Disparities in the Burden of Modifiable Behavioral Cancer Risk Factors
In this section, you will learn:
- In the United States (US), about 40 percent of all cancer cases are associated with modifiable risk factors.
- Built environments disproportionately expose racial and ethnic minority groups and other medically underserved populations to cancer risk factors, including commercial tobacco, pollution, and toxic chemicals.
- Despite overall declines in cigarette smoking, disproportionately high use of commercial tobacco continues among certain populations. Targeted marketing, policy gaps, and inequitable delivery of cessation services sustain disparities in tobacco‑related cancer risk and outcomes.
- Awareness of the links between alcohol consumption and cancer development remains low across many segments of the US population.
- Despite evidence‑based dietary recommendations for cancer prevention, many communities across the US experience barriers to accessing healthy diets.
- Infections with certain pathogens can contribute to cancer development by altering cellular function, weakening immune defenses, and promoting chronic inflammation.
Contents
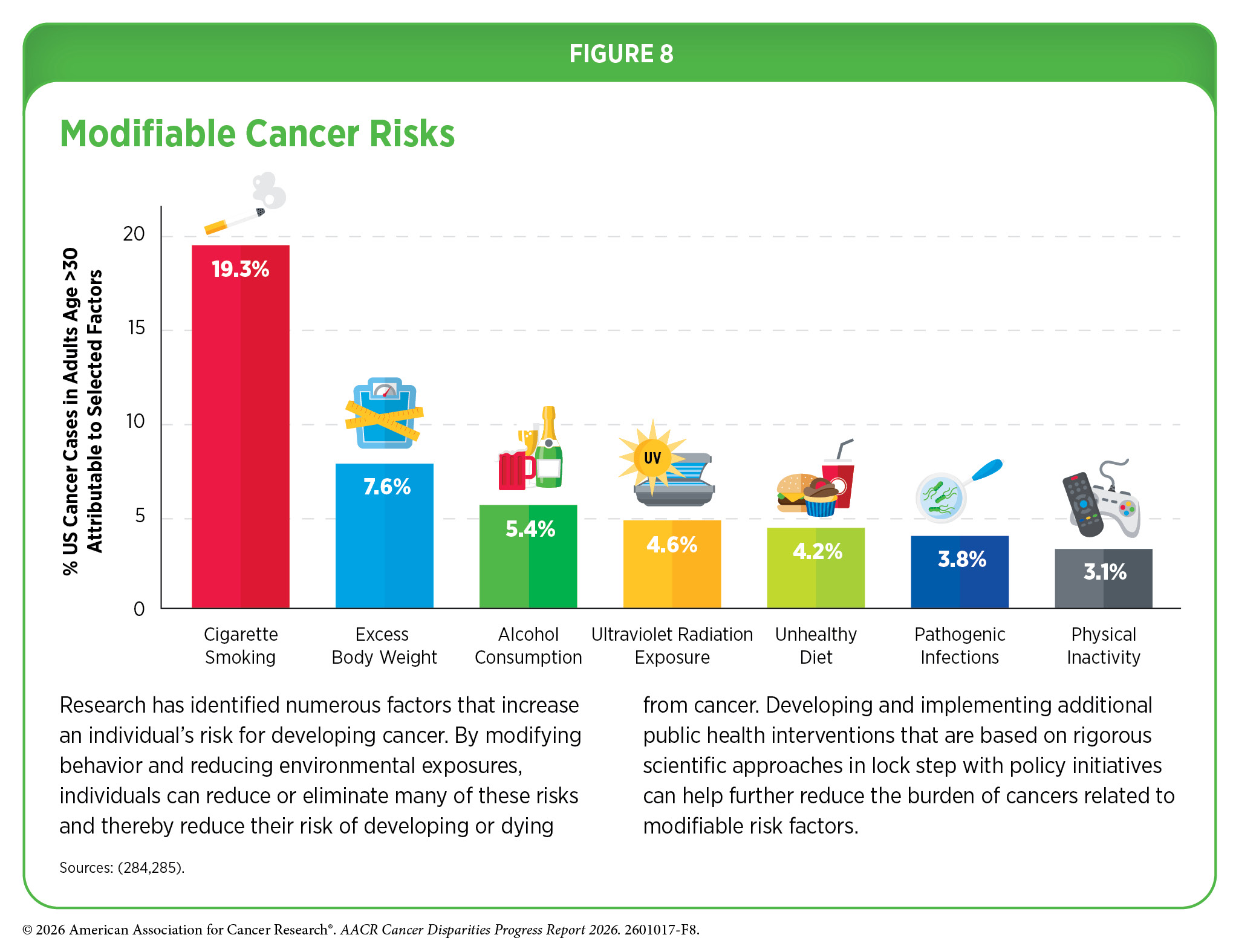
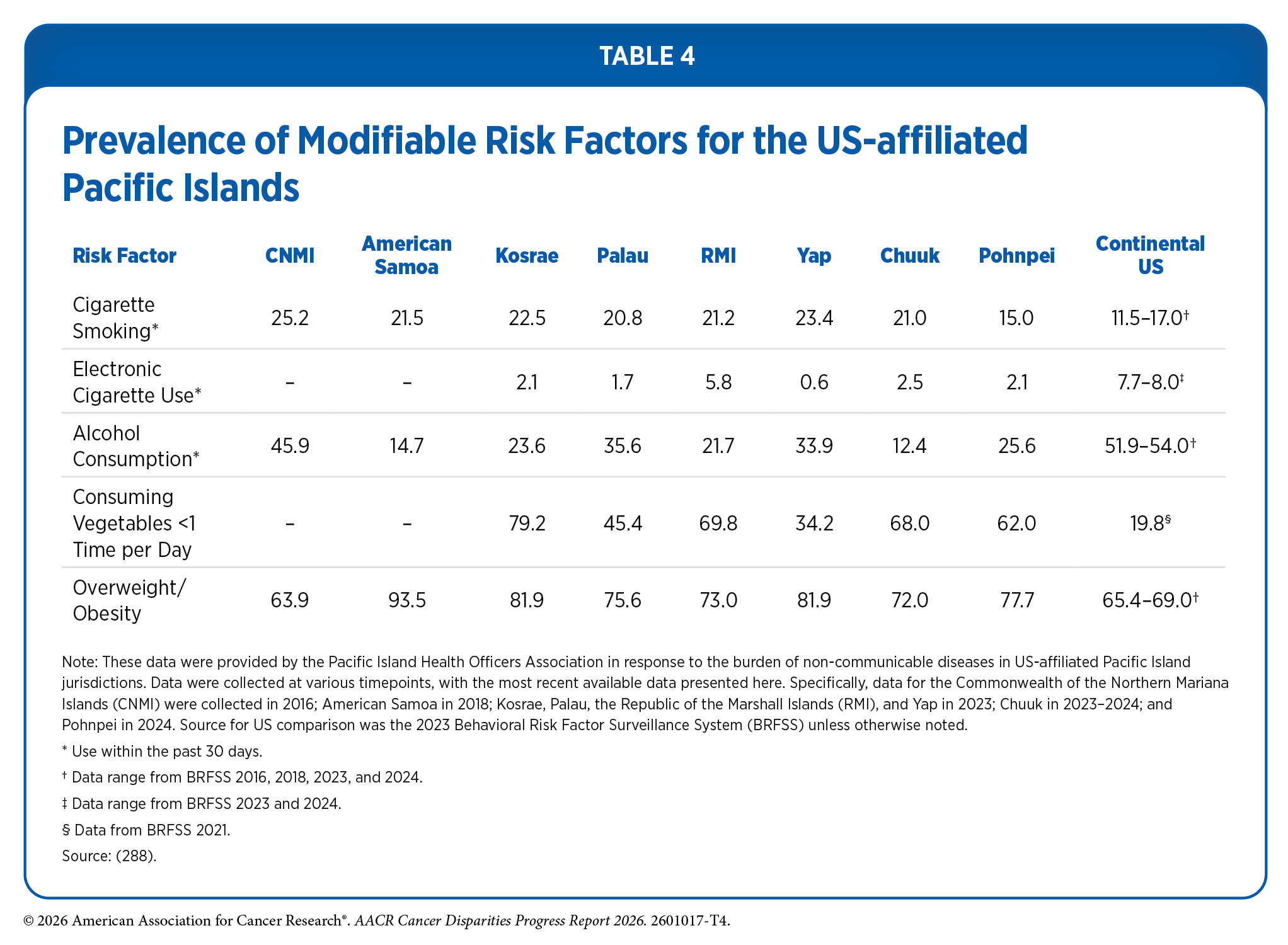
Research in basic, translational, and population sciences has broadened our understanding of factors that increase an individual’s risk of developing cancer. Behavioral and lifestyle factors such as tobacco use, unhealthy diet, physical inactivity, ultraviolet (UV) light exposure, alcohol consumption, exposure to pathogenic infections, and obesity contribute to the development of 40 percent of all cancers (284)Islami F, et al. (2024) CA Cancer J Clin, 74: 405. . Because these factors are modifiable, meaning individuals can potentially change or eliminate these behaviors—such as through quitting commercial tobacco use or receiving recommended vaccinations against pathogenic infections—adopting healthier choices can substantially lower the risk of developing cancer and, in turn, prevent many new cancers (see Figure 8). However, the prevalence of these risk factors varies significantly across segments of the United States (US) population (see Table 4), reflecting broader structural and social conditions that influence health behaviors and opportunities.
Differences in the prevalence of modifiable behavioral and lifestyle factors can also be attributed to systemic structural and social injustices that have affected multiple disparate populations in the United States. As an example, historical redlining—a discriminatory federal housing practice beginning in the 1930s in which neighborhoods with large minority populations were labeled “high risk,” leading banks and insurers to deny residents mortgages, loans, and other financial services—has been linked to present-day neighborhoods with higher levels of poverty, vacant housing, lower economic mobility, poorer environmental conditions, and adverse health outcomes, including poorer cancer survival (158)Schwartz E, et al. (2021) Health Place, 68: 102529. (286)Swope CB, et al. (2022) J Urban Health, 99: 959. . These structural conditions shape the environments in which people live, work, and make daily decisions, subsequently increasing exposure to certain cancer risk factors and making healthy choices more difficult, thereby contributing to disparities in individual behavioral risk. For instance, historically redlined neighborhoods have been associated with a higher density of tobacco and alcohol retailers (158)Schwartz E, et al. (2021) Health Place, 68: 102529. (287)Trangenstein PJ, et al. (2020) Journal of Urban Health, 97: 123. . Strategies that reduce exposure to this wide range of avoidable cancer risk factors have the potential to lessen the burden of cancer and other debilitating conditions. Addressing these upstream structural drivers is therefore essential to achieving lasting and equitable improvements in population health.
Commercial Tobacco Use
Tobacco has a long and complex history in the United States, with ceremonial and cultural use among Indigenous populations dating back to at least 1000 CE. Ceremonial or traditional tobacco has been used by American Indian or Alaska Native (AIAN) Nations for centuries for medicinal, cultural, and spiritual purposes. Its use varies across tribes but commonly includes prayer, healing, purification, offerings, and communication with the spiritual world. Traditional tobacco is not intended for recreational use and is used with cultural protocols that emphasize respect, intent, and connection.
After British colonization, tobacco became one of the first major cash crops in North America. The commercialization of tobacco contributed to the enslavement of Indigenous peoples and people of African descent, who were forced to cultivate and maintain tobacco crops. These disruptions also complicated the distinction between ceremonial and commercial uses of tobacco within AIAN communities (289)Nez Henderson P, et al. (2025) JNCI Monographs, 2025: 184. (290)Fagan P, et al. (2025) JNCI Monographs, 2025: 187. .
As the commercial tobacco industry expanded, American Indian populations were removed from more than 90 million acres of land, and the use of tobacco for ceremonial and traditional purposes was outlawed. These policies contributed to the AIAN population having the highest prevalence of commercial tobacco use among all racial and ethnic groups in the United States (290)Fagan P, et al. (2025) JNCI Monographs, 2025: 187. (291)Bandi P, et al. (2025) Cancer Epidemiol Biomarkers Prev, 34: 836. . This elevated use directly increases cancer risk and is reflected in population-level health outcomes among AIAN communities. Between 2001 and 2021, the incidence of tobacco-related cancers increased by an average of 2.6 percent annually among AIAN adults ages 20 to 49 years, compared to an overall 0.1 percent annual decrease in this age group in the overall US population (292)Mansingka N, et al. (2025) Cancers (Basel), 17. .
The use of commercial tobacco products is the leading modifiable cause of cancer and contributes to the development of 18 different cancer types, including cancers of the oral cavity and pharynx, lung, larynx, esophagus, pancreas, uterine cervix, kidney, bladder, stomach, liver, colon and rectum, and acute myeloid leukemia. Although cigarettes continue to be the most commonly used commercial tobacco products in US adults, cigarette smoking has declined from 42 percent in 1964 to just under 10 percent in 2024 (291)Bandi P, et al. (2025) Cancer Epidemiol Biomarkers Prev, 34: 836. .
Despite this progress, several segments of the US population continue to experience disproportionately high smoking rates (293)Agaku I, NEJM Evidence, 0: EVIDpha2500339. . For example, 27.4 percent of men without a high school diploma are current smokers, compared to 5.3 percent of men with a college degree. Smoking prevalence is also significantly higher among sexual and gender minority (SGM) populations; bisexual women report smoking rates of more than twice those of heterosexual women (20 percent vs. 8.8 percent) (291)Bandi P, et al. (2025) Cancer Epidemiol Biomarkers Prev, 34: 836. .
Geographic patterns further highlight differences in smoking prevalence. Several Southern and Midwestern states—including Oklahoma, Louisiana, Mississippi, Tennessee, and West Virginia—have adult smoking rates between 16.2 percent and 21.9 percent and are collectively referred to as high–tobacco-burden states, or “Tobacco Nation” (291)Bandi P, et al. (2025) Cancer Epidemiol Biomarkers Prev, 34: 836. (293)Agaku I, NEJM Evidence, 0: EVIDpha2500339. . In addition to higher smoking prevalence, states in these regions tend to have more limited access to smoking cessation programs, fewer comprehensive smoke-free laws, lower state taxes on tobacco products, and less legislative investment in tobacco prevention and control efforts (294)Patel M, et al. (2026) American Journal of Preventive Medicine, 70: 108160. (295)American Lung Association. State Rankings. Accessed: March 31, 2026. . These states also experience higher poverty rates, lower educational attainment, and larger rural populations, factors consistently associated with elevated smoking prevalence (294)Patel M, et al. (2026) American Journal of Preventive Medicine, 70: 108160. . Collectively, these place based social and policy conditions contribute to disproportionate rates of tobacco-related cancers, reinforcing persistent geographic disparities in cancer incidence and mortality across the United States.
