- Importance of Routine Cancer Screening
- Recommendations for Cancer Screening
- Disparities in Cancer Screening
- Breast Cancer Screening
- Cervical Cancer Screening
- Colorectal Cancer Screening
- Lung Cancer Screening
- Prostate Cancer Screening
- Disparities in Access to High-risk and Hereditary Cancer Surveillance
- Eliminating Disparities in Cancer Screening Through Evidence-based Interventions
Disparities in Cancer Screening for Early Detection
In this section, you will learn:
- Cancer screening for early detection means checking for precancerous lesions or cancer in people who are at an average or increased risk of developing cancer but do not have symptoms of the disease.
- Consistent uptake of recommended screening, along with timely diagnostic follow-up, is associated with meaningful reductions in cancer morbidity and mortality.
- Persistent gaps in screening uptake and follow-up care disproportionately affect racial and ethnic minority populations and other medically underserved communities.
- Disparities in screening arise from a complex interplay of structural, socioeconomic, health system, and policy-related factors.
- A growing body of evidence shows that targeted, evidence-based strategies can improve adherence to recommended screening and follow-up, thereby narrowing long-standing disparities.
Contents
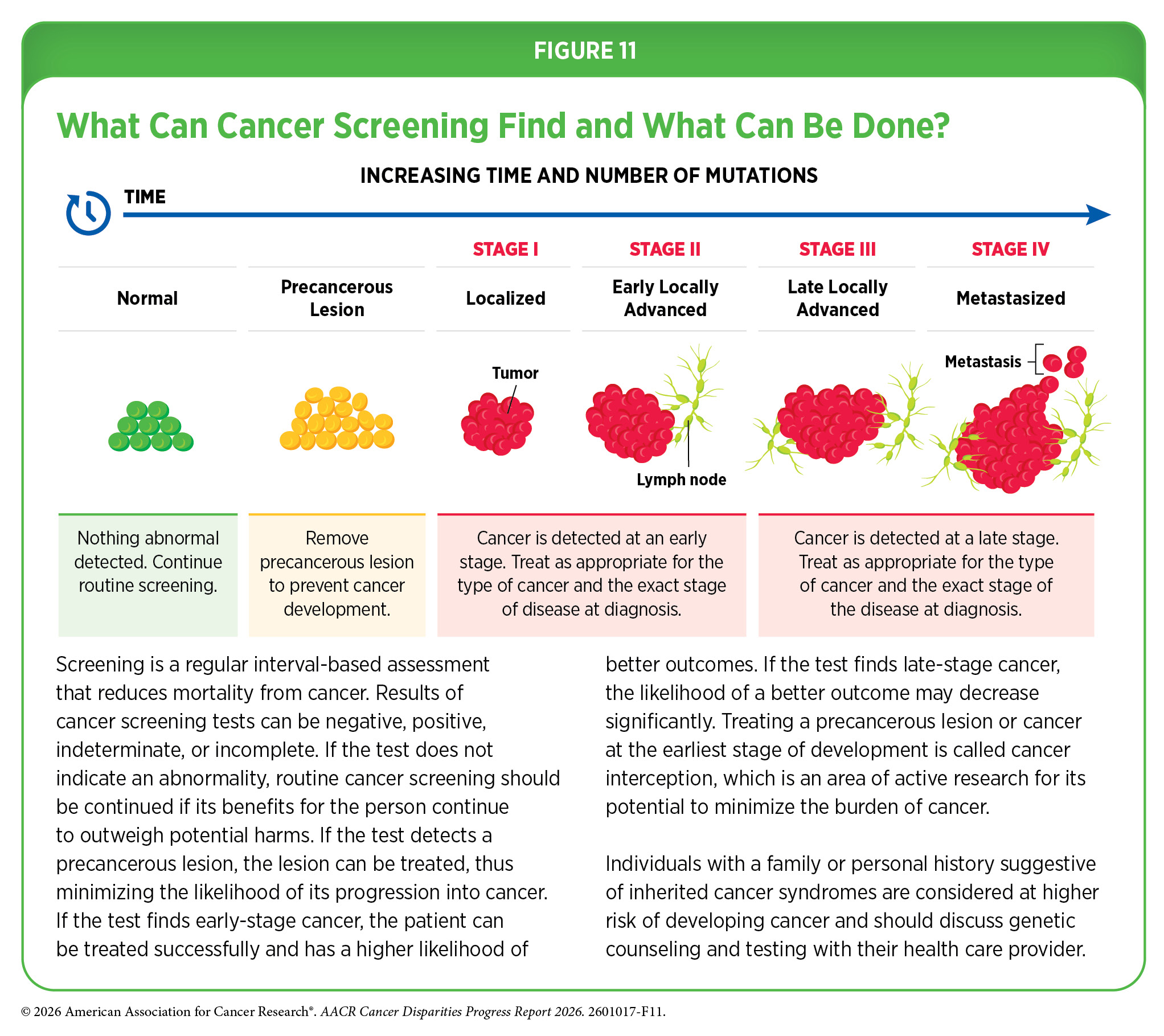
Screening means testing for cancer or abnormal cells that may become cancerous in individuals without any signs or symptoms of the disease. Routine screening is a regular assessment for early detection of cancer and is one of the most powerful public health strategies that reduces mortality and morbidity from cancer. Detection of precancerous lesions and cancers at the earliest possible stage significantly increases the likelihood that the treatment will be successful and markedly reduces the chances that the disease will progress to an advanced stage and spread to other parts of the body (see Figure 11).
