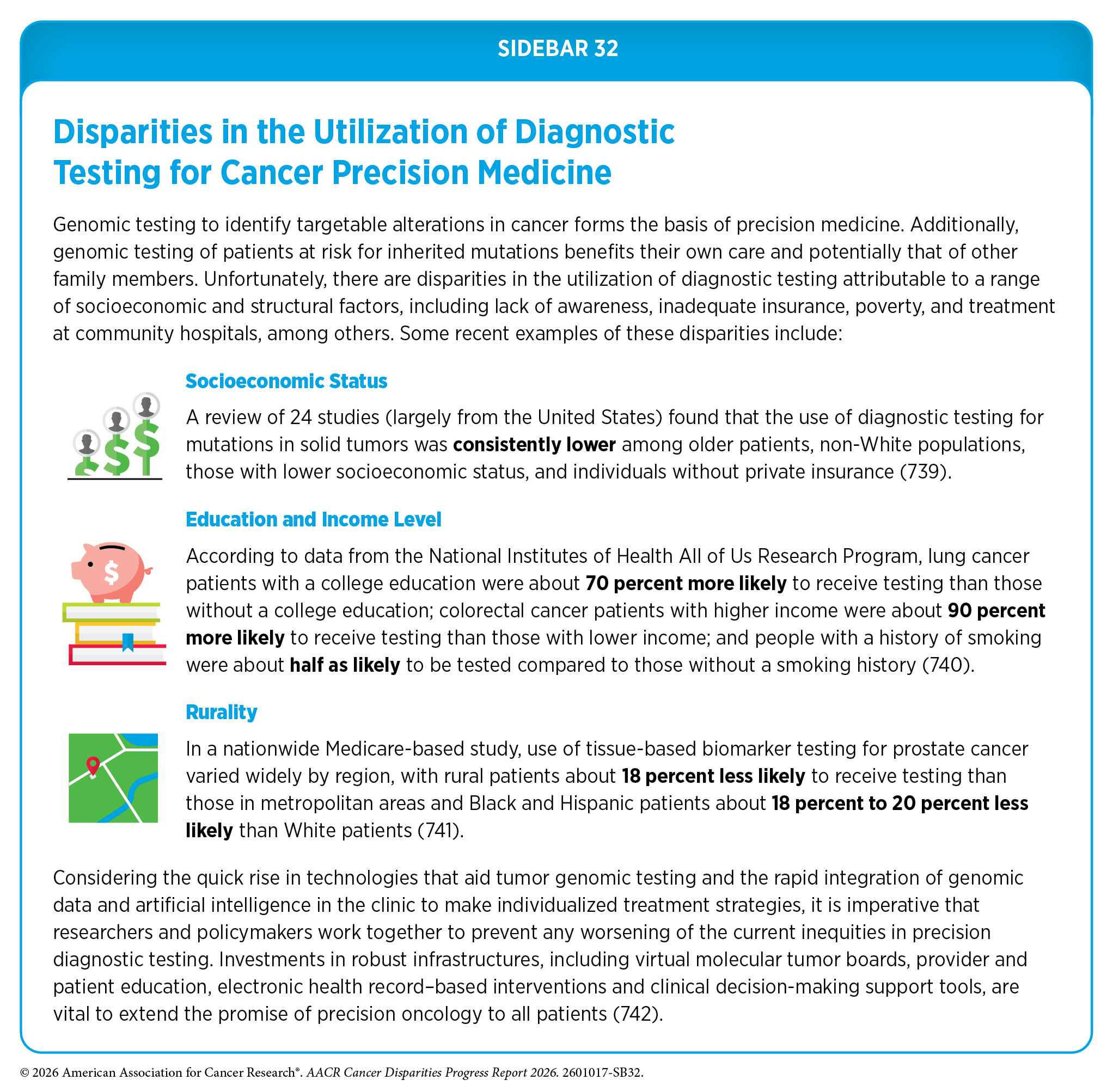
Unfortunately, there are disparities in the utilization of diagnostic testing (see Sidebar 32) as well as in the receipt of molecularly targeted therapies and immunotherapies. These disparities stem from multilevel barriers to health care, including inadequate health insurance, costs of care, and lack of access to quality cancer care (275)Phillip G. Febbo et al. (2024) JCO Precis Oncol 8, e2300382. (737)Podany EL, et al. (2025) JAMA Netw Open, 8: e2461899. (770)Heath E, et al. (2024) Cancer Res Commun, 4: 2598. .
The value of genomic testing in guiding precision treatment across populations is illustrated by a study of 5,015 US veterans with metastatic prostate cancer, which found that Black patients were more likely to harbor alterations associated with eligibility for immunotherapy, whereas White patients more frequently had alterations in pathways amenable to targeted therapies (738)Valle LF, et al. (2025) JAMA Netw Open, 8: e259119. . The benefits of FDA-approved precision medicine have not been evenly distributed. Patients of African ancestry are less likely to have cancers with well-established, targetable markers, which may limit the utility of certain molecularly targeted treatments (282)Arora K, et al. (2025) JAMA Oncol, 11: 310. .