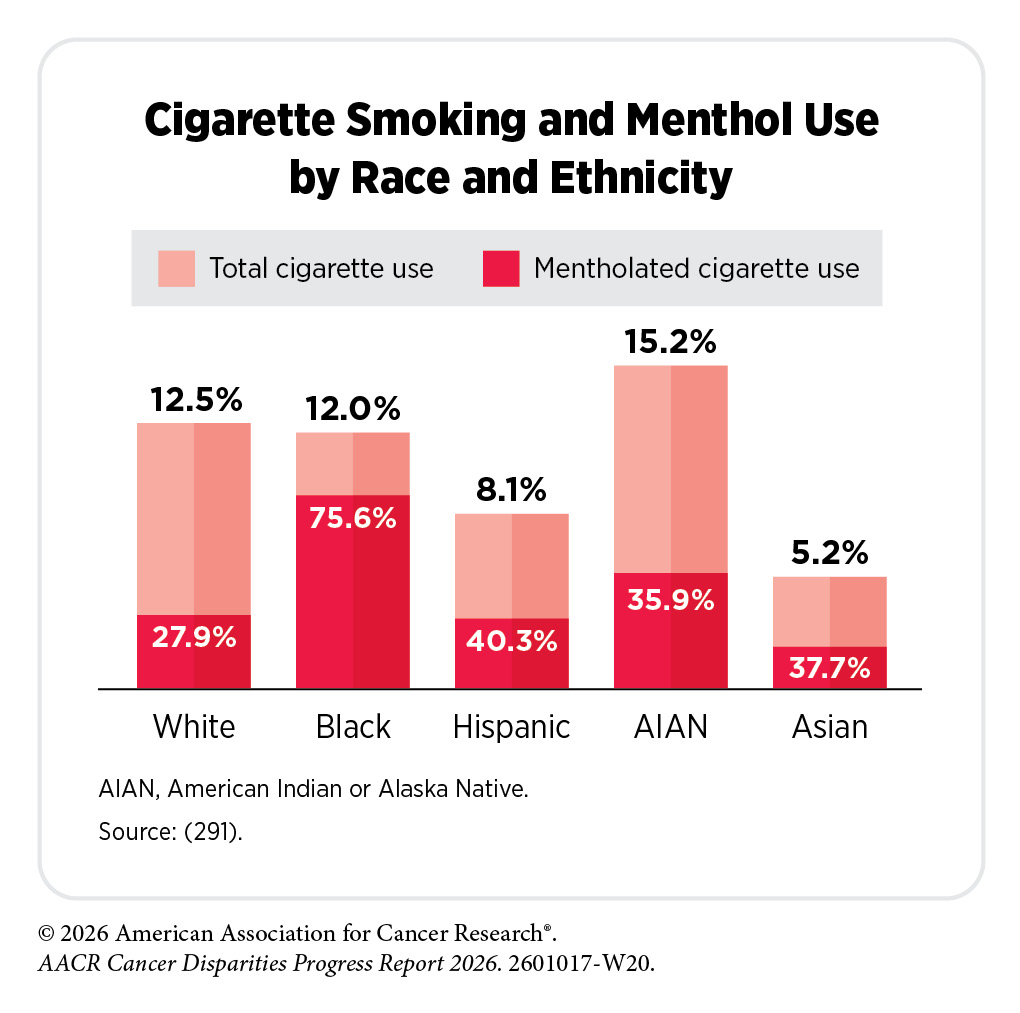
Flavored products also contribute to disparities in commercial tobacco use. Menthol—a chemical that creates a cooling, numbing sensation—is added to cigarettes to reduce throat irritation and enhance the effects of nicotine, the primary addictive compound in tobacco (296)US Food & Drug Administration. Scientific Review of the Effects of Menthol in Cigarettes on Tobacco Addiction: 1980-2021. Accessed: March 31, 2026. . Because menthol increases nicotine absorption and reduces the harshness of smoke, menthol cigarettes are more addictive, making cessation more difficult compared to non-menthol cigarettes (291)Bandi P, et al. (2025) Cancer Epidemiol Biomarkers Prev, 34: 836. . Menthol use is especially high among certain racial and ethnic minority populations, most notably among Black individuals, with more than 75 percent of those who smoke reporting that they use menthol cigarettes (297)Bandi P, et al. (2025) Tob Control. . Black individuals who use menthol cigarettes face an 88 percent higher risk of death from certain heart diseases compared to other groups, underscoring a disproportionate health burden (297)Bandi P, et al. (2025) Tob Control. .
Disparities in tobacco use are driven in part by decades of targeted tobacco industry marketing, including price discounts, lifestyle branding, giveaways, and advertisements, disproportionately directed toward Black communities and other vulnerable groups (298)Kathuria H, et al. (2024) Ann Am Thorac Soc, 21: 1245. . Between 1980 and 2018, Black individuals accounted for approximately 41 percent of smoking-related premature deaths attributable to menthol cigarettes, despite comprising only about 12 percent of the US population (299)Mendez D, et al. (2021) Tob Control. . Although the harms of menthol are well documented, the US Food and Drug Administration (FDA) has not implemented a ban on the additive. Evidence from menthol bans in Europe, Canada, and three US states shows that 24 percent of menthol smokers quit after the bans, suggesting that a national prohibition could meaningfully support cessation among menthol smokers (300)Mills SD, et al. (2025) Nicotine Tob Res, 27: 179. . However, emerging evidence suggests that tobacco companies are responding to proposed menthol restrictions by substituting other additives that produce similar cooling or sensory effects, underscoring the need for comprehensive policies that address not only menthol itself but any additives intended to replicate its effects (301)Page MK, et al. (2025) Tob Control, 34: 254. .
Use of non-combustible tobacco products, such as electronic cigarettes, commonly known as e-cigarettes, has risen sharply over the past decade, although their long-term health effects remain uncertain. In 2024, adult e-cigarette use was 7.0 percent, down from 7.7 percent in 2022 (293)Agaku I, NEJM Evidence, 0: EVIDpha2500339. (294)Patel M, et al. (2026) American Journal of Preventive Medicine, 70: 108160. . Similar to patterns seen for cigarette smoking, disparities in e-cigarette use persist. Usage is highest among young adults ages 18 to 24, nearly 15 percent of whom report current use, and it is disproportionately high among lesbian and gay individuals (19.3 percent vs. 6.3 percent among heterosexual individuals) (293)Agaku I, NEJM Evidence, 0: EVIDpha2500339. . States with high overall tobacco burden—such as Indiana, Missouri, and Oklahoma—also report higher e-cigarette prevalence, ranging from 8.1 percent to 11.0 percent compared to the 2022 national average of 7.7 percent (294)Patel M, et al. (2026) American Journal of Preventive Medicine, 70: 108160. .
Evidence is also emerging regarding the implications of e-cigarette use for lung cancer risk. A recent study of nearly 5,000 newly diagnosed lung cancer cases found that individuals who both vaped and chronically smoked cigarettes had approximately four-fold higher odds of lung cancer compared to those who smoked cigarettes alone (302)Bittoni MA, et al. (2024) J Oncol Res Ther, 9. . The presence of numerous known carcinogens, including heavy metals, volatile organic compounds, tobacco-specific nitrosamines, aldehydes, phenolic compounds, and polycyclic aromatic hydrocarbons, has been detected in e-liquid—the liquid that is converted into an aerosol by an e-cigarette, or vaping product—and e-cigarette aerosol, which may further compound the carcinogenic effects of combined cigarette and e-cigarette use (303)Besaratinia A (2025) Chem Res Toxicol, 38: 542. .
Among youth, e-cigarettes remain the most commonly used tobacco product, with 5.9 percent reporting current use in 2024, the most recent year for which data are available (304)Jamal A, et al. (2024) MMWR Morb Mortal Wkly Rep, 73: 917. . Although overall youth vaping declined from 7.7 percent in 2023 to 5.9 percent in 2024, this downward trend was not consistent across racial and ethnic groups. Notably, e-cigarette use increased among AIAN youth, rising from 5.9 percent to 11.5 percent during this period (304)Jamal A, et al. (2024) MMWR Morb Mortal Wkly Rep, 73: 917. .
The use of smokeless tobacco products—including chewing tobacco, snuff, dip, snus, nicotine pouches, and dissolvable substances—can also cause cancer. The use of these products remains low nationally at 2.6 percent. However, use varies considerably across population groups. Smokeless tobacco is more than twice as common in rural areas (5.4 percent) as in urban areas (2.1 percent) and is particularly prevalent among workers in industries such as construction, agriculture, forestry, fishing, hunting, mining, and utilities, where use ranges from 6.0 percent to 11.5 percent (293)Agaku I, NEJM Evidence, 0: EVIDpha2500339. .
Betel nut is another smokeless substance that is addictive through a different chemical compound than nicotine, but its effects on the body are similar. Betel nut is typically placed in the cheek, allowing its psychoactive compounds to be absorbed and producing increased alertness and stamina (305)Ali NS, et al. Chapter 23 – Betel Nut (Areca catechu) Usage and Its Effects on Health. In: Preedy VR, Watson RR, Patel VB, editors. Nuts and Seeds in Health and Disease Prevention. San Diego: Academic Press; 2011. p 197. It is classified as a Group 1 carcinogen by the International Agency for Research on Cancer (IARC); however, in the United States, its use is common in US-affiliated Pacific Islands, and formal public health warnings about its risks remain limited. Use is particularly common among Asian and Native Hawaiian or Pacific Islander (NHPI) populations (306)Wu N, et al. (2025) JAMA Intern Med, 185: 759. (307)Moss WJ (2022) N Engl J Med, 387: 1059. .
Exposure to secondhand smoke—created when people inhale smoke exhaled by individuals who smoke or released from burning tobacco products—has declined in the United States from 31.3 percent in 2009–2010 to 24.3 percent in 2017–2020 among individuals age 3 years and older (308)National Cancer Institute Cancer Trends Progress Report. Secondhand Smoke Exposure. Accessed: March 31, 2026. . National health goals aim to further reduce this exposure to 17.4 percent by 2030 (308)National Cancer Institute Cancer Trends Progress Report. Secondhand Smoke Exposure. Accessed: March 31, 2026. . Despite progress, secondhand smoke remains a significant public health concern, causing an estimated 53,800 deaths annually in the United States (309)National Institute on Drug Abuse. What are the effects of secondhand and thirdhand tobacco smoke? Accessed: March 31, 2026. . Beyond secondhand smoke, “thirdhand smoke”—the toxic residues that cling to indoor surfaces after smoking—poses additional risks, particularly for children, who may inhale or ingest these chemicals through normal hand to mouth behaviors while crawling or touching contaminated surfaces (310)Arfaeinia H, et al. (2023) Environ Sci Pollut Res Int, 30: 78017. .
Unfortunately, multiple segments of the US population remain disproportionately exposed to secondhand smoke. These include children ages 3 to 11; Black individuals; people with lower income or lower educational attainment; residents of rental and multi-unit housing; and individuals employed in blue collar occupations (311)Tsai J, et al. (2021) Am. J. Prev. Med, 61: e109. (312)Centers for Disease Control and Prevention. Trends and Disparities in Secondhand Smoke. Accessed: April 26, 2026. .
Evidence-based interventions at local, state, and federal levels, including tobacco price increases, public health campaigns, marketing restrictions, cessation counseling, FDA-approved medications, and smoke-free laws, must be utilized to continue the downward trend of tobacco use. A recent study found that from 1975 to 2020, 3.45 million lung cancer deaths were averted due to national smoking cessation efforts (313)Goddard KAB, et al. (2025) JAMA Oncol, 11: 162. . However, substantial gaps persist in access to tobacco cessation support. Although certain groups, including Black individuals, are more likely to express a willingness to stop smoking (314)Soulakova JN, et al. (2017) Preventive Medicine Reports, 5: 160. , they are less likely to receive the assistance needed to do so. For example, findings from a diverse, nationally representative sample of adults who used health care services show that individuals from racial and ethnic minority groups were 10 percent to 35 percent less likely to receive cessation advice from a health care provider (315)Kim N, et al. (2026) AJPM Focus, 5. .
Taken together, these disparities make clear that continued reductions in tobacco use will require both robust tobacco control policies and equal access to cessation tools, enabling every community to realize the full benefits of tobacco free living.
Obesity, Diet, and Physical Activity
In 2019, 15 percent of new cancer cases and 14 percent of cancer deaths among US adults were attributable to the combined effects of excess body weight, unhealthy diet, and physical inactivity (284)Islami F, et al. (2024) CA Cancer J Clin, 74: 405. . Although healthier lifestyles can significantly reduce cancer risk, not all communities have equal access to the resources that support such behaviors. In the United States, systemic and structural racism has created long-standing inequities in key social drivers of health (SDOH), disproportionately affecting racial and ethnic minority groups and other medically underserved populations (see Understanding and Addressing Drivers of Cancer Disparities). Inequities in income, employment opportunities, affordable housing, and neighborhood investment have shaped built environments that limit opportunities to engage in physical activity, maintain a healthy weight, and access nutritious foods—ultimately increasing cancer risk.
Obesity
Obesity is associated with an increased risk of at least 13 cancer types, including colorectal, endometrial, esophageal, pancreatic, liver, stomach, and ovarian cancers; multiple myeloma; meningioma; and postmenopausal breast cancer (316)Pati S, et al. (2023) Cancers (Basel), 15. . Beyond elevating cancer risk, obesity is linked to more adverse treatment-related events and poorer clinical outcomes. Among individuals diagnosed with cancer, obesity is associated with a 14 percent increased risk of overall mortality, a 17 percent increased risk of cancer-specific mortality, and a 13 percent increased risk of cancer recurrence (316)Pati S, et al. (2023) Cancers (Basel), 15. .
In 2024, nearly 70 percent of the US population was categorized as overweight or obese, up from 52 percent in 1996 (288)Centers for Disease Control and Prevention. BRFSS Prevalence & Trends Data. Accessed: March 31, 2026. . The incidence of several early-onset cancers associated with obesity (i.e., breast, thyroid, anal, colorectal, kidney, small intestine, endometrial, pancreatic, and myeloma) has also increased in recent years (317)Patel VR, et al. (2025) JAMA Internal Medicine, 185: 1370. . Although improvements in screening have contributed to higher rates of early detection of some of these cancers, rising obesity remains a major concern for cancer experts.