Importance of Routine Cancer Screening
Routine cancer screening plays an essential role in reducing the overall burden of cancer by identifying precancerous changes or detecting cancers at an early stage, when treatment is more effective and the likelihood of favorable outcomes is greater.
A comprehensive analysis of breast, cervical, colorectal, lung, and prostate cancers diagnosed between 1975 and 2020 estimated that screening and prevention together accounted for 4.75 million of the 5.94 million cancer deaths averted in the United States (US) (313)Goddard KAB, et al. (2025) JAMA Oncol, 11: 162. . The contribution of screening varied by cancer type. For cervical cancer, all mortality reduction was due to screening and treatment of precancerous lesions. For colorectal cancer (CRC), 79 percent of deaths averted resulted from screening and removal of precancerous polyps. Screening accounted for 56 percent of deaths prevented from prostate cancer and 25 percent from breast cancer, while most of the decline in lung cancer deaths was driven by prevention, particularly reduced tobacco use (see Commercial Tobacco Use) (313)Goddard KAB, et al. (2025) JAMA Oncol, 11: 162. .
Routine cancer screening may reduce late-stage diagnosis and the need for more intensive treatment. In a study of more than 13,000 patients ages 70 to 79, those who had at least one mammogram in the 5 years before diagnosis were 54 percent less likely to be diagnosed with late-stage breast cancer and 36 percent less likely to die from it than those who were not screened. Women who had three to four screenings were 37 percent less likely to die than those who had only one screening (467)Huang S, et al. (2025) JAMA Netw Open, 8: e255322. . Further, early detection through screening can reduce the economic burden of cancer by enabling less complex and less costly treatment. In 2021, the United States spent about $43 billion on cancer screening, compared to $52.56 billion for just the first 12 months of cancer treatment (468)Halpern MT, et al. (2024) Ann Intern Med, 177: 1170. .
Recommendations for Cancer Screening
Cancer screening recommendations are developed through structured, evidence-based processes led by expert panels convened by government and public health organizations. This report focuses on guidance from the US Preventive Services Task Force (USPSTF), an independent panel supported by the Agency for Healthcare Research and Quality, which develops primary care recommendations through comprehensive evidence review and public input. Other organizations also issue screening guidelines, using similar rigorous approaches to maximize benefits and minimize harms.
Although screening recommendations are carefully developed using the best available evidence, their effectiveness ultimately depends on whether individuals can access and complete recommended screening. For example, a recent analysis of the impact of the 2021 USPSTF lung cancer screening update found that screening uptake increased by 46 percent. However, those without health insurance were 70 percent less likely, and those without a regular doctor were 52 percent less likely, to be up to date with lung cancer screening than their counterparts (469)Rolle LD, et al. (2025) JAMA Oncol, 11: 784. .
Eligibility Criteria for Cancer Screening
A person’s risk of developing cancer determines eligibility for routine screening. Individuals at average risk, with no personal or family history or known inherited/predisposing condition, are typically screened based on age and sex assigned at birth. Those at higher risk, including individuals with certain exposures, prior cancer, family history, hereditary cancer syndromes, or certain tissue architecture (e.g., women with dense breasts) may require different screening approaches, often including genetic counseling and testing.