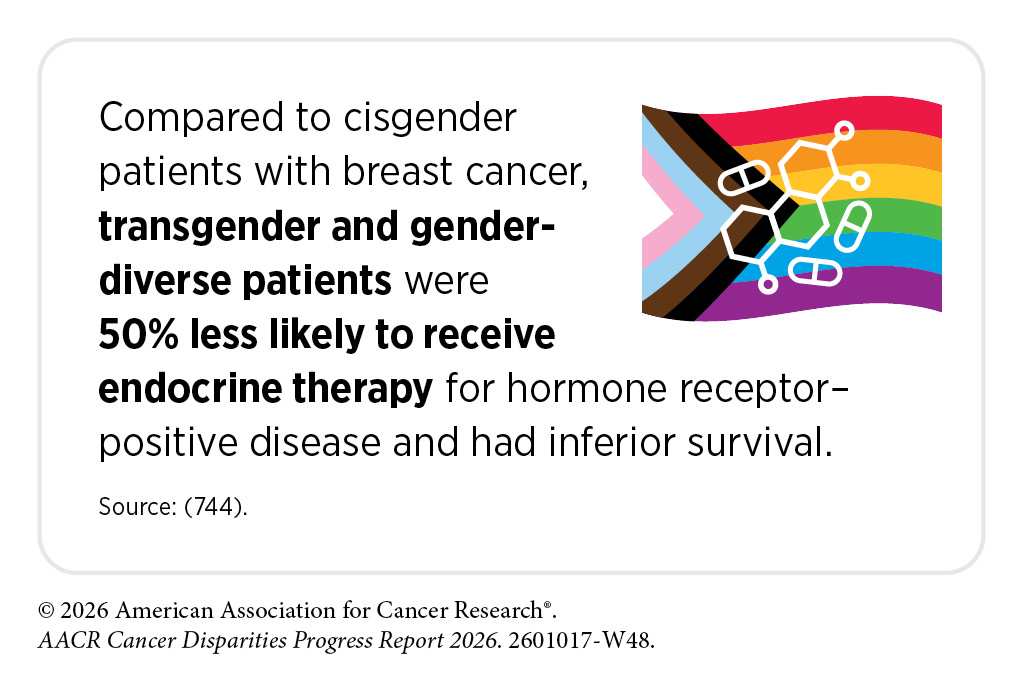
Thanks to major advances in precision medicine, breast cancer death rates have declined significantly in the United States. Just in the past decade, nearly 20 molecularly targeted therapeutics and immunotherapeutics have been approved for breast cancer. About 70 percent of breast cancers diagnosed in the United States are characterized as HR-positive/HER2-negative (2)SEER*Explorer: An interactive website for SEER cancer statistics [Internet]. Surveillance Research Program, National Cancer Institute; 2026 Apr 22. [cited 2026 May 11]. Data source(s): SEER Incidence Data, November 2025 Submission (1975-2023), SEER 21 registries. . Treatment options for these patients include antihormone therapeutics (also called endocrine therapy), with or without another molecularly targeted therapy known as a cyclin-dependent kinase 4/6 inhibitor, the first of which was approved by FDA in 2015. Between 2015 and 2019, when these agents were first being used along with antihormone therapy, White women were more likely to receive them than Black and Hispanic women (743)Vidal GA, et al. (2026) Cancer Epidemiol Biomarkers Prev. . Patients with lower incomes and those treated in community settings were also less likely to receive these treatments compared to those with higher incomes or those treated at academic centers. Encouragingly, these differences became smaller between 2020 and 2023 (743)Vidal GA, et al. (2026) Cancer Epidemiol Biomarkers Prev. .
Many advanced HR-positive breast cancers eventually stop responding to antihormone therapy because the cancer becomes resistant. One reason is a pathway involving the PI3K-alpha protein, which is overactive in about half of these cancers and often driven by mutations in the PIK3CA gene. Molecularly targeted treatments have been developed to block this pathway, including alpelisib and inavolisib, which, when used with other therapies, can help control cancer for longer. In a US study of 1,327 women with metastatic breast cancer who were treated at academic institutions and who underwent genomic testing between 2015 and 2023, Black patients with PIK3CA mutations were significantly less likely than White patients to receive PI3K inhibitor treatment, even though both groups had similar rates of the PIK3CA alterations that these drugs are meant to target (737)Podany EL, et al. (2025) JAMA Netw Open, 8: e2461899. .
Genomic testing using next-generation sequencing—an advanced diagnostic method—has transformed the management of advanced prostate cancer by identifying actionable genetic alterations, such as BRCA1/2 mutations in about 30 percent of patients, that inform the use of targeted therapies and improve outcomes (745)Hage Chehade C, et al. (2024) JAMA Netw Open, 7: e2423186. . Despite overall increases in next-generation sequencing in metastatic prostate cancer (from 19 percent in 2015 to 27 percent in 2022), and in advanced urothelial cancer (from 14 percent in 2015 to 47 percent in 2022), significant disparities persist (745)Hage Chehade C, et al. (2024) JAMA Netw Open, 7: e2423186. . Black and Hispanic patients, individuals with low socioeconomic status, those with Medicaid or government insurance, and people living in certain geographic regions remain consistently less likely to receive genomic testing (745)Hage Chehade C, et al. (2024) JAMA Netw Open, 7: e2423186. (746)Diaz GM, et al. (2025) Urology. .
Patients with advanced prostate cancer that has spread and carries BRCA1/2 mutations can be treated with molecularly targeted therapeutics known as poly (ADP-ribose) polymerase (PARP) inhibitors, which have been shown to help patients live longer. Based on an analysis of a large US database built from electronic health records mostly from community clinics and some academic practices, only half of eligible patients received a PARP inhibitor (747)Ostrowski M, et al. (2025) JAMA Netw Open, 8: e2534968. .