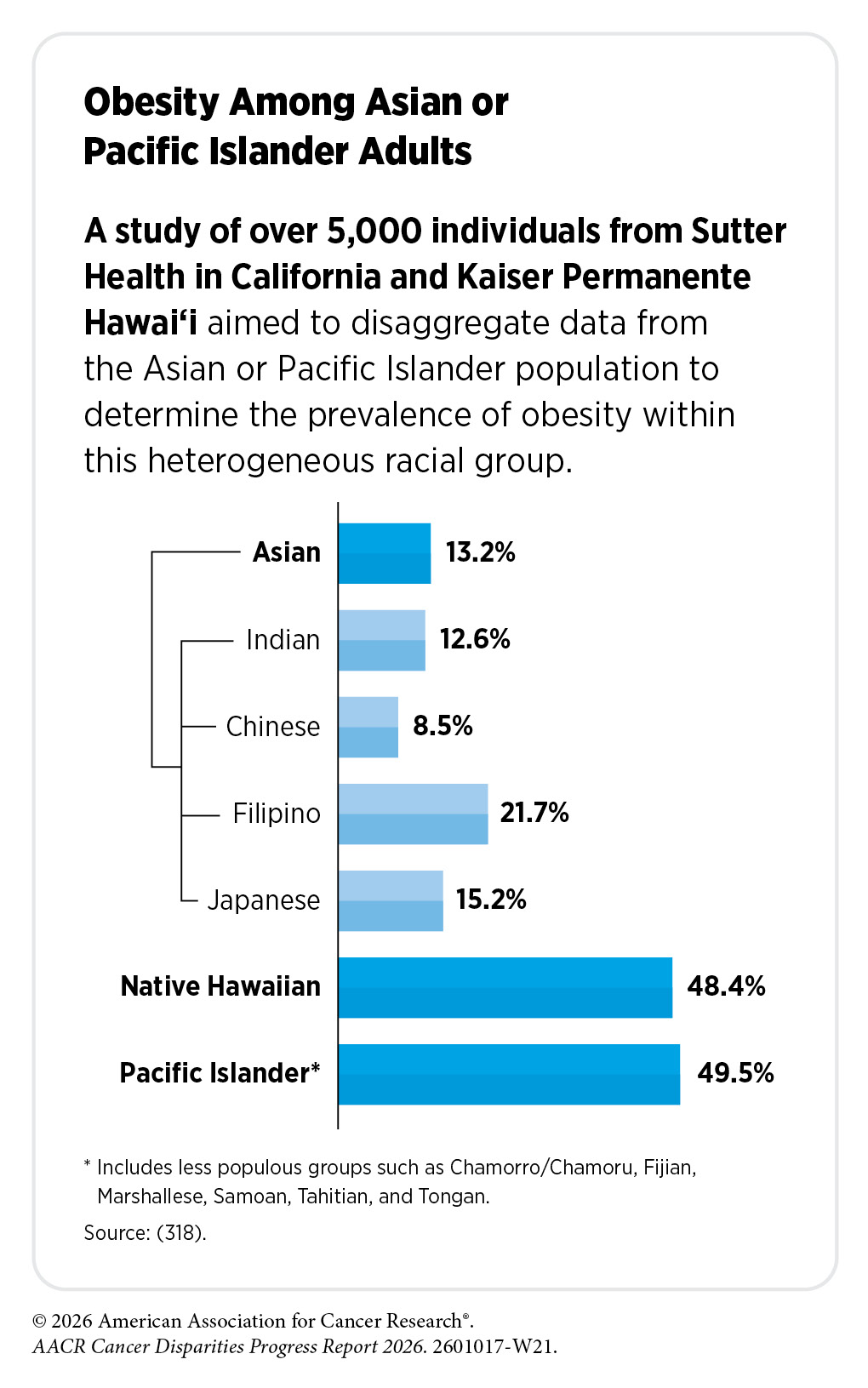
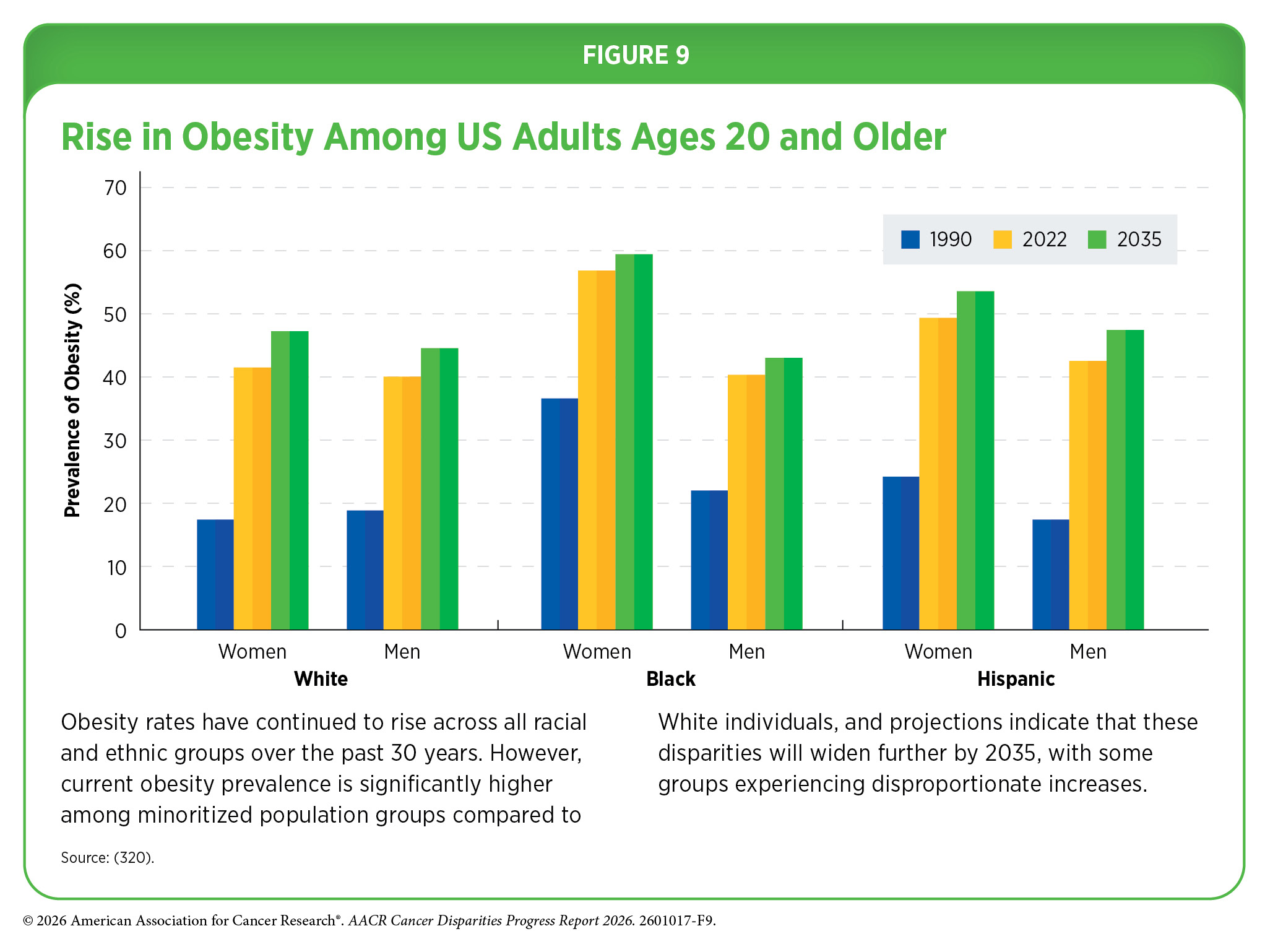
Obesity is shaped by complex and interrelated socioeconomic, environmental, biological, and behavioral factors. Although obesity prevalence has risen across all racial and ethnic groups, some populations have experienced disproportionately steeper increases (see Figure 9). In 2024, obesity prevalence among US adults age 18 and older, was 12.5 percent among Asian individuals, 33 percent among White individuals, 41 percent among AIAN individuals, and 42 percent among NHPI individuals and Black individuals (319)Centers for Disease Control and Prevention. Percentage of angina for adults aged 18 and over, United States, 2019—2024. Accessed: March 31, 2026. . Obesity prevalence was also higher (37.5 percent) among Hispanic adults, compared to non-Hispanic adults (32.5 percent) (319)Centers for Disease Control and Prevention. Percentage of angina for adults aged 18 and over, United States, 2019—2024. Accessed: March 31, 2026. .
Obesity rates also vary by immigrant status. US-born adults have a higher prevalence of obesity (43.2 percent) compared to adults born outside the United States. Among immigrants, those who have lived in the United States for 10 years or longer exhibit significantly higher obesity prevalence than more recent arrivals (33.1 percent vs. 25.5 percent) (291)Bandi P, et al. (2025) Cancer Epidemiol Biomarkers Prev, 34: 836. .
Taken together, these patterns underscore the urgent need for effective and accessible weight loss interventions to mitigate rising obesity rates and reduce associated cancer risks. Although lifestyle interventions, bariatric surgery, and pharmacologic therapies such as glucagon-like peptide-1 (GLP-1) receptor agonists can meaningfully improve outcomes, access to these treatments remains inequitable.
Addressing inequities in access to effective weight loss interventions is essential to reducing the growing burden of obesity-related cancers. Evidence shows that bariatric surgery substantially lowers overall obesity-related cancer incidence and cancer mortality, while newer medical therapies such as GLP-1 receptor agonists show promise for weight management, though their long-term cancer preventive effects—particularly in non-diabetic populations—remain uncertain (321)Wilson RB, et al. (2023) Int J Mol Sci, 24. . Despite their effectiveness, access to both surgical and medical weight loss treatments remain uneven across segments of the US population, potentially limiting their population-level impact.
A recent nationally representative study found that more than 55 percent of Black and Hispanic adults were eligible to receive semaglutide, a type of GLP-1 medication. However, they were also more likely to be uninsured, lack a usual source of care, have lower family income, or have lower educational attainment, all of which could make the medication difficult to access or afford (322)Lu Y, et al. (2022) Journal of the American Heart Association, 11: e025545. . Disparities in access to GLP-1s are also evident among youth. Hispanic and Black adolescents, those living in socioeconomically disadvantaged or rural areas, and individuals insured by Medicaid were significantly less likely to be prescribed GLP-1 therapies (323)Kim C, et al. (2026) JAMA Pediatrics, 180: 334. .
The rising prevalence of obesity in the United States, accompanied by increasing rates of obesity-related cancers, underscores the urgency of ensuring that effective prevention and treatment strategies are accessible to all communities.
Diet
Substantial evidence shows that diets high in calorie-dense, ultra-processed foods and sugar-sweetened beverages, combined with insufficient physical activity, significantly increase obesity and subsequent cancer risk. Poor diet alone is responsible for an estimated 4.2 percent of all cancers, and numerous studies have linked higher intake of ultra-processed foods to increased Group 4792, Grouped objectcancer incidence (110)Morales-Berstein F, et al. (2024) Eur J Nutr, 63: 377. (284)Islami F, et al. (2024) CA Cancer J Clin, 74: 405. (324)Jin Q, et al. (2023) Br J Cancer, 129: 1978. (325)Chang K, et al. (2023) EClinicalMedicine, 56: 101840. . Ultra-processed foods are defined as industrial formulations manufactured from processed substances (e.g., oils, fats, sugars, and proteins) containing little to no whole food (i.e., foods that have not been processed) (326)Monteiro CA, et al. (2019) Public Health Nutr, 22: 936. . Today, approximately 73 percent of the US food supply is composed of ultra-processed products (327)Ravandi B, et al. (2025) Nat Food, 6: 296. .
Consumption of fast food—typically characterized by having high levels of calories, salt, saturated fat, and added sugars, and low nutritional value—is also disproportionately high among certain racial and ethnic minority groups. Between 2017 and 2018, the most recent time frame for which these data are available, an estimated 42.6 percent of Black adults, 36.3 percent of White adults, 34.9 percent of Mexican American adults, and 33.8 percent of Asian adults consumed fast food on a typical day (329)Dunn CG, et al. (2021) American Journal of Preventive Medicine, 61: e197. .
In contrast, dietary patterns rich in fruits and vegetables, whole grains, nuts, and fish are associated with a lower risk of cancers and several chronic health conditions (107)Bui LP, et al. (2024) Am J Clin Nutr, 120: 80. (108)Cai Y, et al. (2024) Am J Clin Nutr, 119: 406. (330)Poorolajal J, et al. (2024) PLoS One, 19: e0305994. . One recent study found that, compared to non-vegetarians, vegetarians and pescatarians had a 45 percent lower risk of stomach cancer, a 25 percent lower risk of certain blood cancers (including Group 4795, Grouped objectnon-Hodgkin lymphoma, Hodgkin lymphoma, and chronic lymphocytic leukemia), and a 21 percent lower risk of colorectal cancer (109)Fraser GE, et al. (2025) Am J Clin Nutr, 122: 535. . Conversely, consumption of red meat and other processed meats have been associated with a 6 percent to 33 percent increased risk of multiple cancers including breast, colorectal, and lung cancers (331)Farvid MS, et al. (2021) European Journal of Epidemiology, 36: 937. (332)Zouiouich S, et al. (2025) Current Developments in Nutrition, 9: 107540. .
Diets higher in fruits and vegetables have consistently been associated with healthier body weight, reduced adiposity, and lower incidence of obesity-related cancers. However, intake remains below recommended levels for much of the US population, particularly among racial and ethnic minority groups and individuals living in low-income or food-insecure communities, where access to affordable fresh produce is often limited. In 2019, the most recent year for which these data are available, only 6.9 percent of Black adults, 10.1 percent of White adults, and 11.0 percent of Hispanic adults consumed the federally recommended daily intake of vegetables (2 to 3 cups) (334)Lee SH, et al. (2022) Morb Mortal Wkly Rep, 71: 1. .
Disparities in diet quality are closely linked to socioeconomic and geographic factors that contribute to food insecurity. The US Department of Agriculture defines food security as “access by all people at all times to enough food for an active, healthy life,” whereas food insecurity occurs when households cannot acquire adequate food because of insufficient financial or other resources (111)Odoms-Young A, et al. (2024) The American Journal of Clinical Nutrition, 119: 850. .
Analyses of nationally representative data indicate that, between 1999 and 2020, the consumption of poor diet declined from 47.9 percent to 33.0 percent among US residents who did not experience food insecurity; however, individuals experiencing food insecurity saw no meaningful improvement during the same period (51.3 percent vs. 48.2 percent) (335)Liu J, et al. (2024) Ann Intern Med, 177: 841. .
Disparities in diet quality are shaped by SDOH (i.e., neighborhood segregation, limited transportation options, and chronic underinvestment in certain communities), which create food deserts where access to affordable, nutritious foods is severely limited (see Understanding and Addressing Drivers of Cancer Disparities). Addressing disparities in diet quality and the associated cancer risk requires a multifaceted approach that includes culturally relevant nutrition education to support healthy food choices, alongside policies and investments that improve the availability, affordability, and accessibility of nutritious foods in underserved communities (336)Silva P, et al. (2023) Nutrients, 15. .
Physical Activity
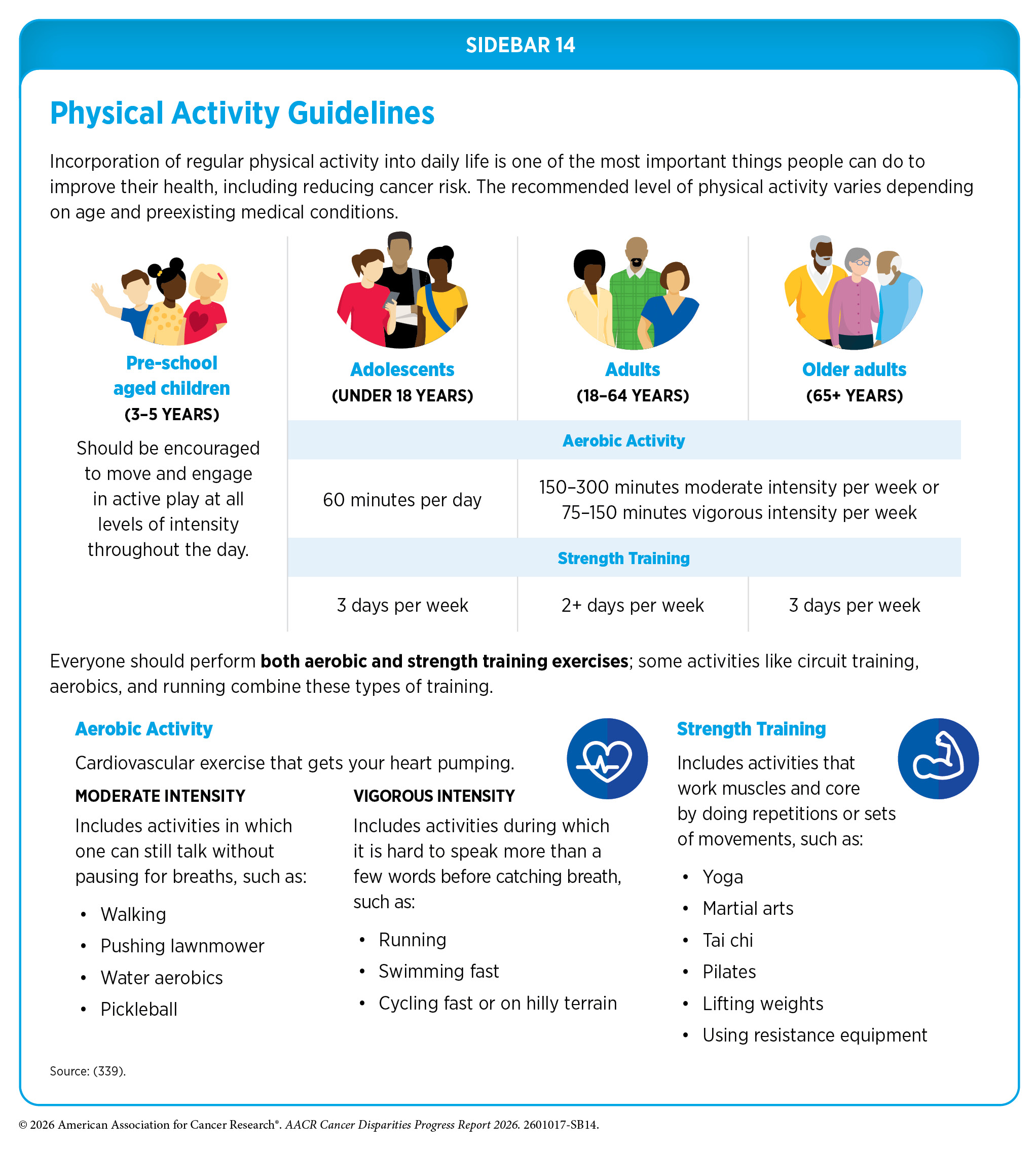
Engaging in higher levels of physical activity can reduce the risk of nine different types of cancer by 10 percent to 25 percent (337)Friedenreich CM, et al. (2021) Mol Oncol, 15: 790. . In 2019, an estimated 16,540 cancer cases in men and 38,030 cases in women in the United States were attributable to physical inactivity (284)Islami F, et al. (2024) CA Cancer J Clin, 74: 405. . In a recent study of more than 85,000 individuals, engaging in either one hour of daily light-intensity activity or moderate-to-vigorous physical activity reduced cancer risk by 6 percent to 13 percent compared to a more sedentary lifestyle (see Sidebar 14) (338)Shreves AH, et al. (2025) British Journal of Sports Medicine, 59: 839. .
Despite the clear health benefits of regular physical activity, substantial disparities persist across racial and ethnic minority groups. Physical inactivity ranges from 18.0 percent to 21.0 percent in Asian, AIAN, and White men, increasing to 26.4 percent in Black men and 31.3 percent in Hispanic men. Physical inactivity is the lowest among Asian and White women (23 percent) but considerably higher among Black, AIAN, and Hispanic women, ranging from 32.3 percent to 36.2 percent. Geographic factors further widen these disparities, with higher levels of physical inactivity observed in rural areas than in urban areas (17)Islami F, et al. (2026) CA Cancer J Clin, 76: e70045. .
Multiple barriers can limit opportunities for physical activity, including low income, lack of affordable fitness facilities, poor neighborhood walkability, limited access to green spaces, inadequate tree canopy cover, and competing family responsibilities (see Understanding and Addressing Drivers of Cancer Disparities) (340)Kegler MC, et al. (2022) Prev Chronic Dis, 19: E40. (341)Patel NA, et al. (2022) Kans J Med, 15: 267. . Tailored strategies—such as culturally responsive fitness programs, accessible community-based activity initiatives, investments in safe neighborhood infrastructure, and workplace- or school-based movement supports—can help reduce these disparities and promote more equitable opportunities for physical activity.
Alcohol Consumption
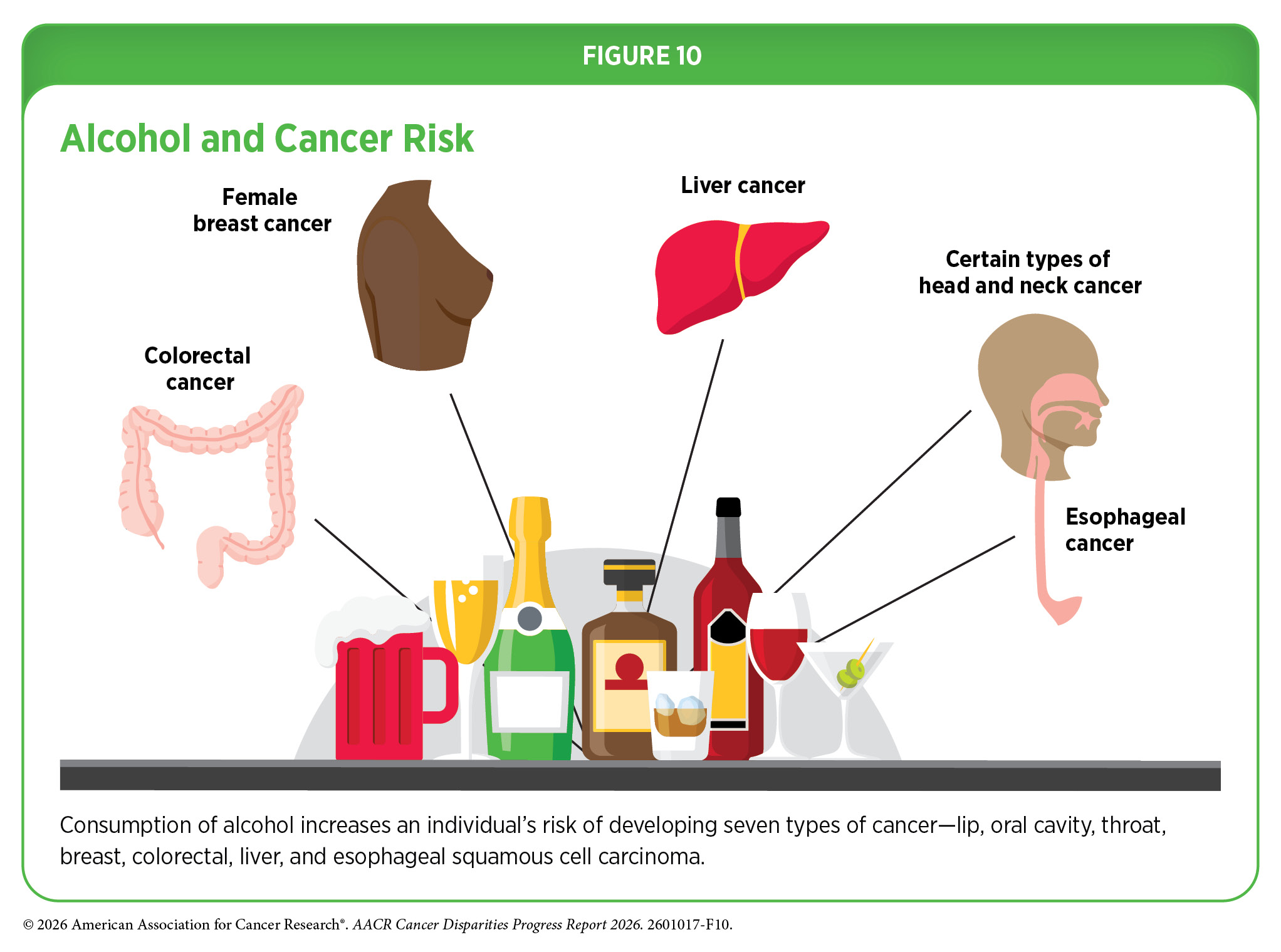
Alcohol consumption increases the risk of seven different types of cancer (see Figure 10) and is associated with more than 200 diseases. The health risks associated with alcohol increase with both the amount consumed and the pattern of drinking. The highest risks are associated with long-term alcohol use and binge drinking, defined as consuming large quantities of alcohol in a short period (342)Jun S, et al. (2023) Epidemiol Health, 45: e2023092. . Even light alcohol intake can elevate the risk of certain cancers. Any level of alcohol consumption increases the risk of cancers of the head and neck, breast, and colon and rectum, while heavy drinking is associated with increased risk of cancers of the stomach, liver, gallbladder, and pancreas; however, additional evidence is needed to confirm causal relationships for some of these sites (343)Bagnardi V, et al. (2015) Br J Cancer, 112: 580. .
In the United States, just over 5 percent of all cancers, or more than 96,000 new cases each year, are attributable to alcohol use. Despite this substantial burden, public awareness of the role of alcohol in cancer remains low. A nationally representative survey found that nearly 53 percent of US adults did not know whether alcohol affects cancer risk (344)Fokom Domgue J, et al. (2025) JAMA Oncology. .
Knowledge gaps were especially pronounced in certain population groups. Black adults were 64 percent more likely to be unaware that alcohol increases cancer risk. Adults with lower educational attainment had nearly three times the likelihood of not knowing about this association. Current cigarette smokers were also less informed, with a 45 percent higher chance of being unaware. In addition, people who believed cancer is not preventable were 74 percent more likely to not know that alcohol can increase cancer risk (344)Fokom Domgue J, et al. (2025) JAMA Oncology. . These findings emphasize the need for clearer public messaging and targeted education efforts to address persistent gaps in awareness of alcohol-related cancer risks (see Figure 10).
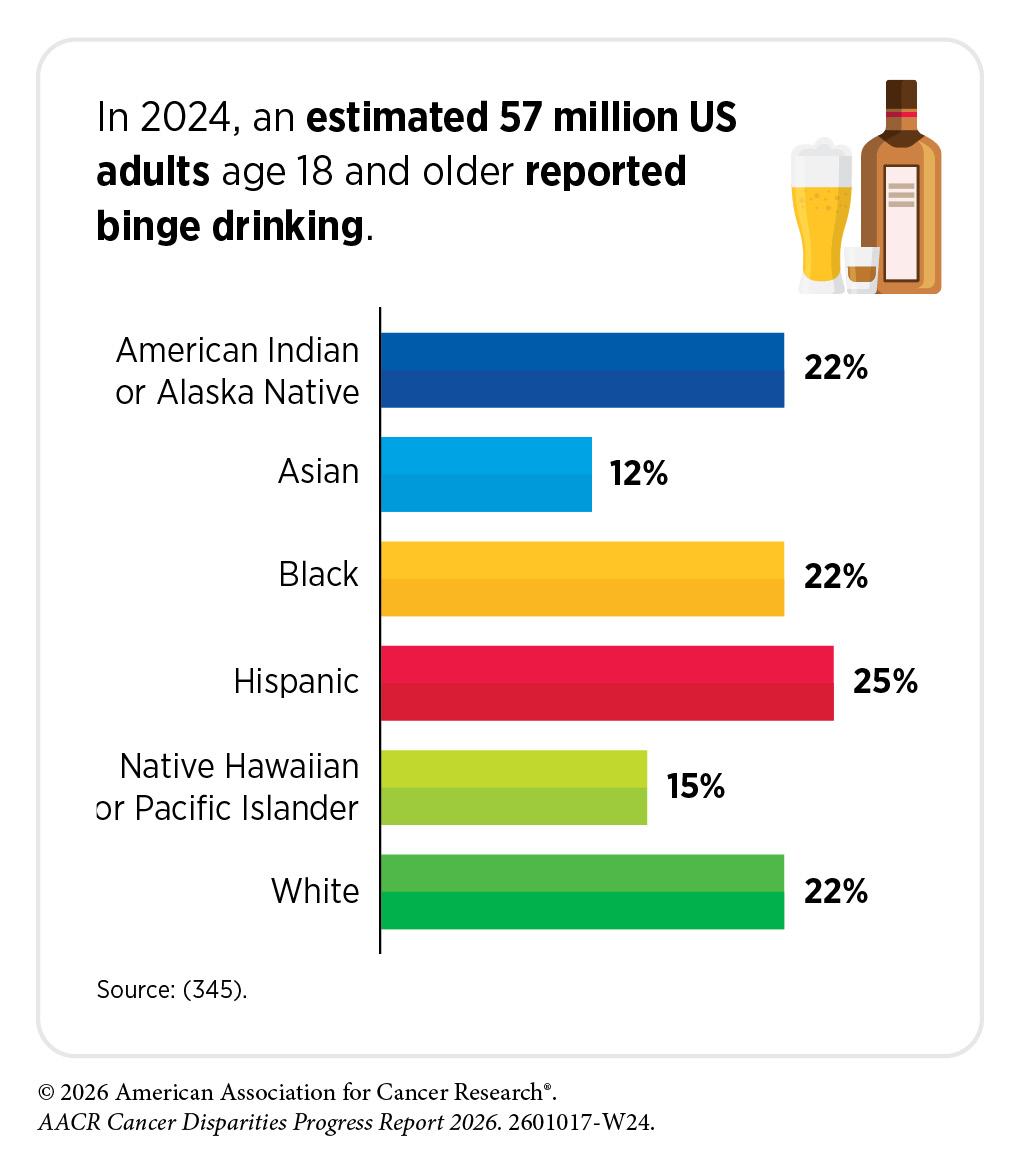
Alcohol use remained widespread in 2024, with nearly 51 percent of adults age 18 and older reported alcohol consumption in the past month (345)National Institute on Alcohol Abuse and Alcoholism. Alcohol Use in the United States: Age Groups and Demographic Characteristics. Accessed: March 31, 2026. . Importantly, drinking patterns vary considerably across demographic groups, reflecting differences in culture, access, social norms, and health education (345)National Institute on Alcohol Abuse and Alcoholism. Alcohol Use in the United States: Age Groups and Demographic Characteristics. Accessed: March 31, 2026. . Individuals who experience structural racism are more likely to binge drink. As one example, recent studies found that structural racism experienced by Black individuals increased the level of binge drinking frequency and smoking (346)Desalu JM, et al. (2019) Addiction, 114: 957. (347)Woodard N, et al. (2025) J Racial Ethn Health Disparities, 12: 3819. .
US veterans have a higher prevalence of alcohol use and alcohol use disorder (AUD) (348)Panza KE, et al. (2022) Drug Alcohol Depend, 231: 109240. . A national survey found that alcohol use was significantly more common among veterans than among civilians (59.2 percent vs. 51.9 percent, respectively) (349)Bachrach RL, et al. (2018) J Subst Abuse Treat, 95: 18. . Lifetime prevalence of AUD followed a similar pattern, with veterans experiencing higher rates than the civilian population (40.8 percent vs. 29.1 percent) (348)Panza KE, et al. (2022) Drug Alcohol Depend, 231: 109240. . Within the veteran population, binge drinking and heavy alcohol use were higher among veterans who served in combat zones compared to those who did not (24.8 percent vs. 19.4 percent for binge drinking; 8.7 percent vs. 6.1 percent for heavy alcohol use) (350)Substance Abuse and Mental Health Service Administration. Mental Health and Substance Use among Veterans. Accessed: March 31, 2026. . Racial differences in the prevalence of AUD in the US veteran population have also been reported. Specifically, Black veterans had the lowest prevalence of AUD compared to White and Hispanic veterans (34.0 percent vs. 42.7 percent and 41.5 percent, respectively) (351)Carr MM, et al. (2021) Am J Addict, 30: 26. .
Together, these findings demonstrate that alcohol consumption contributes substantially to the cancer burden in the United States. Reducing alcohol-related cancer risk will require improved public awareness, targeted prevention strategies for high-risk populations, and structural interventions that address the social and occupational contexts shaping harmful drinking patterns.
Ultraviolet (UV) Exposure
Ultraviolet (UV) radiation—an invisible form of energy emitted by the sun—is a major environmental risk factor for skin cancer. UV radiation also comes from artificial sources such as sunlamps and indoor tanning beds. There are three types of UV rays: UVA, which primarily contribute to skin aging and wrinkling; UVB, which are more likely to cause sunburn; and UVC, which are largely absorbed by Earth’s atmosphere and do not typically reach the surface. Exposure to UV radiation from any source can damage skin cells and lead to the development of skin cancers, including basal cell carcinoma, squamous cell carcinoma, and melanoma, the most aggressive form of the disease.
In the United States, sun exposure and sun protective behaviors vary substantially by race, ethnicity, and rurality. For example, White individuals living in rural areas were more likely than those in urban areas to spend 2 or more hours outdoors during both workdays (42.9 percent vs. 29.1 percent) and non-workdays (72.2 percent vs. 64.8 percent) (352)Dona AC, et al. (2024) Cancer Epidemiol Biomarkers Prev, 33: 608. . In addition, Black and White individuals residing in rural areas were less likely than their urban counterparts to seek shade when outdoors (31.6 percent vs. 43.9 percent and 21.7 percent vs. 26.7 percent, respectively) (352)Dona AC, et al. (2024) Cancer Epidemiol Biomarkers Prev, 33: 608. . Sunburn prevalence also differs by race and ethnicity: White individuals reported rates at approximately 60 percent, individuals identifying as multiracial or another race had rates of 40 percent to 45 percent, and Black and Asian individuals had rates of 10 percent to 25 percent (352)Dona AC, et al. (2024) Cancer Epidemiol Biomarkers Prev, 33: 608. .