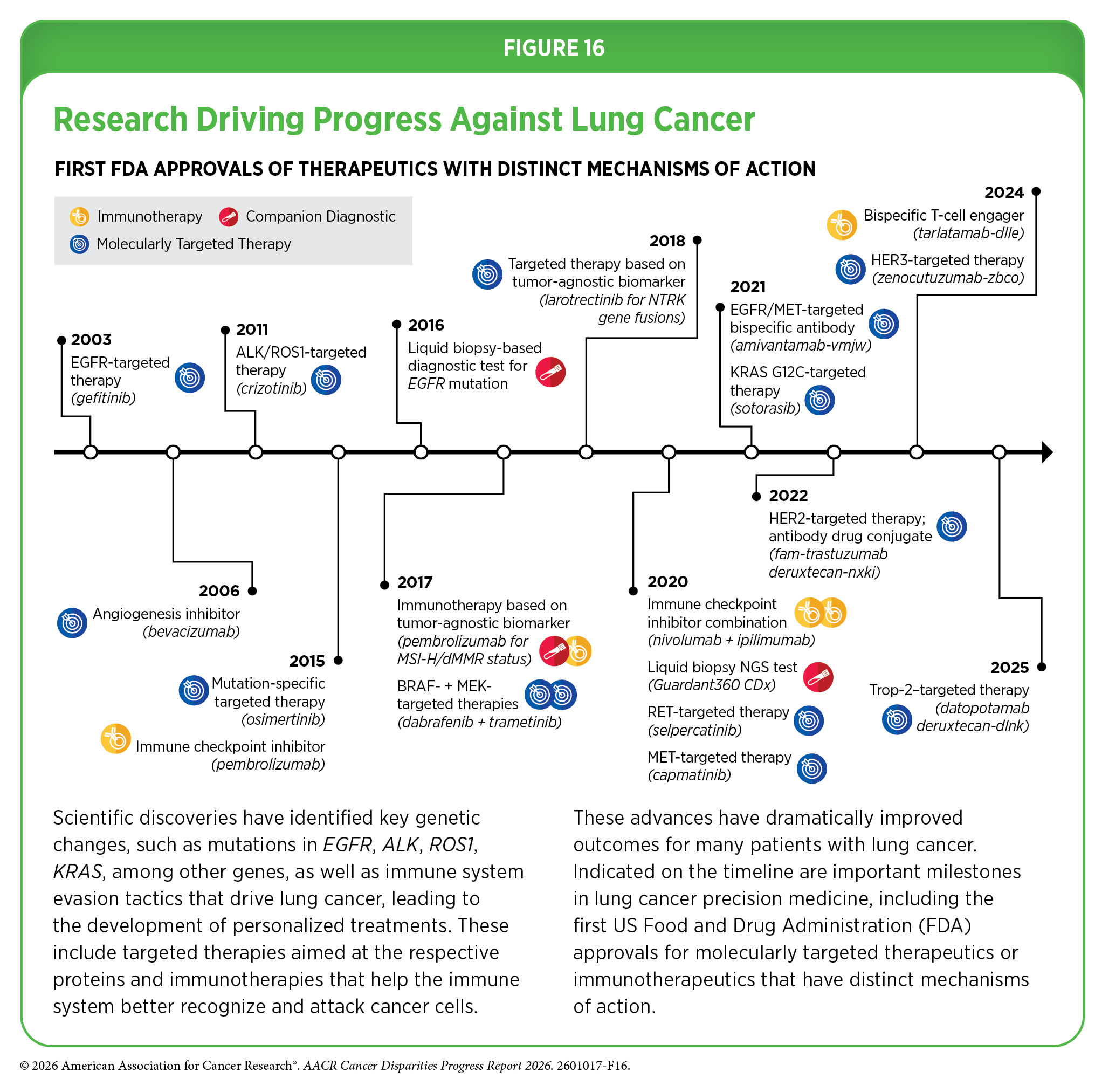
Lung cancer is the leading cause of cancer deaths in the United States. An estimated 229,410 new cases will be diagnosed, and 124,990 people will die from the disease in the United States in 2026 (19)Siegel RL, et al. (2026) CA Cancer J Clin, 76: e70067. . More than 80 percent of lung cancers diagnosed in the United States are classified as NSCLC. Research over the past decade has significantly increased our understanding of the genetic drivers of lung cancer, which has led to the development of precision medicine directed at many of these alterations (see Figure 16). Thanks to these breakthroughs in treatment, as well as improved prevention and earlier detection, the decline in lung cancer death rates has accelerated in the past decade.
The use of precision medicine for lung cancer relies on biomarker-based diagnostic testing and access to molecularly targeted therapies and immunotherapies. Using data from the All of Us Research Program, a study of 287 patients with advanced NSCLC showed that biomarker testing was documented in only 18 percent of patients, and disparities were observed. Individuals who had any college education were more likely than those without college education to receive targeted therapy, while retired patients were significantly less likely than employed patients to receive targeted therapy, highlighting gaps in access to precision care (748)Kiel PJ, et al. (2025) J Cancer Educ. . Another study from a large, diverse Northern California integrated health system evaluating 8,267 patients with NSCLC found that only 39 percent received biomarker testing, with higher use observed among younger, never-smoking, and less socioeconomically deprived patients (749)Carroway WP, et al. (2025) Front Surg, 12: 1632360. ; those who underwent next-generation sequencing–based testing had a 13 percent lower risk of death at 3 years.
Osimertinib is a molecularly targeted therapy that inhibits EGFR, a protein that, when mutated, becomes hyperactive and drives the growth of NSCLC cells. It is approved by FDA as a single agent or in combination with chemotherapy for certain patients with locally advanced or metastatic NSCLC. However, the clinical trials leading to its approval included limited participation of racial and ethnic minority populations, raising concerns about the generalizability of findings to real-world patient populations (750)Lee M, et al. (2026) NPJ Precis Oncol, 10. . In a retrospective analysis of 174 patients with advanced, EGFR-mutated NSCLC that included a substantial proportion of Hispanic, Black, and Asian patients, Black patients had significantly worse overall survival compared to White patients, despite similar treatment adherence (750)Lee M, et al. (2026) NPJ Precis Oncol, 10. . These data reinforce the vital importance of inclusive clinical trials to ensure that we fully understand the population specific benefits of new molecularly targeted therapeutics.