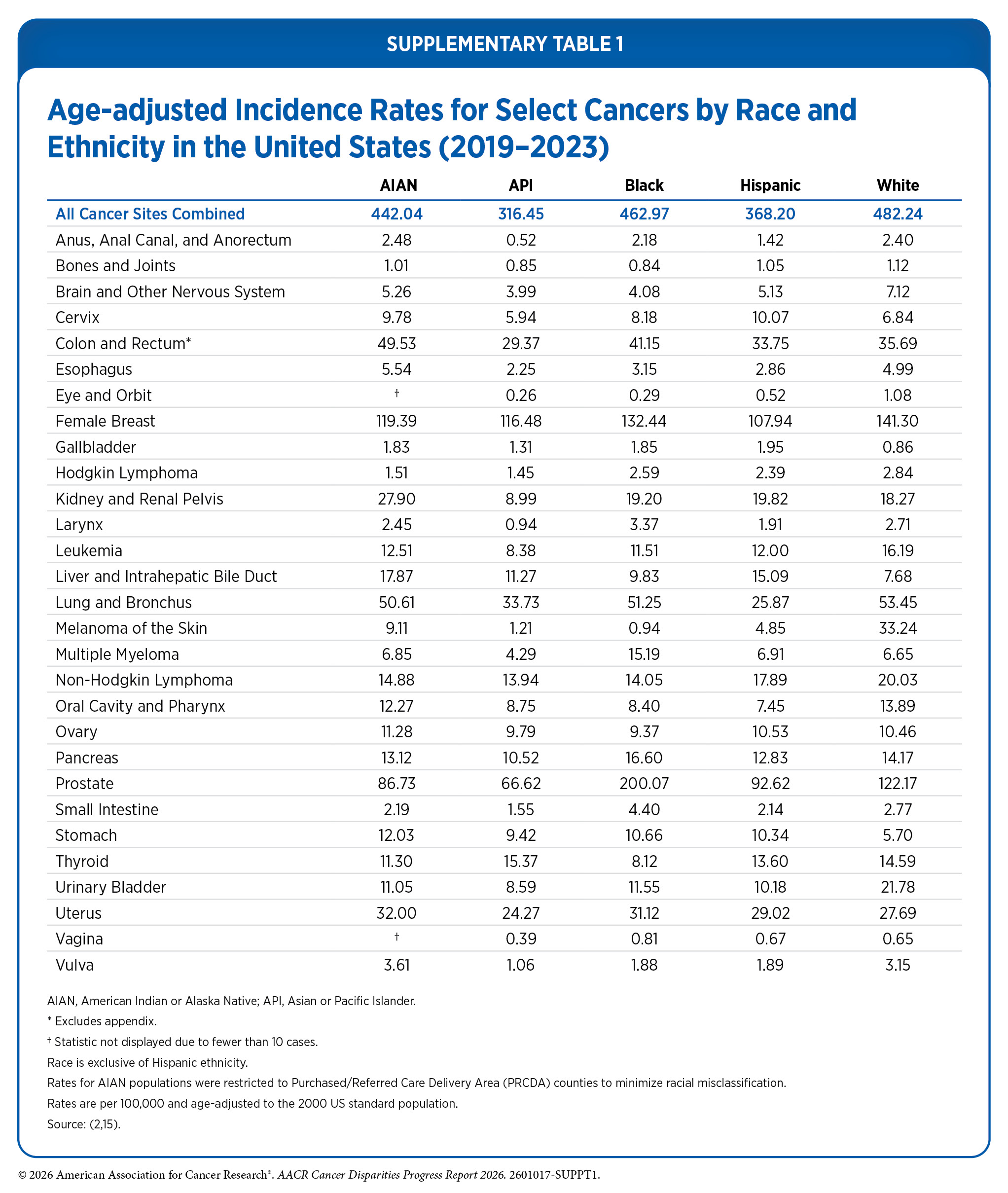
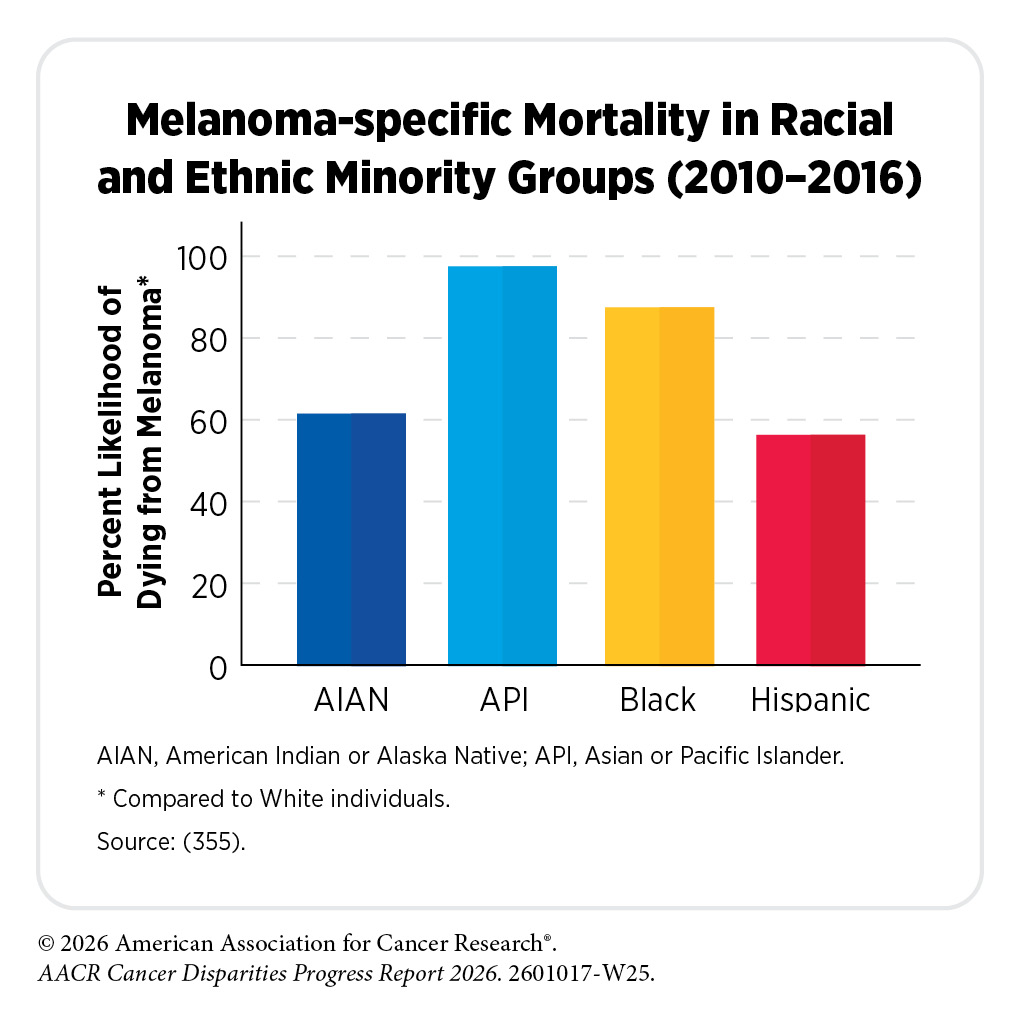
In the United States, more than 33,000 sunburns requiring emergency room care are reported each year (353)National Cancer Institute Cancer Trends Progress Report. Sunburn. Accessed: March 31, 2026. . Experiencing sunburns, especially during childhood and early adulthood, significantly increases the likelihood of developing skin cancer later in life, particularly melanoma. Although melanoma incidence is highest among White individuals and lowest among Black individuals (30.5 vs. 0.9 per 100,000 individuals, respectively; see Supplementary Table 1), substantial disparities in prognosis and outcomes persist. Long-term data from 1975 to 2016 show marked racial and ethnic differences in stage at diagnosis (354)Visser WI, et al. (2025) EJC Skin Cancer, 3: 100730. . The proportion of individuals diagnosed with regional or distant disease was 12.6 percent among White patients, 18.6 percent among AIAN patients, 21.0 percent among Hispanic patients, 28.6 percent among Asian or Pacific Islander (API) patients, and 34.1 percent among Black patients (354)Visser WI, et al. (2025) EJC Skin Cancer, 3: 100730. . Five-year relative survival rates mirror these differences. Between 2016 and 2022, the 5-year survival rate for melanoma was 94.8 percent for White individuals compared to 71.2 percent among Black individuals (2)SEER*Explorer: An interactive website for SEER cancer statistics [Internet]. Surveillance Research Program, National Cancer Institute; 2026 Apr 22. [cited 2026 May 11]. Data source(s): SEER Incidence Data, November 2025 Submission (1975-2023), SEER 21 registries. .
Geographic differences in melanoma outcomes have also been observed. Rural areas tend to have higher-than-average rates of melanoma diagnosed at advanced stages, while urban residents are more likely to be diagnosed at earlier stages, potentially due to geographic differences in access to dermatologic care (356)Zhang K, et al. (2025) JMIR Cancer, 11: e67902. . These disparities underscore the importance of early detection, timely access to high-quality care, and equitable prevention strategies across all communities.
Disparities in skin cancer awareness and prevention behaviors further contribute to worse health outcomes. Perceived risk of developing skin cancer is lowest among racial and ethnic minority groups. One study found that Black and API adults reported the lowest perceived risk (8 percent to 16 percent), compared to White and Hispanic adults (53 percent to 70 percent). Consistent with these perceptions, sunscreen use was lowest among Black individuals relative to other racial and ethnic groups (357)Fliorent R, et al. (2023) Cureus, 15: e33752. . These knowledge gaps are concerning because of the findings that Black, Hispanic, and NHPI populations are more likely to be diagnosed at advanced stages of melanoma, which are associated with poorer outcomes (354)Visser WI, et al. (2025) EJC Skin Cancer, 3: 100730. .
Taken together, disparities in skin cancer awareness and prevention behaviors highlight the urgent need for improved education, tailored prevention efforts, and more equitable access to early detection and treatment to reduce UV exposure and melanoma disparities across all populations.
Infectious Agents
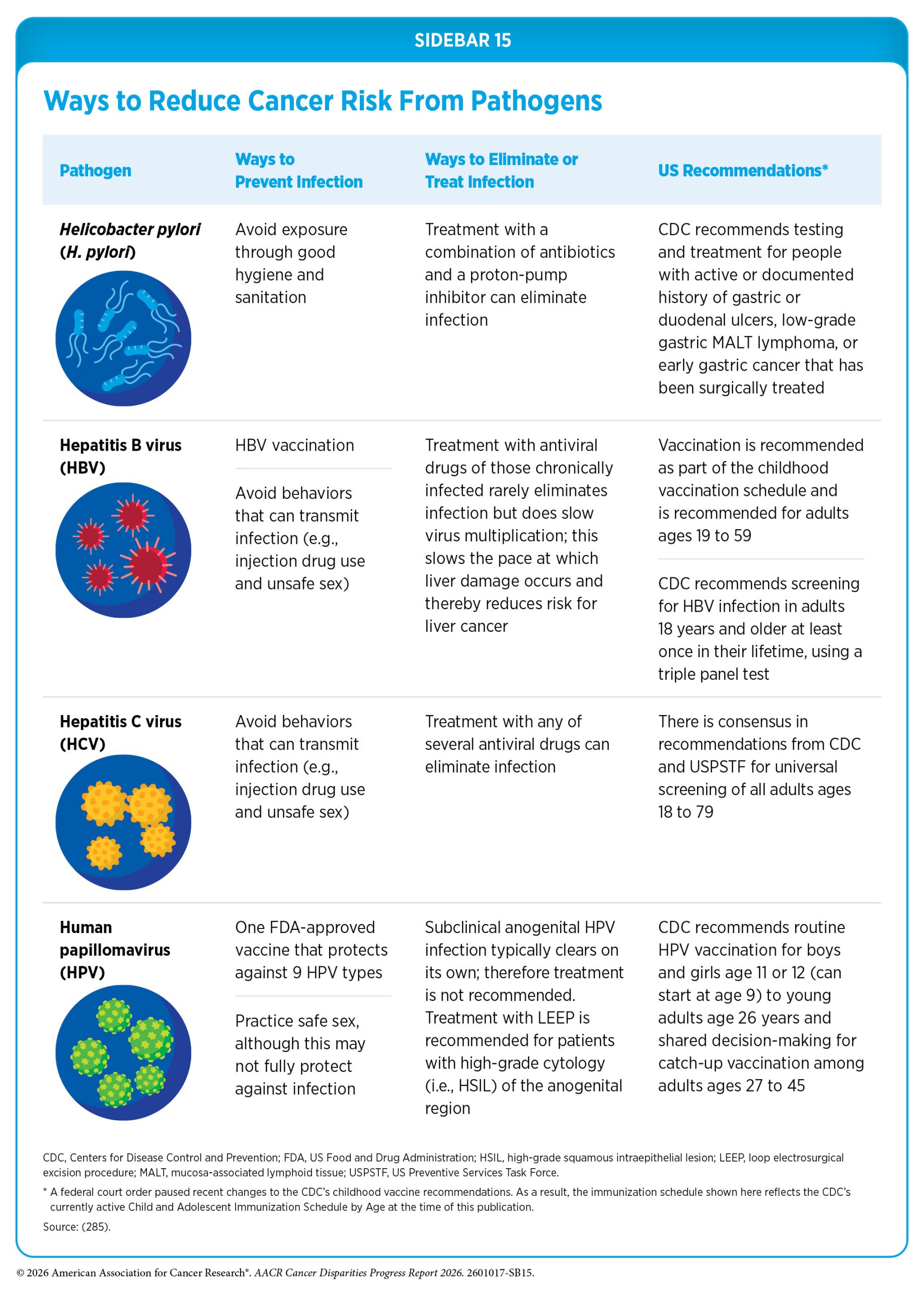
In addition to lifestyle and behavioral factors, infections with certain pathogens can also increase cancer risk. Specific bacteria, viruses, and parasites can alter how cells function, weaken the immune system, or cause chronic inflammation, mechanisms that contribute to cancer development. In the United States, about 3 percent of all cancer cases are attributable to pathogenic infections (284)Islami F, et al. (2024) CA Cancer J Clin, 74: 405. . Globally, the burden is even greater. In 2018, an estimated 13 percent of all cancer cases (approximately 2.2 million) were linked to infections, with more than 90 percent of these cases caused by just four pathogens—Helicobacter pylori (H. pylori), human papillomavirus (HPV), hepatitis B virus (HBV), and hepatitis C virus (HCV) (358)de Martel C, et al. (2020) The Lancet Global Health, 8: e180. . Decades of research have demonstrated that preventive measures, including vaccination and treatment or eradication of existing infections, can significantly reduce cancer risk associated with infectious agents (see Sidebar 15).
Human papillomavirus (HPV)
HPV refers to a group of more than 200 related viruses that are responsible for almost all cervical cancers, 90 percent of anal cancers, and 70 percent of oropharyngeal cancers, as well as most penile, vaginal, and vulvar cancers. While most HPV infections do not lead to cancer, persistent infection with high-risk HPV strains can cause precancerous changes that progress to malignancy. High-risk HPV types account for just under 2 percent of all cancers diagnosed in men and women in the United States (284)Islami F, et al. (2024) CA Cancer J Clin, 74: 405. . Globally, HPV is attributable to 31.4 percent of all cancers caused by infectious agents (358)de Martel C, et al. (2020) The Lancet Global Health, 8: e180. .
HPV prevalence varies significantly across racial and ethnic minority populations. Young Black women, for example, have higher HPV infection rates than young White women (35 percent vs. 25 percent, respectively) (359)Hirth J (2019) Hum Vaccin Immunother, 15: 146. . Differences in HPV prevalence are also evident by nativity. A national survey reported that individuals born in the United States were more likely to have an HPV infection than those born elsewhere; however, among immigrants, Black individuals were more than three times as likely as White individuals to have HPV (360)Cofie LE, et al. (2025) Frontiers in Public Health, Volume 13 – 2025. . These disparities highlight the critical need for effective prevention strategies, with HPV vaccination serving as the most reliable way to prevent infection and reduce HPV-related cancers.
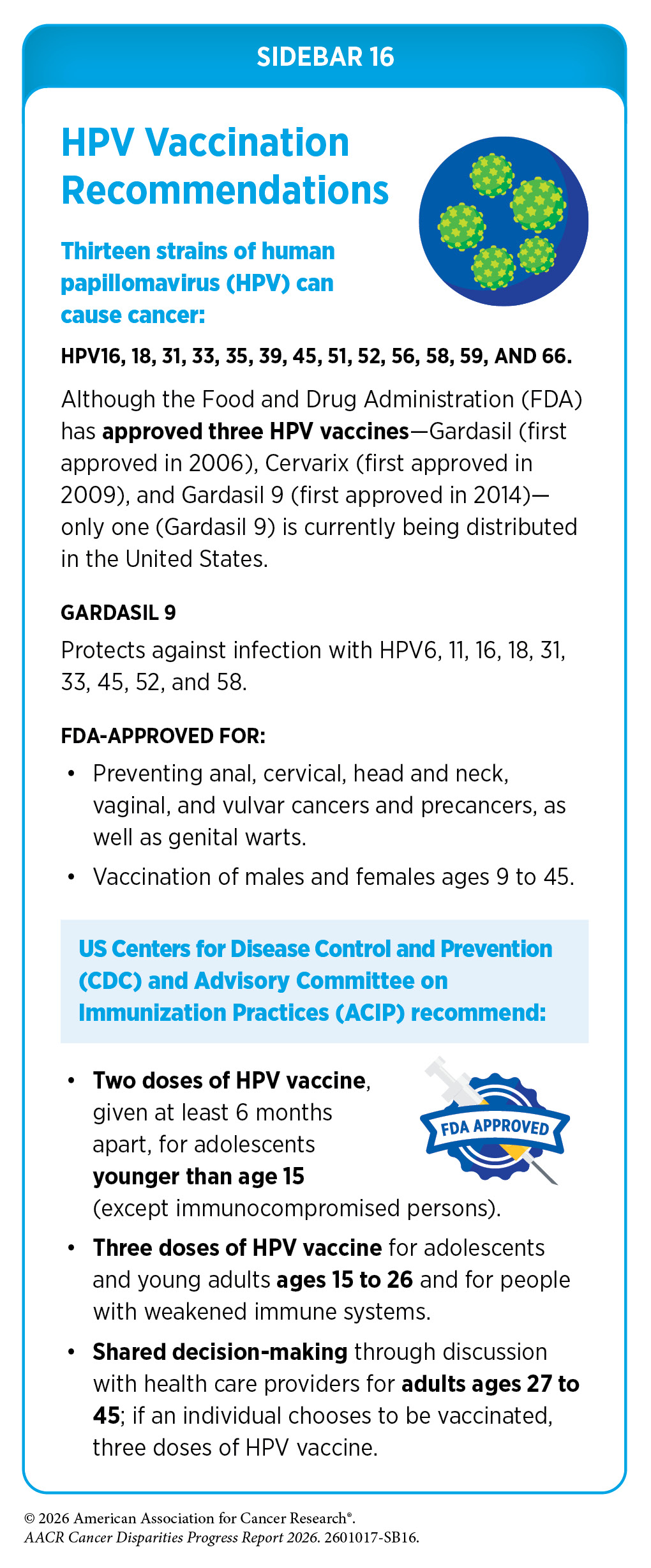
The HPV vaccine is approved for males and females ages 9 to 45, with recommendations for the first doses beginning at age 11 to 12 (see Sidebar 16). There are 13 different types of HPV that can cause cancers; the HPV vaccine currently used in the United States, Gardasil 9, can protect against nine of these HPV strains.
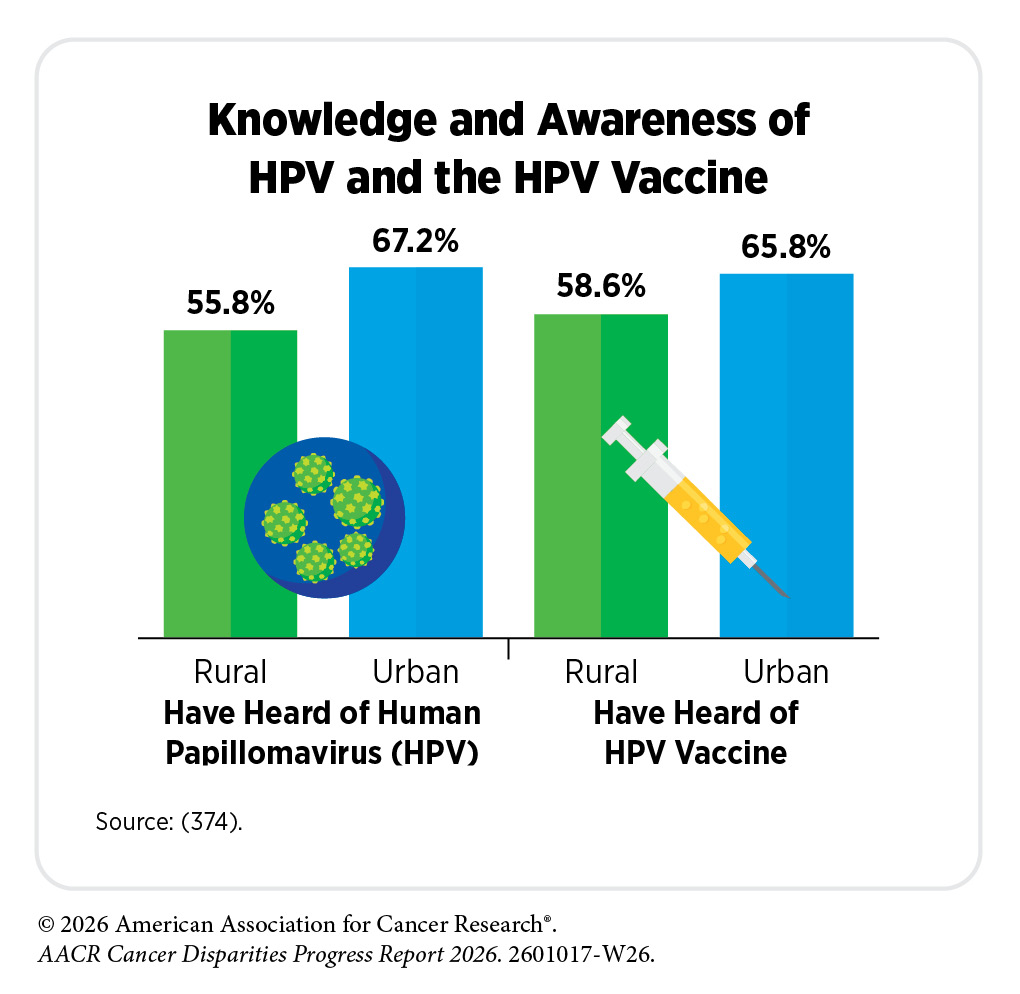
Although HPV vaccination is widely available, only 63 percent of US adolescents are up to date with the recommended vaccine schedule, and uptake remains low across several population groups. Adolescents living in rural areas are less likely to be vaccinated than their urban counterparts (361)Pingali C, et al. (2021) MMWR Morb Mortal Wkly Rep, 70: 1183. (362)Pingali C, et al. (2025) MMWR Morb Mortal Wkly Rep, 74: 466. . Among those who initiated HPV vaccination, a larger proportion of urban adolescents (65.6 percent) had completed all recommended doses compared to rural adolescents (54.8 percent) (362)Pingali C, et al. (2025) MMWR Morb Mortal Wkly Rep, 74: 466. . Completion rates were also higher when parents received a provider recommendation, emphasizing the importance of strong patient–provider communication to support vaccine uptake.
Differences in HPV vaccine uptake are also observed among immigrant populations. A nationally representative survey indicated disparities in uptake by sex, race and ethnicity, nativity, and poverty level. A lower proportion of males were vaccinated than females (37.8 percent vs. 57.2 percent), and non–US-born individuals had lower vaccination rates than US born individuals (31.9 percent vs. 49.7 percent vaccinated) (363)Sokale I, et al. (2025) Vaccines (Basel), 13. . Non–US-born Black individuals were nearly 70 percent less likely to report being vaccinated than non–US-born White individuals, and 73 percent less likely to report HPV vaccination compared to their US-born Black counterparts (363)Sokale I, et al. (2025) Vaccines (Basel), 13. .
Recent evidence indicates that a single dose of the HPV vaccine can provide sufficient protection against the virus, offering an important opportunity to improve vaccination coverage, particularly in communities where completing a three dose schedule is challenging (364)Kreimer AR, et al. (2025) N Engl J Med, 393: 2421. (365)Fokom-Defo V, et al. (2024) The Lancet Global Health, 12: e360. (366)Stanley M, et al. (2024) Vaccine, 42: S16. . A population-based study from Scotland reported that among women born between January 1, 1988, and June 5, 1996, those vaccinated against HPV at 12 or 13 years of age experienced no cases of invasive cervical cancer, regardless of the number of doses received. Among women vaccinated at older ages (14–22 years), receipt of three doses was associated with significantly lower cervical cancer incidence compared to unvaccinated women (2.1 vs. 3.2 per 100,000, respectively) (367)Palmer TJ, et al. (2024) JNCI: Journal of the National Cancer Institute, 116: 857. .
During 2019–2023, Alabama had the third highest cervical cancer mortality rate nationally (7)SEER*Stat Database: Mortality – All COD, Aggregated With State, Total U.S. (1990-2023) , National Cancer Institute, DCCPS, Surveillance Research Program, released February 2025.. In response, the state became the first to implement a coordinated plan aimed at eliminating cervical cancer–related deaths, launching the Operation Wipe Out initiative in 2021 (368)TogetHER for Health. Operation Wipe Out: Statewide Action Plan to Eliminate Cervical Cancer in Alabama. Accessed: March 31, 2026. .
Increased uptake of the HPV vaccine, regardless of the number of doses received, can lead to substantial declines in HPV-related cancer incidence and mortality. In 2020, the World Health Organization launched the global Cervical Cancer Elimination Initiative to accelerate the elimination of cervical cancer (369)Canfell K (2019) Papillomavirus Research, 8: 100170. (370)Gultekin M, et al. (2020) International Journal of Gynecological Cancer, 30: 426. . The initiative aims to have 90 percent of girls fully vaccinated by age 15; 70 percent of women screened; and 90 percent of women diagnosed with cervical disease—precancerous and invasive cancers—treated by 2030 (371)World Health Organization. Global strategy to accelerate the elimination of cervical cancer as a public health problem. World Health Organization; 2020. If achieved, by 2120, 74 million new cancer cases and 62 million cervical cancer–related deaths will be averted (371)World Health Organization. Global strategy to accelerate the elimination of cervical cancer as a public health problem. World Health Organization; 2020.
Collectively, these findings demonstrate that multiple national and international organizations have articulated clear, evidence-based, and achievable plans for eliminating HPV-related cancers (369)Canfell K (2019) Papillomavirus Research, 8: 100170. (371)World Health Organization. Global strategy to accelerate the elimination of cervical cancer as a public health problem. World Health Organization; 2020(372)Wilailak S, et al. (2025) Int J Gynaecol Obstet, 171 Suppl 1: 120. . However, persistent disparities in HPV vaccine uptake highlight an urgent need for equitable access, culturally responsive outreach and education, and stronger clinical and community partnerships to ensure that all populations are protected against HPV-related cancers. Strengthening vaccine uptake remains the most critical and modifiable factor for translating these well-defined strategies into sustained population-level impact (372)Wilailak S, et al. (2025) Int J Gynaecol Obstet, 171 Suppl 1: 120. (373)Tsui J, et al. (2024) Prev Sci, 25: 147. .
Hepatitis B Virus (HBV) and Hepatitis C Virus (HCV)
Chronic infection with hepatitis B virus (HBV) and hepatitis C virus (HCV) can lead to liver cancer and is also a risk factor for other malignancies, including non-Hodgkin lymphoma. Globally, chronic infection with HBV and HCV is the most common cause of liver cancer. In the United States, just over 2,200 new acute HBV cases and approximately 17,650 newly reported chronic HBV cases were documented in 2023 (375)Centers for Disease Control and Prevention. Hepatitis B Surveillance. Accessed: March 31, 2026. . During the same year, nearly 5,000 new acute HCV cases and more than 101,000 chronic HCV infections were reported (376)Centers for Disease Control and Prevention. Hepatitis C Surveillance. Accessed: March 31, 2026. . Both HBV and HCV are significantly underreported; the estimated actual numbers of new acute cases in 2023 were estimated to be approximately 14,400 for HBV and 69,000 for HCV (375)Centers for Disease Control and Prevention. Hepatitis B Surveillance. Accessed: March 31, 2026. (376)Centers for Disease Control and Prevention. Hepatitis C Surveillance. Accessed: March 31, 2026. .

Acute HBV infection rates are highest among individuals ages 40 to 59 years, who accounted for 48 percent of all diagnosed cases in 2023. Rates of acute HBV infection among Black individuals are nearly twice that of White individuals. Chronic HBV infection disproportionately affects API individuals, such as Alan Wang. Rates of chronic HBV infections among API individuals are nearly 10 times that of White individuals (18.9 vs. 1.9 cases per 100,000) (375)Centers for Disease Control and Prevention. Hepatitis B Surveillance. Accessed: March 31, 2026. . Geographic patterns also reveal disparities. States in the eastern and southeastern United States, particularly those in or bordering the Appalachia region, report the highest HBV rates, aligning with the higher liver cancer burden observed in this region (375)Centers for Disease Control and Prevention. Hepatitis B Surveillance. Accessed: March 31, 2026. (377)Burus T, et al. (2025) Journal of the American College of Surgeons, 240: 425. .
Similar disparities are seen with HCV infection. Acute HCV cases are most commonly diagnosed among adults ages 30 to 39 years, with the highest rates reported in AIAN populations, who experience infection rates more than twice those of White individuals. Chronic HCV infection is most prevalent among individuals ages 30 to 49 years, and the rate of new chronic infections is also highest among AIAN populations, reaching 99.4 per 100,000 in 2023, in line with the high rates of liver cancer in this population (376)Centers for Disease Control and Prevention. Hepatitis C Surveillance. Accessed: March 31, 2026. (378)Jing W, et al. (2026) JHEP Reports, 8: 101754. (379)Abboud Y, et al. (2024) J Clin Transl Hepatol, 12: 172. . Mortality from HCV-related causes is highest among AIAN individuals and Black individuals, with death rates 3.2 times and 1.7 times higher, respectively, than those observed among White individuals (376)Centers for Disease Control and Prevention. Hepatitis C Surveillance. Accessed: March 31, 2026. .
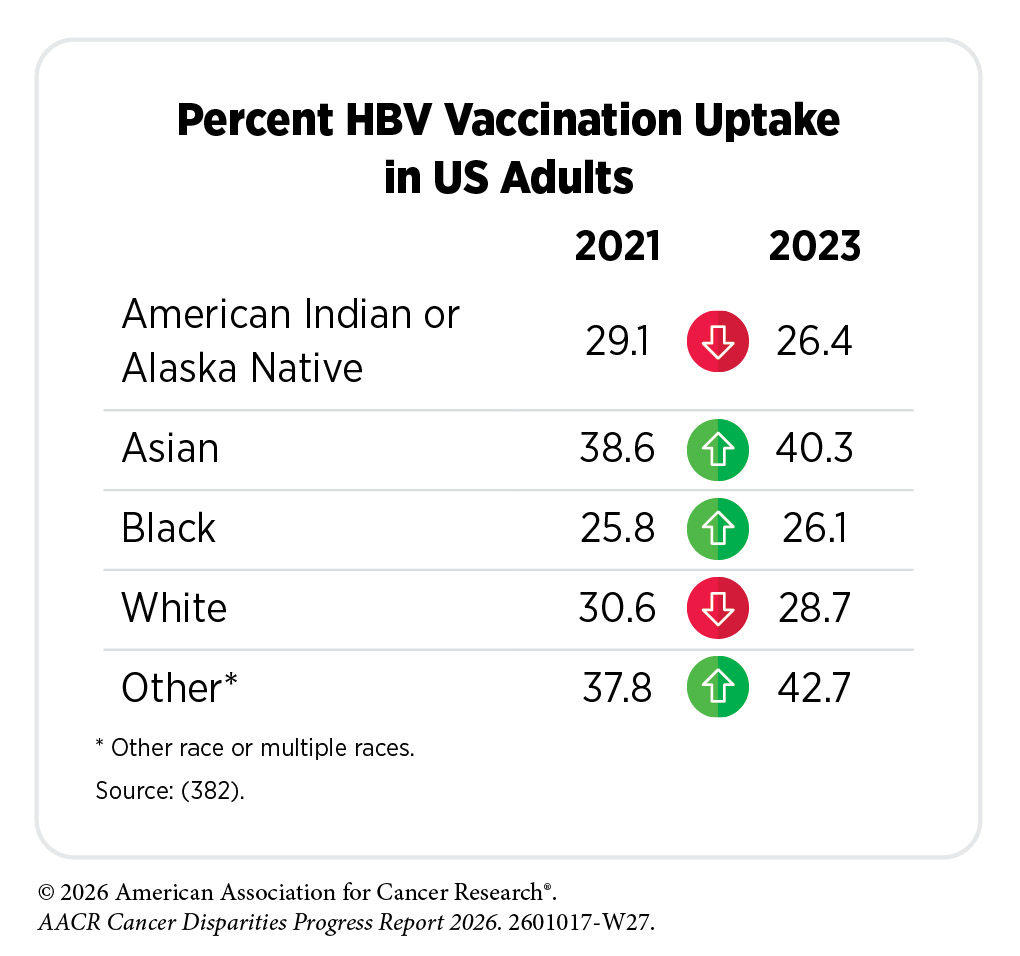
As with HPV, prevention remains the most effective strategy and increasing access to and uptake of HBV vaccination is essential for reducing the burden of HBV-related disease and the cancers it causes. To support national efforts to reduce viral hepatitis, the US Department of Health and Human Services developed The Viral Hepatitis National Strategic Plan: A Roadmap to Elimination 2021-2025, which outlines a coordinated approach to eliminate viral hepatitis in the United States by 2030 (380)US Department of Health and Human Services. Viral Hepatitis National Strategic Plan for the United States: A Roadmap to Elimination (2021–2025). Washington, DC. Accessed: March 31, 2026. .
The plan goals include preventing new infections, improving health outcomes for people living with viral hepatitis, strengthening surveillance and data systems, and fostering integrated, coordinated efforts across partners and stakeholders. A key component of the plan is reducing disparities and advancing health equity. Within the goal of preventing new infections, a top priority is the development of a novel HCV vaccine, an important step toward reducing the long-term burden of HCV disease and achieving national elimination goals. By 2030, CDC aims to reduce HBV-related mortality by 65 percent among API populations; similarly, a 65 percent reduction in HCV-related deaths is expected among AIAN and Black populations (381)Centers for Disease Control and Prevention. 2025 Strategic Plan. Division of Viral Hepatitis. Accessed: March 31, 2026. .
Helicobacter pylori (H. pylori)
Helicobacter pylori (H. pylori) is a type of bacteria that can cause stomach cancer if left untreated. Rates of H. pylori infection are disproportionately higher among racial and ethnic minority groups in the United States. A recent study of over 750,000 individuals tested for H. pylori between 2000 and 2019 found higher positivity among adults age 70 years and older; men; individuals identifying as Asian, Black, or Hispanic; people with a non–English language preference; those living in areas with lower levels of college attainment; and individuals who were overweight or obese (383)Li D, et al. (2024) Gastro Hep Adv, 3: 749. .