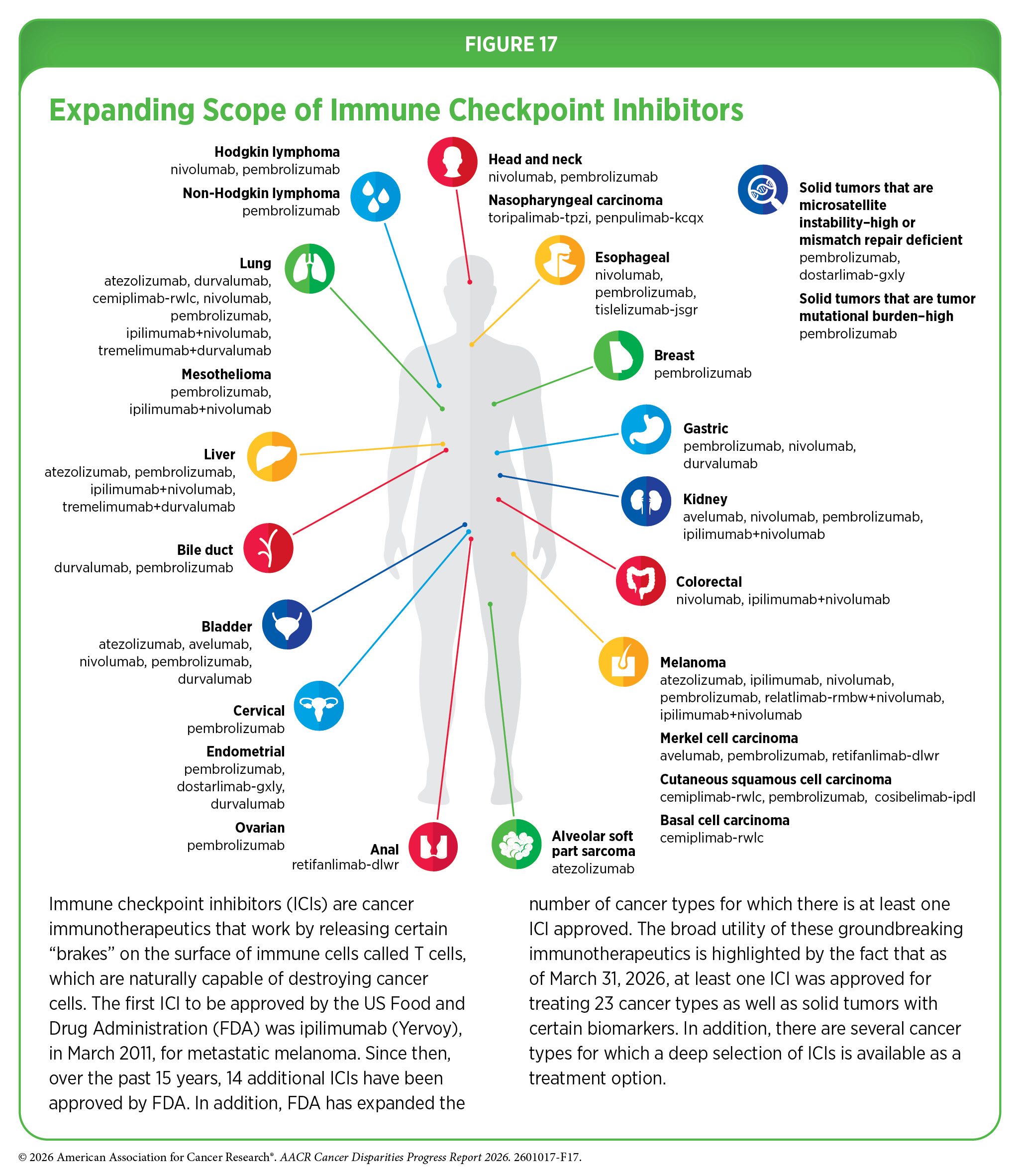
The first ICI was approved by FDA in 2011 for the treatment of patients with metastatic melanoma. Since 2011, the FDA approvals and use of ICIs have expanded rapidly, and these therapeutics are currently considered one of the most exciting approaches to cancer treatment (see Figure 17). This is because some patients with metastatic cancers who have been treated with these therapeutics have had remarkable and durable responses. For example, long-term results from a clinical trial testing the ICI pembrolizumab in patients with advanced NSCLC showed that 23 percent of patients lived 5 or more years after the treatment, which stands in stark contrast to the historically low 5-year relative survival rate for these patients of just about 5 percent (751)Garon EB, et al. (2019) J Clin Oncol, 37: 2518. . Another clinical trial that monitored advanced melanoma patients for at least 7.5 years showed that half of the patients treated with the combination of two ICIs, nivolumab and ipilimumab, lived at least 6 years (752)Wolchok JD, et al. (2025) N Engl J Med, 392: 11. . Before ipilimumab was approved in 2011, most patients lived less than a year.
A large US study of more than 47,000 patients receiving treatment for advanced or metastatic melanoma between 2004 and 2021 demonstrated that the use of immunotherapy increased substantially and was linked to better survival, but access to these treatments was uneven (753)Ali MS, et al. (2025) Immunotherapy, 17: 37. . Patients with private insurance, living in neighborhoods with higher income and education, and those treated at academic centers were more likely to receive immunotherapy. Additionally, Black patients experienced worse outcomes than White patients even when receiving similar immunotherapies. This finding underscores the need to increase participation of underrepresented populations in clinical trials to better understand the effectiveness of novel therapies in patients from diverse racial and ethnic groups.
Another study comparing outcomes of patients ages 18 to 64 with metastatic melanoma, NSCLC, and kidney cancer, before and after the introduction of FDA-approved ICIs, showed that survival improved overall for all patients, but disparities widened, with uninsured patients experiencing significantly smaller gains than those with private insurance (754)Zhao J, et al. (2025) JAMA Netw Open, 8: e2519274. . These findings highlight the need for policies that expand access to health insurance and improve the affordability of novel cancer therapies to ensure equitable benefit across populations.
Treatment with FDA-approved ICIs improves outcomes for patients with advanced or metastatic triple-negative breast cancer, an aggressive disease with a disproportionate burden among Black women. A recent analysis of the use of ICI and its potential association with patient outcomes showed that while use increased since the FDA approval, Black women with metastatic disease were less likely to receive ICIs, compared to White women (755)Freeman JQ, et al. (2025) JAMA Netw Open, 8: e2460243. . Lower use was also evident among older adults, patients treated in community settings, and those without private insurance (665)Ajjawi I, et al. (2025) Cancers (Basel), 17. . Encouragingly, patients who received ICIs experienced significantly improved survival, with similar outcomes observed across racial and ethnic groups (665)Ajjawi I, et al. (2025) Cancers (Basel), 17. (755)Freeman JQ, et al. (2025) JAMA Netw Open, 8: e2460243. . In this regard, a large study from VHA that included more than 26,000 patients across multiple cancer types, predominantly lung cancer, found that Black patients treated with ICIs had similar or slightly improved survival and lower rates of treatment-related toxicities, compared to White patients, highlighting the importance of equitable access to treatments in reducing cancer disparities (756)Miller S, et al. (2024) Lancet Oncol, 25: 1666. .