Similar trends were observed in a study within the Veterans Health Administration. H. pylori infection rates were highest in the South—especially Texas, Alabama, Mississippi, Kentucky, and Georgia—where several regions exceeded 40 percent (384)Shah SC, et al. (2024) Clin Gastroenterol Hepatol, 22: 42. . H. pylori infection leads to chronic inflammation of the stomach lining, which over time increases the risk of developing gastric adenocarcinoma and gastric mucosa associated lymphoid tissue (MALT) lymphoma—a rare form of non-Hodgkin lymphoma. Black individuals remain at an increased risk of stomach cancer compared to White individuals and have nearly double the mortality rate for the disease. This disparity may be partly attributable to a higher prevalence in Black individuals of H. pylori strains expressing cytotoxin-associated gene A (CagA), a cancer-promoting protein injected into gastric epithelial cells by the bacterium (2)SEER*Explorer: An interactive website for SEER cancer statistics [Internet]. Surveillance Research Program, National Cancer Institute; 2026 Apr 22. [cited 2026 May 11]. Data source(s): SEER Incidence Data, November 2025 Submission (1975-2023), SEER 21 registries. (385)Brown H, et al. (2022) Gastro Hep Adv, 1: 857. . In fact, a recent review of US studies found that the prevalence of H. pylori CagA was substantially higher among Black individuals (ranging from 62 percent to 90 percent) than among White individuals (ranging from 19 percent to 77 percent) (385)Brown H, et al. (2022) Gastro Hep Adv, 1: 857. . Further, racially and ethnically minoritized individuals also have greater difficulty eliminating the infection after treatment, further compounding disparities in stomach cancer risk and outcomes; although the underlying reasons are not fully understood, they may reflect a complex interplay of inherited genetic variation, immune response, and other social and environmental factors (2)SEER*Explorer: An interactive website for SEER cancer statistics [Internet]. Surveillance Research Program, National Cancer Institute; 2026 Apr 22. [cited 2026 May 11]. Data source(s): SEER Incidence Data, November 2025 Submission (1975-2023), SEER 21 registries. (385)Brown H, et al. (2022) Gastro Hep Adv, 1: 857. (386)Rammohan R, et al. (2023) Cureus, 15: e43080. . Additional contributing factors may include poor treatment adherence, antibiotic resistance, high gastric acidity, greater bacterial load, and reduced sensitivity of certain H. pylori strains to antibiotics (386)Rammohan R, et al. (2023) Cureus, 15: e43080. .
Nonetheless, treatment of H. pylori infection significantly reduces the risk of developing stomach cancer (387)Kumar S, et al. (2020) Gastroenterology, 158: 527. . Although H. pylori–associated stomach cancer has declined overall in the past two decades, these reductions have not been equally experienced across population groups, with Black and AIAN individuals continuing to bear a disproportionate burden (2)SEER*Explorer: An interactive website for SEER cancer statistics [Internet]. Surveillance Research Program, National Cancer Institute; 2026 Apr 22. [cited 2026 May 11]. Data source(s): SEER Incidence Data, November 2025 Submission (1975-2023), SEER 21 registries. . These findings highlight the need for tailored screening, timely diagnosis, and equitable treatment strategies, particularly in underserved communities facing elevated risk and persistent barriers to care.
Environmental Exposures
Environmental exposures, including sunlight, chemical pollutants, radiation, and sources of chronic stressors, substantially contribute to cancer risk and are shaped by the places where people live, work, and play. These places constitute the built environment, which refers to the physical surroundings of a neighborhood and includes elements such as transportation systems, infrastructure quality, clean air and water, adherence to radon and asbestos regulations, access to healthy food, community gardens, walkability, and public services and policies (see Understanding and Addressing Drivers of Cancer Disparities). Environmental exposures arising from these surroundings or from occupational settings often mirror broader patterns of structural inequity and can significantly affect human health, including increased cancer risk.
This section focuses on the physical environment and highlights disparities in exposure to toxic substances, particularly environmental carcinogens, that are associated with increased cancer risk and poorer cancer outcomes. Unlike many behavioral or lifestyle factors, environmental exposures are often outside an individual’s control. Reducing exposure typically requires coordinated regulation and enforcement at the local, state, or national levels, highlighting the importance of public policy and environmental justice.
An increasing concern among public health experts centers on climate change, which refers to long-term shifts in global temperatures and weather patterns driven largely by human activity. Strong scientific evidence shows that climate change can worsen exposure to known carcinogens (388)National Oceanic and Atmospheric Administration. Impacts, Risks, and Adaptation in the United States: Fourth National Climate Assessment, Volume II. Accessed: March 31, 2026. . For example, wildfires in the western United States and Canada—whose frequency and intensity have increased in recent years—have elevated exposure to certain metal toxins, including carcinogenic forms of chromium linked to increased cancer risk (389)Bernicker E, et al. (2024) JCO Oncology Practice, 20: 178. . Individuals living in rural communities or participating in agricultural and other outdoor employment, firefighting, and emergency response activities may face particularly elevated risks as wildfire conditions intensify.
Exposure to pollutants at levels exceeding safety thresholds can increase the risk of several diseases, including cancer. Environmental carcinogens—substances present in air, water, soil, and consumer products—include arsenic, asbestos, radon, lead, ionizing radiation, heavy metals, and endocrine-disrupting chemicals. To better understand and address these threats, initiatives such as the Cohorts for Environmental Exposures and Cancer Risks (CEECR) are building collaborative infrastructures to support integrated scientific research. These efforts aim to deepen understanding of how environmental exposures influence cancer development and how genetic, behavioral, and structural factors modify risk across diverse populations. Other initiatives include the Community Impact of Wildfires and Cancer study, which is a collaboration between academic organizations and community-based partner organizations in California’s Central Valley to investigate solutions across levels (community member, clinician, payer, policymakers) to address the adverse health impacts of air pollution (390)Stanford Cancer Institute. SCI 2022 Equity Impact Research Grant Challenge Award. Accessed: March 31, 2026. .
Ionizing Radiation
NCI defines ionizing radiation as a type of high energy radiation that has enough energy to remove an electron—negative particle—from an atom or molecule, causing it to become ionized. Ionizing radiation can cause changes in cells and damage DNA (see Influences Inside the Cell) (391)Patel R (2024) JCO Glob Oncol, 10: e2400455. . This damage can increase cancer risk and may result from exposure to natural sources, such as radon and cosmic rays, as well as medical imaging procedures including X-ray, computed tomography (CT), and positron emission tomography (PET) scans. High dose exposures—such as those from nuclear accidents or atomic weapons—can cause immediate and severe health effects, including acute radiation sickness, organ damage, and death.
From 1946 to 1958, inhabitants of the US-affiliated Pacific Islands—particularly the Northern Marshall Islands—were exposed to ionizing radiation from US nuclear weapons testing. These exposures have been linked to increased rates of thyroid, breast, and hematologic cancers (392)Moore MA, et al. (2010) Asian Pac J Cancer Prev, 11 Suppl 2: 99. Residents of affected atolls were forcibly relocated during the nuclear testing period, and the health consequences persist to this day (391)Patel R (2024) JCO Glob Oncol, 10: e2400455. . To help mitigate the adverse effects of nuclear testing, the US Department of Energy established the Republic of the Marshall Islands Special Medical Care and Logistics Program to provide ongoing medical care and logistical support for individuals from Rongelap and Utrik exposed during the 1954 “Bravo” thermonuclear test. In 2024, 62 individuals were eligible for radiation-related cancer screening and follow-up care, of whom 76 percent utilized program services (393)Department of Energy. Republic of the Marshall Islands Special Medical Care and Logistics Program Activities. Fiscal Year 2024. Accessed: March 31, 2026. .
While the Marshall Islands represent a well-documented example of population-level exposure to ionizing radiation, other communities across the United States—including nuclear workers, residents near contaminated sites, and military veterans—have also experienced harmful radiation exposures. These exposures can have long lasting health effects and continue to contribute to persistent cancer disparities.
Radon
Radon is a naturally occurring radioactive gas formed from the breakdown of uranium in soil, rock, and water. It can seep into homes through cracks in floors, walls, and gaps around pipes, wires, or sump pumps. Radon levels vary widely by geography and tend to be highest in areas with greater concentrations of radioactive ore. In addition, byproducts from historical uranium mining, particularly in the US Southwest, have contributed to elevated radon levels in surrounding communities (394)Yazzie SA, et al. (2020) Int J Environ Res Public Health, 17. , disproportionately affecting AIAN tribal communities who live in these areas (395)Centers for Disease Control and Prevention. Raising Radon Awareness in Tribal Communities. Accessed: March 31, 2026. .
In the United States, an estimated 83.8 million people live in homes with radon concentrations above the action level of 148 becquerels per cubic meter (Bq/m³)—equivalent to one radioactive decay per second in a cubic meter of air—at which the US Environmental Protection Agency (EPA) recommends mitigation (396)Li L, et al. (2025) Proc Natl Acad Sci U S A, 122: e2408084121. . From 2001 to 2021, average community-level radon concentrations exceeded the action level in many regions such as eastern Pennsylvania, central Ohio, and a continuous band across eastern North Dakota, eastern South Dakota, western Iowa, and eastern Nebraska. Surrounding areas also showed elevated levels, ranging between 111 and 148 Bq/m³ (396)Li L, et al. (2025) Proc Natl Acad Sci U S A, 122: e2408084121. .
Since the late 1980s, EPA has recommended radon testing and the installation of an active radon mitigation system when indoor radon levels exceed 148 Bq/m³. However, not all households are able to comply with these recommendations. Recent evidence shows that radon testing rates are substantially lower in communities experiencing socioeconomic disadvantages. Area-level poverty, a high proportion of single-parent households, renter-occupied housing, overcrowding, limited vehicle access, and lower levels of educational attainment were all associated with reduced radon testing rates (397)Yang Z, et al. (2024) J Environ Radioact, 277: 107460. . Further, the average cost of a radon mitigation system—typically ranging from $2,000 to $4,000—is prohibitive for many households, particularly those already disproportionately affected by elevated radon exposure. These financial barriers further reinforce structural disparities in environmental health protections.
Pollution and Endocrine-disrupting Chemicals
Hazardous materials present in both indoor and outdoor air, as well as in drinking water, can elevate the risk of developing cancer. Air pollution refers to contamination of indoor or outdoor environments by chemical, physical, or biological agents that alter the natural atmospheric composition. Major air pollutants include carbon monoxide, ozone, nitrogen dioxide, sulfur dioxide, and particulate matter (PM)—a mixture of solid particles and liquid droplets suspended in the air. Exposure to these substances has been associated with an increased risk of cancers of the lung (398)Luo G, et al. (2025) Lancet Respir Med, 13: 348. (399)LoPiccolo J, et al. (2024) Nat Rev Clin Oncol, 21: 121. (400)Zhang Y, et al. (2025) BMC Public Health, 25: 1260. (401)Hill W, et al. (2023) Nature, 616: 159. , breast (402)Wu AH, et al. (2025) J Clin Oncol, 43: 273. , and more recently, skin (403)Chan FY, et al. (2025) PLOS Glob Public Health, 5: e0004357. . These associations emphasize the importance of environmental quality as a determinant of cancer outcomes.
The endocrine system consists of glands and organs that produce and release hormones into the bloodstream, where they regulate numerous bodily functions. Endocrine-disrupting chemicals (EDCs) may be naturally occurring or human made, and can mimic, block, or interfere with the body’s hormones. EDCs such as per- and poly-fluoroalkyl substances (PFAS) (see Sidebar 17) and polybrominated diphenyl ethers have been linked to an increased risk of thyroid and liver cancers, and certain types of lymphoma, as well as higher cancer mortality (404)van Gerwen M, et al. (2023) EBioMedicine, 97: 104831. (405)Liu B, et al. (2024) JAMA Netw Open, 7: e243127. (406)Rhee J, et al. (2024) Environ Int, 192: 109058. . More recently, a population-based study in California showed increased risk of brain tumors, leukemia, neuroblastoma, and retinoblastoma among children who lived in areas with PFAS (PFOS/PFOA) contamination (407)Tanghal RB, et al. (2026) Environ Sci Technol, 60: 2816. (408)Binczewski NR, et al. (2026) J Expo Sci Environ Epidemiol. .
Geographically, PFAS contamination in drinking water has been widespread near military sites, airports, industrial sites, and wastewater treatment plants—facilities that are disproportionately located near low-income communities. Additionally, PFAS exposure from fast-food packaging disproportionately affects Black individuals compared to White individuals, as Black populations are more likely to live in neighborhoods with greater access to fast-food restaurants (411)James P, et al. (2014) Health Place, 29: 10. (412)Santaliz Casiano A, et al. (2022) Endocrinology, 163. . Use of parabens—often found in personal care and hair products—is more common among ethnically minoritized populations, contributing to unequal patterns of chemical exposure (413)Johnson PI, et al. (2022) J Expo Sci Environ Epidemiol, 32: 864. .
Organochlorine (OC) pesticides, although banned in the United States in the 1970s, were widely used from the 1940s through the 1960s as agricultural insecticides and for vector control. Despite the ban, these chemicals persist in soil, water, and air and can cause endocrine dysfunction. OC pesticide levels found in the blood are higher among Black and Asian women compared to White women. Recent Hispanic immigrants also have higher levels of OC pesticides than longer-term US counterparts, suggesting important international exposure disparities (414)Weiss MC, et al. (2023) Endocrinol Metab Clin North Am, 52: 719. .
Occupational Exposures
Because of elevated exposure to carcinogens, certain occupations—such as firefighting, industrial painting, and jobs in environments like iron and steel foundries or around welding fumes—have been classified by IARC as Group 1 carcinogenic occupations exposures, meaning they are known to cause cancer in humans (415)Baan R, et al. (2009) Lancet Oncol, 10: 1143. . To reduce risk, workers should consistently use personal protective equipment and ensure it is properly decontaminated after exposure to carcinogens and other hazardous substances.
Beyond direct carcinogenic exposures, other occupational factors, including lack of sleep and night-shift work, have also been linked to increased risks of developing certain types of cancers and other chronic diseases, including diabetes and obesity (416)McDermott JE, et al. (2024) J Proteome Res, 23: 1547. . Approximately 11 million adults in the United States regularly work night shifts, and certain population groups are disproportionately represented in these roles. Men, Black individuals, and adults with only a high school education are all more likely to work night shifts (417)National Toxicology P. NTP Cancer Hazard Assessment Report on Night Shift Work and Light at Night. Research Triangle Park (NC): National Toxicology Program; 2021. These disparities in work schedules may contribute to disproportionately higher burdens of cancer and chronic disease among populations already facing structural disadvantages.
Occupational exposures in specific industries further compound these risks. In a historic study of steel workers, Black workers were disproportionately assigned to coke ovens—industrial furnaces used to bake raw coal in a low-oxygen environment. For example, 89 percent of Black plant employees work on coke ovens compared to 31 percent of White workers. Among the coke oven workers with 5 or more years of exposure, 70 percent of whom were Black, the risk of lung cancer was 10 times higher than among unexposed steel workers. Elevated risks of kidney and skin cancers were also observed, particularly among Black employees (418)Collatuzzo G, et al. (2022) Cancers (Basel), 14. (419)Michaels D (1983) J Natl Med Assoc, 75: 1014.
Disparities in occupational exposures also extend to immigrants, particularly women diagnosed with breast cancer. A recent study assessing breast cancer–relevant occupational exposure to chemicals among immigrant women found that many were employed as house cleaners, nurses, cashiers, janitors, and care aides (421)Knox KE, et al. (2026) Journal of Exposure Science & Environmental Epidemiology, 36: 355. . Of these, nurses and those in closely related occupations such as nursing assistants and home health aides were exposed to the highest number of harmful chemicals, including antimicrobials, cleaning products, fragrances, and phthalates, as well as possible exposures to plastics, parabens, pharmaceuticals, antineoplastic drugs, and alkylphenols (421)Knox KE, et al. (2026) Journal of Exposure Science & Environmental Epidemiology, 36: 355. . House cleaners were commonly exposed to alkylphenols, antimicrobials, cleaning agents, fragrances, phthalates, solvents, plastics, and pesticides (421)Knox KE, et al. (2026) Journal of Exposure Science & Environmental Epidemiology, 36: 355. .
Hormonal Factors
Hormonal factors play an important role in the development of several cancers, particularly breast and gynecologic cancers. Cancer risk can be influenced by lifetime exposure to naturally occurring hormones in the body, as well as hormones used in medications or therapies. This section highlights how reproductive history, breastfeeding, hormone replacement therapy, and gender-affirming hormone therapy shape patterns of hormone exposure and may contribute to differences in cancer risk across populations.