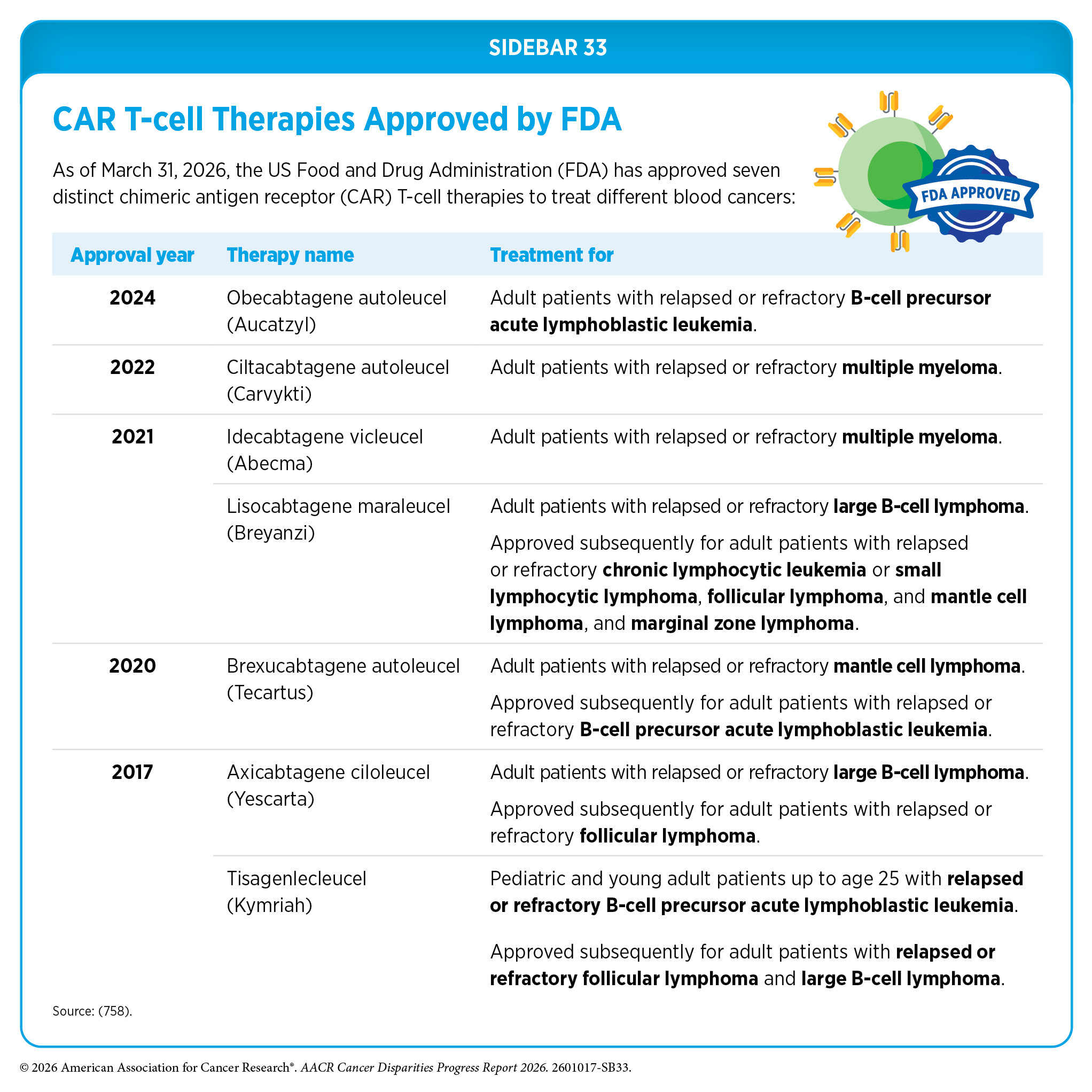
CAR T-cell therapy is a form of cellular immunotherapy that has revolutionized the treatment landscape for blood cancers. As of March 31, 2026, FDA has approved seven CAR T-cell therapies, all for the treatment of blood cancers, including leukemia, lymphoma, and multiple myeloma (see Sidebar 33). CAR T-cell therapies represent a breakthrough in the treatment of pediatric leukemia, the most common cancer in children (757)Dana H, et al. (2021) Acta Pharm Sin B, 11: 1129. .
Only selected cancer centers in the United States have the capability and approval to administer CAR T-cell therapies, with many states having limited access for patients, as was the case with Vanessa Bañuelos. Consequently, disparities in access to CAR T-cell therapies have been well reported. As one example, patients with lymphoma living in low-income states and farther from CAR T-cell therapy centers are less likely to receive treatment (759)Chung AP, et al. (2025) Blood Adv, 9: 4727. . Researchers estimate that reducing travel distance could increase CAR T-cell therapy access nationwide by 38 percent. Based on a multicenter study, there are also disparities in the receipt of CAR T-cell therapy among racial and ethnic minority patients with lymphoma. Additionally, the study revealed differences in outcomes by race and insurance type, including faster cancer progression in Black patients and worse outcomes among patients with Medicaid (760)Karmali R, et al. (2024) Blood Adv, 8: 2592. . In another study among adult patients with blood cancers, 44 percent of the 400 patients who were referred to CAR T-cell therapy did not receive the treatment (761)Valtis YK, et al. (2025) JAMA Oncol, 11: 781. . The data showed that patients who were Black were less likely to receive CAR T-cell therapy.
Multiple myeloma is the second most common blood cancer in the United States among White individuals, but its higher incidence in the Black population compared to the White population makes multiple myeloma the most common blood cancer among Black individuals. Research has now shown that a single infusion of the CAR T-cell therapy ciltacabtagene autoleucel can produce long-term remission, with about one-third of patients alive and free of disease progression after 5 years, marking a major step toward a potential cure (762)Jagannath S, et al. (2025) J Clin Oncol, 43: 2766. . However, a study of 12,360 multiple myeloma patients treated across six University of California health systems and affiliated hospitals between 2021 and 2025 showed that less than 3 percent received CAR T-cell therapy, with Black patients significantly less likely than White patients to receive the treatment; additional differences were observed by treatment location (763)Davidson J, et al. (2026) Cancers (Basel), 18. .
Barriers to access and delivery of CAR T-cell therapies occur at multiple levels, including policy, institutional, provider, and patient factors, each contributing to inequities in care (764)Kaparis S, et al. (2025) Blood Rev: 101358. (765)Munshi PN, et al. (2026) Transplant Cell Ther. . At the patient level, financial burden, limited awareness, cultural biases, and logistical challenges, such as transportation and caregiving-related needs, pose significant barriers, highlighting the importance of patient education and support programs to improve equitable access. Provider-level challenges include knowledge gaps, concerns about toxicity, financial burden, and complex treatment logistics, which may be mitigated through education and standardized patient referral frameworks.
Policy-level barriers include complex and inconsistent insurance authorization processes, uneven or inconsistent coverage, and high out-of-pocket costs, while potential facilitators include standardized coverage policies and cost-reduction strategies. At the institutional level, limited geographic access to specialized treatment centers and capacity constraints restrict availability, while expansion of treatment sites, outpatient delivery models, and telehealth may improve access.