Family Planning, Pregnancy, and Breastfeeding
Research shows that a woman’s risk of developing certain gynecologic cancers is strongly influenced by reproductive factors, such as oral contraceptive use, pregnancy, and breastfeeding, all of which affect lifetime exposure to estrogen and progesterone. Oral contraceptive use has been associated with a slightly increased risk of breast and cervical cancers, but a reduced risk of endometrial and ovarian cancers. More recently, one study reported that hormonal contraceptive use was associated with an approximately 30 percent increased risk of breast cancer among women with BRCA1 gene mutations (422)Phillips KA, et al. (2025) J Clin Oncol, 43: 422. . Evidence also indicates that women who have given birth have a lower risk of developing estrogen receptor (ER)–positive tumors than women who have never given birth; however, this protective effect typically emerges a decade or more after the last pregnancy (423)Nichols HB, et al. (2019) Ann Intern Med, 170: 22. (424)Ambrosone CB, et al. (2020) Cancer Res, 80: 4871. (425)Jung AY, et al. (2022) J Natl Cancer Inst, 114: 1706. .
Breastfeeding, specifically lactation, has been shown to reduce the risk of both breast and ovarian cancers (426)Millikan RC, et al. (2008) Breast Cancer Res Treat, 109: 123. (427)Lord SJ, et al. (2008) Cancer Epidemiol Biomarkers Prev, 17: 1723. (428)Fortner RT, et al. (2019) Breast Cancer Res, 21: 40. (429)Masi AC, et al. (2024) Microb Biotechnol, 17: e14520. . Longer durations of breastfeeding are associated with even greater reductions in risk (425)Jung AY, et al. (2022) J Natl Cancer Inst, 114: 1706. (427)Lord SJ, et al. (2008) Cancer Epidemiol Biomarkers Prev, 17: 1723. (430)Anstey EH, et al. (2017) Am J Prev Med, 53: S40. (431)Palmer JR, et al. (2014) J Natl Cancer Inst, 106. (432)World Cancer Research Fund. Research and Policy. Accessed: March 31, 2026. . For example, breastfeeding for 1 to 3 months has been associated with an 18 percent reduction in ovarian cancer risk, while breastfeeding for more than a year was linked to a 34 percent reduction (433)Babic A, et al. (2020) JAMA Oncol, 6: e200421. .
Importantly, the benefits of breastfeeding also extend to aggressive tumor subtypes. Women who have given birth but never breastfed were 2.18 times more likely than women who have never given birth to be diagnosed with triple-negative breast cancer. However, breastfeeding appears to mitigate this increased risk, with longer durations providing greater protection against both ER-negative and triple-negative breast cancers (430)Anstey EH, et al. (2017) Am J Prev Med, 53: S40. .
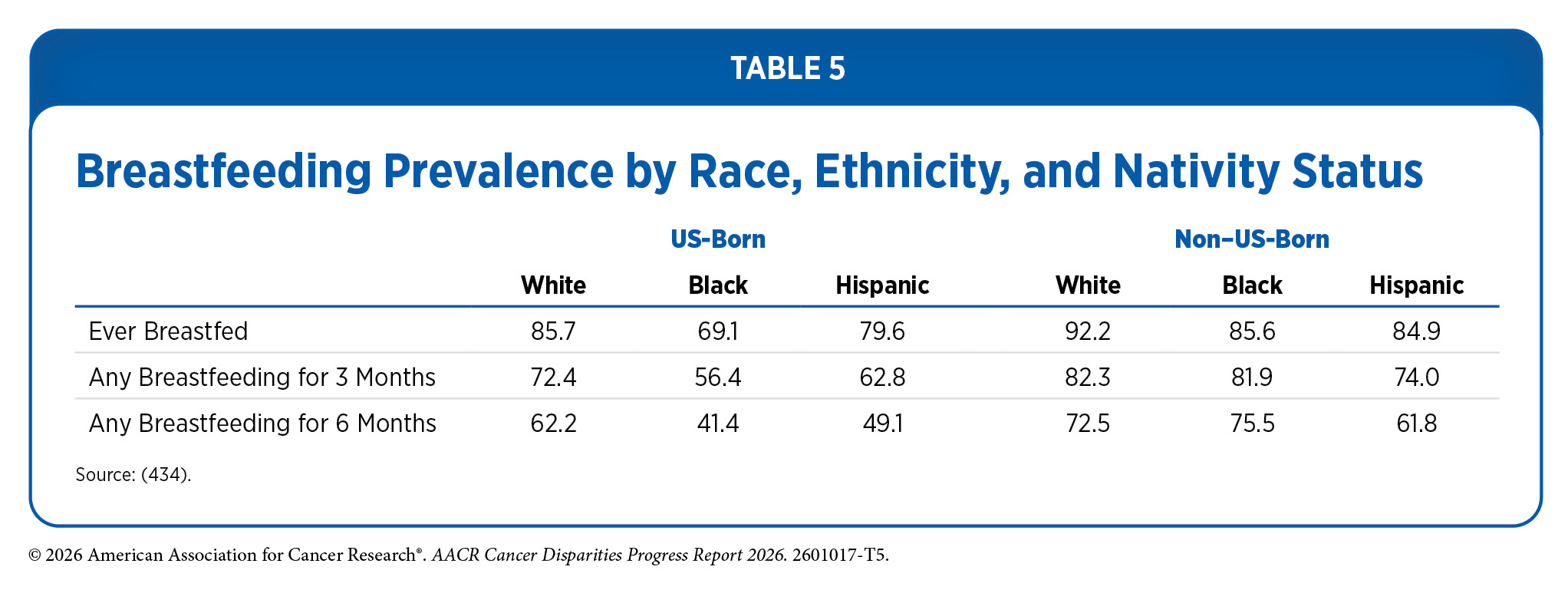
These findings show particular relevance for populations facing a disproportionate burden of these aggressive cancers. Young women and Black women experience higher rates of triple-negative and ER-negative breast cancers (see Understanding Cancer Development in the Context of Cancer Disparities and Understanding and Addressing Drivers of Cancer Disparities). Compounding this disparity, US-born Black and Hispanic women are less likely to breastfeed than White women (see Table 5) (434)Campbell AG, et al. (2024) Breastfeeding Medicine, 19: 870. .
Hormone Replacement Therapy
Hormone replacement therapy (HRT) refers to treatments used to alleviate symptoms of menopause and address long-term biological changes, such as bone density loss, that occur with age-related declines in estrogen and progesterone levels. HRT typically involves either estrogen alone or a combination of estrogen and progestin. Estrogen only therapy is used for individuals who have undergone a hysterectomy; for those who have not, progestin is added because estrogen alone increases the risk of endometrial cancer, a type of cancer that forms in the tissue lining of the uterus.
Data show that women who use the estrogen and progestin combination have an increased risk of developing breast cancer (435)Chlebowski RT, et al. (2020) JAMA, 324: 369. (436)Chlebowski RT, et al. (2008) Arch Intern Med, 168: 370. . The risk is greater with longer duration of use and is nearly two-fold higher among women who have used estrogen and progestin in combination for 10 years or longer, compared to those who never used HRT (437)Chlebowski RT, et al. (2009) N Engl J Med, 360: 573. (438)Collaborative Group on Hormonal Factors in Breast Cancer (2019) Lancet, 394: 1159. (439)Wang SM, et al. (2020) Breast Cancer Res, 22: 129. . Women who are no longer using HRT have a lower risk than current users, but an elevated risk may persist for more than a decade after they have stopped taking the drugs (438)Collaborative Group on Hormonal Factors in Breast Cancer (2019) Lancet, 394: 1159. . Individuals who seek HRT should discuss with their health care providers the advantages and possible risks before deciding what is right for them.
Women from racial and ethnic minority groups report vasomotor symptoms—hot flashes and night sweats—associated with menopause at higher rates than White women, yet they are less likely to seek or receive HRT (440)Green R, et al. (2010) Climacteric, 13: 376. (441)Gold EB, et al. (2006) Am J Public Health, 96: 1226. (442)Blanken A, et al. (2022) Menopause, 29: 877. (443)Zahn K, et al. (2024) Maturitas, 186: 108021. . Insurance status also contributes to disparities in the receipt of HRT. Women with Medicaid or Medicare receive systemic estrogen at nearly half the rate of women with private insurance (444)Rodriguez MI, et al. (2024) Menopause, 31: 1062. . While lower uptake of HRT among women from racial and ethnic minority groups represents a disparity in symptom management and quality of life, it may also confer a relative advantage with respect to HRT-related cancer risk. Because systemic HRT is associated with an increased risk of breast cancer, higher utilization among White women may contribute to greater cancer risk in this group, whereas disparities in HRT use primarily reflect inequities in menopause care rather than elevated cancer risk among minority women.
An emerging area of research within hormone therapy involves understanding cancer risks associated with gender-affirming hormone therapy (GAHT) (445)Jackson SS, et al. (2022) Trends Cancer, 8: 273. . Although current data remain limited, evidence suggests that transgender women receiving GAHT may have an increased risk of breast cancer, but a decreased risk of prostate cancer compared to age-matched cisgender men (446)de Blok CJM, et al. (2019) BMJ, 365: l1652. . In contrast, transgender men who received testosterone for at least 5 years show no increased risk of endometrial, ovarian, vaginal, or vulvar cancers (447)Vestering A, et al. (2025) EClinicalMedicine, 80: 103037. . Long-term follow-up studies are needed to fully understand these risks, but current evidence provides important preliminary guidance for SGM individuals considering GAHT (447)Vestering A, et al. (2025) EClinicalMedicine, 80: 103037. .
Social and Behavioral Stress
Psychosocial risk factors, which include depression, anxiety, and stress, have been associated with cancer risk (448)McGee R, et al. (1994) Social Science & Medicine, 38: 187. (449)Oerlemans ME, et al. (2007) Clin Pract Epidemiol Ment Health, 3: 29. and outcomes (450)Chida Y, et al. (2008) Nat Clin Pract Oncol, 5: 466. with mixed findings. However, when examined independently, stress—whether chronic or acute—has been more consistently associated with increased cancer risk (451)Dalton SO, et al. (2002) Eur J Cancer, 38: 1313. . Despite this evidence, the precise role of stress remains difficult to determine due to challenges in measuring stress exposure and distinguishing its effects from co-occurring factors. Stress may also indirectly elevate cancer risk by promoting unhealthy coping behaviors such as smoking, alcohol use, physical inactivity, and unhealthy diet, all of which are established cancer risk factors.
Growing evidence shows that stress can act not only as a trigger for risk enhancing behaviors but also directly on the body by promoting chronic inflammation, disrupting hormonal regulation, and weakening immune function, all of which can contribute to cancer development and worse outcomes (452)Antoni MH, et al. (2023) Annu Rev Psychol, 74: 423. (453)Mohan A, et al. (2022) Eur J Cancer Prev, 31: 585. . SDOH, such as financial strain, social isolation, and negative life events, can further exacerbate physiological stress responses, including elevated cortisol levels, particularly among populations who are disproportionately exposed to these stressors (454)Vignjevic Petrinovic S, et al. (2023) Front Physiol, 14: 1119095. . For example, recent evidence indicates that Black women diagnosed with breast cancer who reported greater exposure to SDOH-related stressors had higher cortisol levels than those with lower exposure (155)Sanogo F, et al. (2026) Cancer Res Commun, 6: 698. . Elevated cortisol activity is associated with tumor progression, metastasis, and reduced treatment efficacy, which contribute to racial disparities in cancer outcomes. As a result, stress is increasingly recognized as an independent factor influencing cancer initiation and progression (see Sidebar 18).
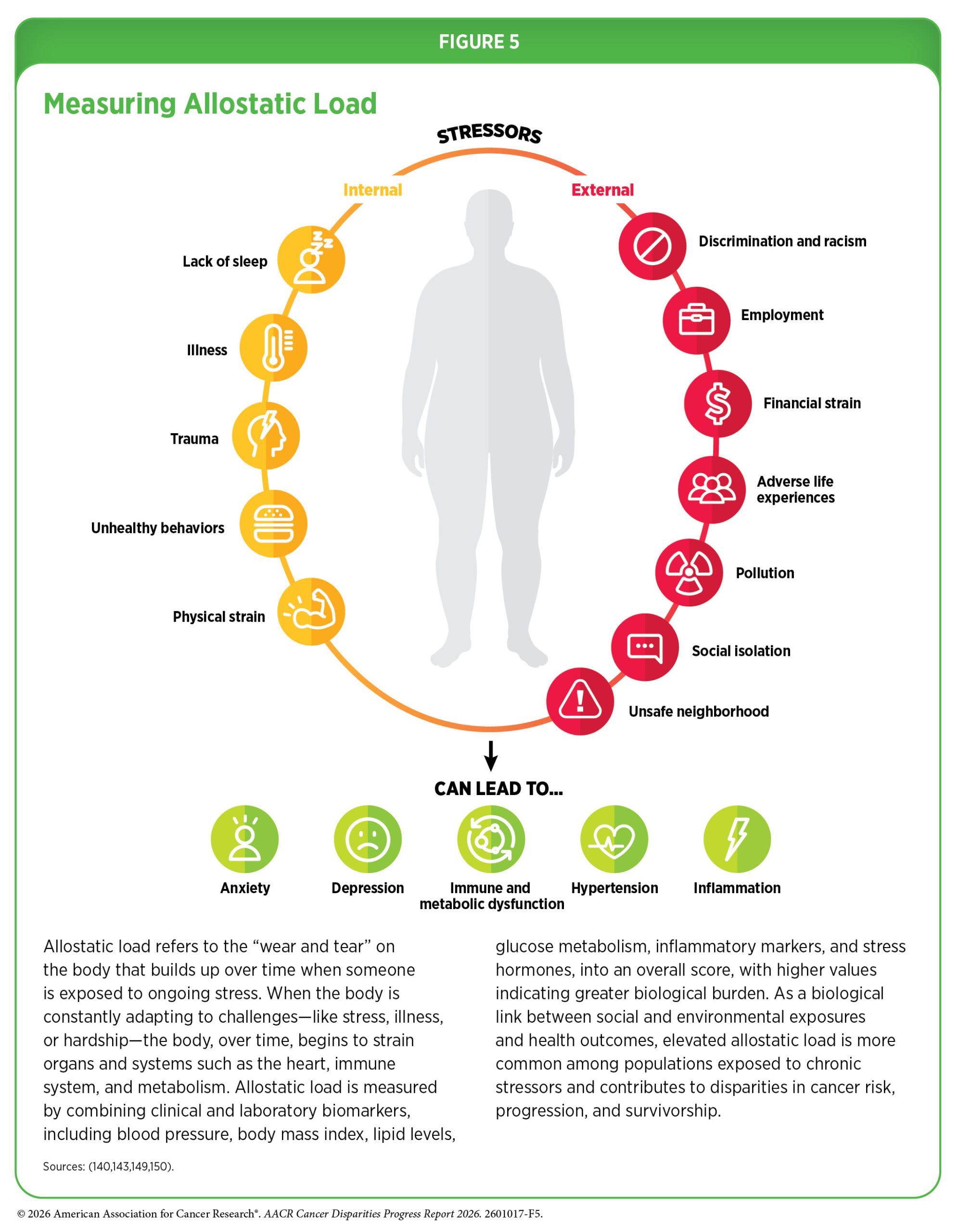
An expanding area of research in cancer disparities focuses on allostatic load—the cumulative physiologic burden of chronic stressors, lifestyle factors, and environmental exposures over the life course (see Figure 5) (460)Obeng-Gyasi S, et al. (2023) JAMA Network Open, 6: e2313989. (461)Guan Y, et al. (2023) Breast Cancer Res, 25: 155. (462)Obeng-Gyasi S, et al. (2022) JAMA Network Open, 5: e2221626. (463)Parker HW, et al. (2022) Am J Prev Med, 63: 131. . Heightened allostatic load, particularly when driven by adverse SDOH, has been linked to worse cancer outcomes among racial and ethnic minority populations and other medically underserved communities (142)Guan Y, et al. (2025) JAMA Network Open, 8: e2528019. (464)Li C, et al. (2023) BMC Women’s Health, 23: 448. (465)Ishibe N, et al. (2025) American Journal of Epidemiology, 194: 1485. . In one recent study of women with stage I to III breast cancer, each one unit increase in allostatic load was associated with a 3.33-fold higher risk of death among rural Black women (142)Guan Y, et al. (2025) JAMA Network Open, 8: e2528019. . These findings underscore the importance of addressing chronic stress as a biologically meaningful pathway through which structural inequities shape cancer outcomes. Researchers are actively evaluating interventions, including lifestyle modifications, stress reduction programs, and community-based support, that may help reduce allostatic load in populations at elevated risk for cancer.
Next Section: Disparities in Cancer Screening for Early Detection Previous Section: Understanding Cancer Development in the Context of Cancer Disparities