Because of serious or life-threatening immune-related adverse reactions, FDA initially required CAR T cells to be administered only at specially certified large academic hospitals by qualified health care professionals with appropriate medical support. However, most US cancer patients receive their treatment at community settings, which limits their access to this rapidly growing class of lifesaving immunotherapies (766)Byrne MT, et al. (2025) JAMA Oncol, 11: 481. . Innovations in simplifying manufacturing and broadening delivery are needed so more patients can benefit from CAR T-cell therapies.
In June 2025, FDA removed the special safety requirements for approved CAR T-cell therapies, a decision expected to expand access by allowing more treatment centers—including those in community and rural areas—to administer these therapies without additional regulatory hurdles (767)US Food & Drug Administration. FDA Eliminates Risk Evaluation and Mitigation Strategies (REMS) for Autologous Chimeric Antigen Receptor (CAR) T cell Immunotherapies. Accessed: March 31, 2026. . Despite this change, the administration of CAR T cells requires close collaboration across many medical specialties, which can be challenging in resource-limited communities.
Equity in Quality Cancer Care
Research has shown that survival disparities across several cancer types can be eliminated in the United States when patients have equitable access to novel therapeutics that are increasingly becoming the standard of care (716)American Association for Cancer Research. AACR Cancer Progress Report 2024. Accessed: June 11, 2025. (755)Freeman JQ, et al. (2025) JAMA Netw Open, 8: e2460243. (768)Espinoza-Gutarra MR, et al. (2026) Blood Lymphat Cancer, 16: 559759. . As one example, some studies have found that racial or ethnic disparities in cancer outcomes are mitigated among veteran patients who are treated at a single-payer system, such as the VHA, the nation’s largest integrated health care system (769)Kim RB, et al. (2025) J Racial Ethn Health Disparities, 12: 2646. . Equitable access to precision diagnostics has also been shown to help reduce disparities in cancer outcomes. For instance, in a large multi-institutional study of more than 12,000 US patients who underwent genomic testing, outcomes were largely similar across racial and socioeconomic groups (770)Heath E, et al. (2024) Cancer Res Commun, 4: 2598. . However, some disparities persisted at more granular levels, including in specific cancers and among younger patients, potentially reflecting differences in tumor biology associated with inherited genetic variation and other clinical factors. These findings highlight the need for further research to better understand and address the remaining drivers of disparities.
Researchers have also shown that for many cancers, racial and ethnic minority patients may respond better to treatments and have better outcomes compared to White patients when offered similar access to guideline-adherent care (756)Miller S, et al. (2024) Lancet Oncol, 25: 1666. . As one example, when Black and White patients with multiple myeloma received comparable treatment and had similar socioeconomic status, overall health, and the stage at which the disease was diagnosed, disparities in survival were effectively eliminated (771)Dong J, et al. (2022) Blood Cancer J, 12: 34. . In fact, Black patients had a 4.6 percent higher 5-year survival rate compared to their White counterparts (771)Dong J, et al. (2022) Blood Cancer J, 12: 34. . Similar patterns are emerging in other blood cancers with the advent of precision medicine. A population-level analysis showed that survival disparities in Black patients with acute myeloid leukemia that were seen in earlier treatment eras were no longer observed following the introduction of the molecularly targeted therapeutic venetoclax, despite Black patients having lower socioeconomic status. Notably, when utilization of novel therapies was comparable across groups, Black patients experienced survival outcomes comparable to, or in some cases better than, those of White patients (772)Wang X, et al. (2025) Blood Adv, 9: 533. .
In the following sections, we describe targeted interventions from recent studies that have demonstrated success in reducing disparities in cancer treatment.
Vital Role of Patient Navigation and Community Engagement
Given the accumulating evidence that disparities in cancer outcomes can be reduced, and in some cases eliminated, when all patients receive guideline-adherent, high-quality care, it is essential that researchers develop innovative strategies to increase access to standard treatments and cutting-edge clinical trials for medically underserved populations. These strategies must simultaneously address many of the complex and interrelated structural and social barriers that contribute to disparities in cancer care.
There is strong evidence that patient navigation can be effective in reducing time to cancer diagnosis in adults, reducing hospital readmissions during treatment, increasing adherence to follow-up appointments, and improving treatment knowledge and patients’ satisfaction with care (773)Chan RJ, et al. (2023) CA Cancer J Clin, 73: 565. . A recent review of 59 studies found that patient navigation programs significantly improved cancer care, with percent of studies showing better treatment initiation, percent showing improved treatment adherence, 87 percent reporting higher patient satisfaction, and 81 percent demonstrating improved quality of care, particularly benefiting disadvantaged populations (as highlighted in 76 percent of studies) (774)Chen M, et al. (2024) Curr Oncol Rep, 26: 504. . Research has shown that patient navigation can overcome numerous challenges related to SDOH, including transportation, food insecurity, language, literacy, and health insurance, among others.
Diagnostic testing for molecular alterations in tumors is a prerequisite for treatment with many molecularly targeted therapies and immunotherapies, and there are known disparities in the receipt of these tests (see Sidebar 32). Studies have shown that patient navigation can improve the rates of tumor genomic testing, specifically among medically underserved populations. As one example, in a study of 693 prostate cancer patients, implementation of a precision medicine navigator increased overall genomic testing rates from 18 percent to 70 percent, with substantial gains among underserved groups, including Black patients (from 18.2 percent to 58.5 percent), patients with lower income (from 20 percent to 64 percent), those with Medicare and Medicaid (from 20 percent to 68.5 percent), and patients treated at community sites (from 6 percent to 77 percent) (776)Allen AJ, et al. (2026) JCO Oncol Pract: OP2500983. .
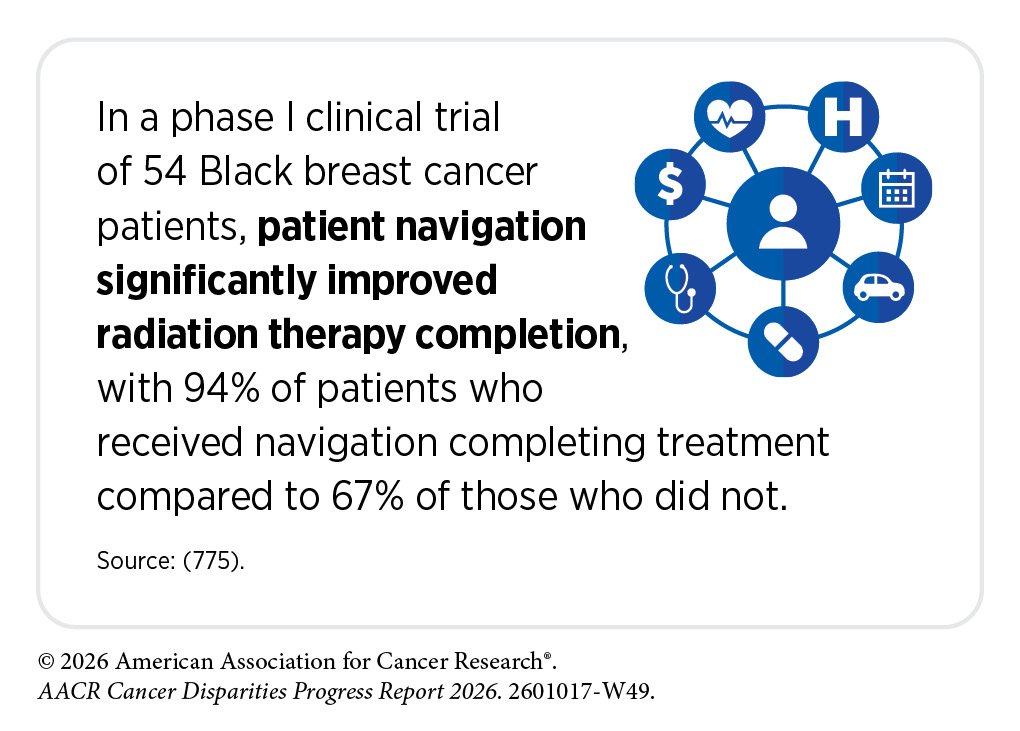
Research has shown that patient navigation can improve timely treatment initiation, increase rates of treatment completion, and enhance quality of life for patients with cancer. In a randomized clinical study among patients with head and neck cancer, an enhanced patient navigation program helped many more patients start radiation therapy on time after surgery (74 percent vs. 39 percent with usual care) and made them about 82 percent more likely to start timely treatment and 67 percent more likely to complete treatment, showing that navigation can reduce delays and improve care (777)Graboyes EM, et al. (2025) JCO Oncol Pract, 21: 1153. . Starting radiation on time is important because delays are linked to worse cancer outcomes and survival. In another randomized clinical trial among medically underserved cancer patients treated at safety-net clinics in New York City, a multilingual, multidisciplinary patient navigation program increased treatment completion (92 percent vs. 78 percent with usual care) and led to greater improvements in quality of life, depression symptoms, and stress, compared to usual care (778)Gany F, et al. (2025) J Natl Compr Canc Netw, 23. .
Partnering with community-based organizations to design strategies that improve care is a key solution. Several studies demonstrate that integration of community health workers can improve receipt of evidence-based cancer care across the continuum among veteran and non-veteran populations. These studies consistently demonstrate the impact of multi-level interventions on improvements in molecular testing and evidence-based treatment and improvements in care delivery with reductions in acute care use, increased hospice use, and reductions in total costs of care for people with cancer who are nearing the end of life (779)Wood EH, et al. (2026) Cancers, 18: 1247(780)Thomas M, et al. (2025) JCO Oncol Pract: OP2500531. .
In one randomized clinical trial, low-income and racial and ethnic minority patients with cancer who received a three-level intervention involving elimination of payer prior authorization for molecular testing, clinician training regarding evidence-based guidelines for molecular testing and targeted therapeutics, and patient-level education and support delivered by community health workers regarding precision cancer care had a three-fold greater odds of receiving molecular testing and targeted therapeutics than those who received the payer and clinician intervention alone (779)Wood EH, et al. (2026) Cancers, 18: 1247. Further studies showed the impact of such co-designed strategies on reductions in symptom burden among older adults with cancer (781)Patel MI, et al. (2026) JAMA, 335: 674. . These efforts have been sustained as part of the usual cancer care across multiple facilities given that they were co-designed with patients, caregivers, community-based organizations, payer organizations, and clinicians.
Impact of Health Insurance and Access to Care
Ensuring affordable health insurance and access to quality care is fundamental to reducing disparities in cancer treatment and improving outcomes for underserved populations (see Overcoming Cancer Disparities Through Science-based Public Policy). In this context, Medicaid expansion through the Patient Protection and Affordable Care Act (ACA) has been shown to increase insured status, early diagnosis, access to high-volume hospitals, and timely cancer treatment, and reduce cancer disparities, leading to improved outcomes for patients (162)Tamirisa N, et al. (2024) Ann Surg, 280: 136. (782)Hooda Z, et al. (2025) Ann Thorac Surg, 120: 401. (783)Lyons JM, et al. (2025) Cancers (Basel), 17. . As one example, Medicaid expansion was associated with better access to surgical resection and improved survival for patients with pancreatic cancer (784)Hohenleitner JT, et al. (2026) JAMA Surg. .
Historically, older women from racial or ethnic minority populations with HER2-positive breast cancer had reduced access and lower rates of treatment with HER2-targeted therapies, leading to worse outcomes. In a study of 12,765 Medicare beneficiaries with HER2-positive breast cancer diagnosed between 2010 and 2019, use of targeted therapies increased over time and racial and ethnic disparities in receipt narrowed, with no differences observed between Black, Hispanic, and White patients by 2018–2019 (785)Krishnamurthy S, et al. (2025) JAMA Netw Open, 8: e258086. . Given that all patients were Medicare insured, these findings suggest that factors beyond insurance coverage contributed to the narrowing of disparities and warrant further investigation.
Patients with cancer living in US rural areas have significantly reduced access to quality health care due to geographic isolation and lack of specialty care facilities and physicians in rural communities. Based on a recent analysis, rural-residing patients were approximately two times more likely to cross state lines for surgical procedures, three times more likely to cross state lines for radiation therapy, and almost four times more likely to cross state lines for chemotherapy services, compared to urban-residing patients (661)Moen EL, et al. (2025) JAMA Netw Open, 8: e2461021. . Expanding telemedicine is a feasible strategy that has been effectively used by medically underserved populations, but sustaining its impact will require policy changes to address cross-state licensure and reimbursement barriers (786)Torrado C, et al. (2026) Oncologist, 31. .
An emerging strategy to increase access for rural patients is the home hospital approach. A recent study in rural US and Canadian settings, which comprised delivery of hospital-level acute care at home using in-person nurse and/or paramedic visits, remote physician care, intravenous therapies, remote monitoring, video communication, and point-of-care testing, showed similar costs, readmission rates, and length of stay as at brick-and-mortar hospitals, while improving patient activity levels and experience (787)Levine DM, et al. (2025) JAMA Netw Open, 8: e2545712. . Notably, promising preliminary evidence shows that certain patients with common, high-burden cancers such as colon and lung cancers living in rural areas who undergo elective surgery at rural facilities closer to their home have similar outcomes to those who choose to travel farther to urban facilities (788)Egger ME, et al. (2026) J Am Coll Surg, 242: 1032. . While more research is needed to examine the unique characteristics of rural and urban facilities that achieve strong patient outcomes, these data highlight opportunities for certain rural patients to receive their cancer care closer to home, decreasing their travel burden without compromising outcomes.
In conclusion, it is imperative that cancer researchers and physicians move past simply describing disparities to developing a more in-depth understanding of the interrelated factors associated with disparate cancer treatments and outcomes. Addressing disparities in treatment and improving the health of the nation’s medically underserved patients can enhance the quality of care for all and advance population health. Poor outcomes in racial and ethnic minority groups and other underserved populations are not isolated; they contribute to poorer outcomes for all patients across the health care system. Because structural barriers and inequitable policies limit regular access to high-quality care, individuals in these communities are more likely to seek care only after disease has advanced, often relying on emergency departments as a primary point of access. This overreliance, in turn, places a substantial burden on the US health care system and economy.
A greater understanding of the underlying drivers of disparities will lay the foundation for comprehensive, sustainable, population-based interventions that can potentially narrow treatment differences among different populations and improve outcomes for all patients. Furthermore, all scientific endeavors must be complemented with evidence-based policy initiatives that aim toward delivering guideline-adherent quality care for every cancer patient (see Policies to Address Disparities in Clinical Research and Care). All stakeholders committed to fundamentally changing the face of cancer must work together to address the challenges of disparities in cancer treatment and lead us toward a brighter, healthier future for all populations.
Next Section: Disparities in Cancer Survivorship Previous Section: Disparities in Cancer Screening for Early Detection
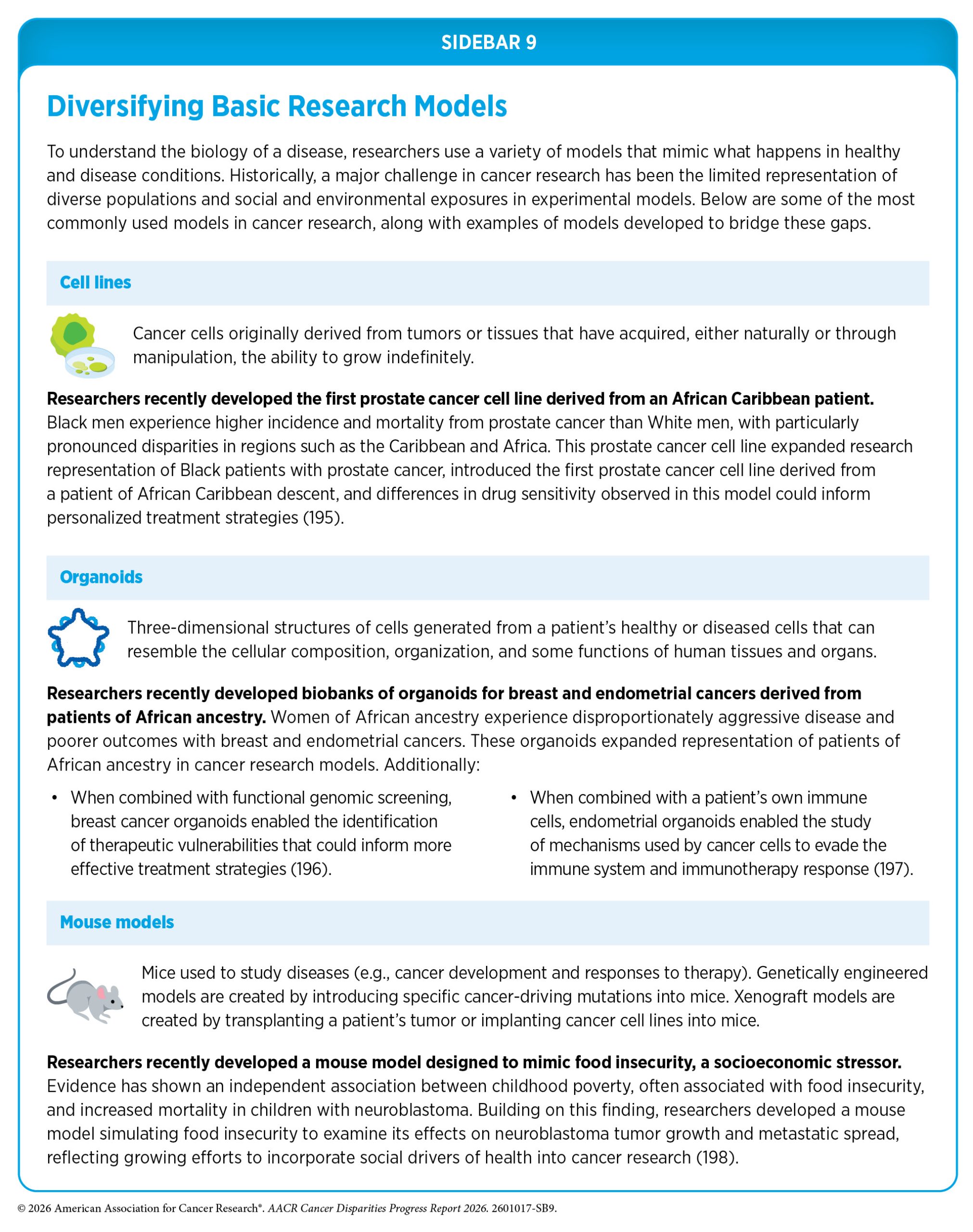{kind=link}