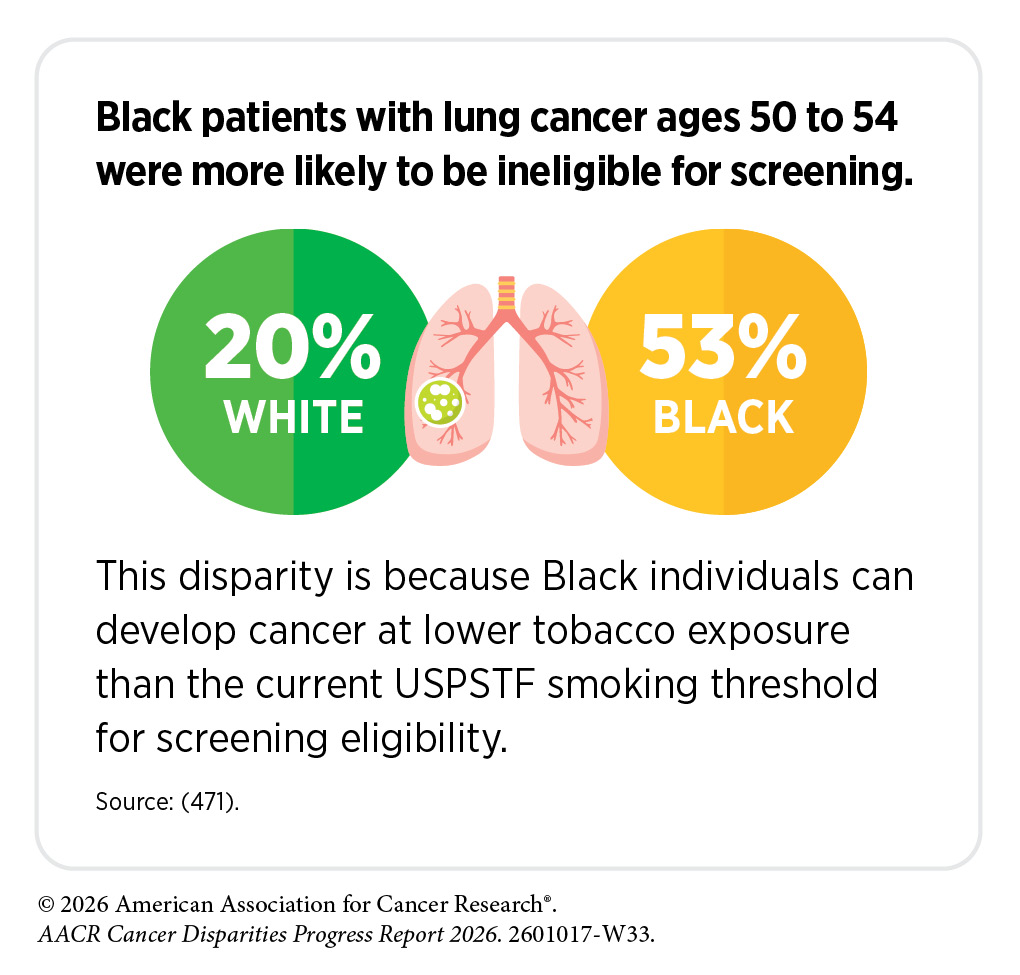
Screening eligibility criteria can contribute to disparities, because exposure to risk factors (see Disparities in the Burden of Modifiable Behavioral Cancer Risk Factors), the risk associated with a given level of exposure, and access to risk assessment vary across populations. For example, lung cancer screening eligibility is partly based on smoking history, for which many Black individuals do not often qualify. This is a particular concern because Black individuals develop lung cancer at lower levels of tobacco exposure than White individuals (470)Potter AL, et al. (2024) J Clin Oncol, 42: 2026. , meaning current smoking-based eligibility thresholds may systematically exclude a population that carries a disproportionately higher lung cancer burden.
A large study evaluated the revised lung cancer screening guidelines issued by USPSTF and a cancer-focused professional organization. Researchers found that removing the requirement for time since smoking cessation increased eligibility overall but widened disparities in lung cancer screening among Black and Hispanic individuals by 12 and 22 percentage points, respectively, compared to White individuals (472)Manful A, et al. (2026) Chest. . The study also found increased disparity between these populations with the revised USPSTF lung cancer screening guidelines, albeit to a lesser extent. These findings emphasize how eligibility criteria designed around population averages can inadvertently exacerbate disparities in routine cancer screening.
Because risk factors differ across populations and change over time, screening recommendations are periodically updated as new evidence comes to light. Ongoing discussions between patients and providers are important to ensure screening decisions reflect evolving evidence, individual risk, and preferences. It is important to note that USPSTF has not met since March 2025. As a result, recommendations under revision, notably those for cervical and prostate cancer screening, have not been updated since at least December 2024, delays that may have far reaching ramifications for the burden of these cancers at the population level (see Policies to Address Disparities in Cancer Screening and Follow-up Care).
Guidelines for Cancer Screening
USPSTF develops screening recommendations by evaluating whether the benefits of screening outweigh the potential harms. In some cases, USPSTF recommends against screening if available evidence suggests that harms may exceed benefits. In other situations, the panel may issue an “I statement,” indicating that the evidence is insufficient to determine the balance of benefits and harms.
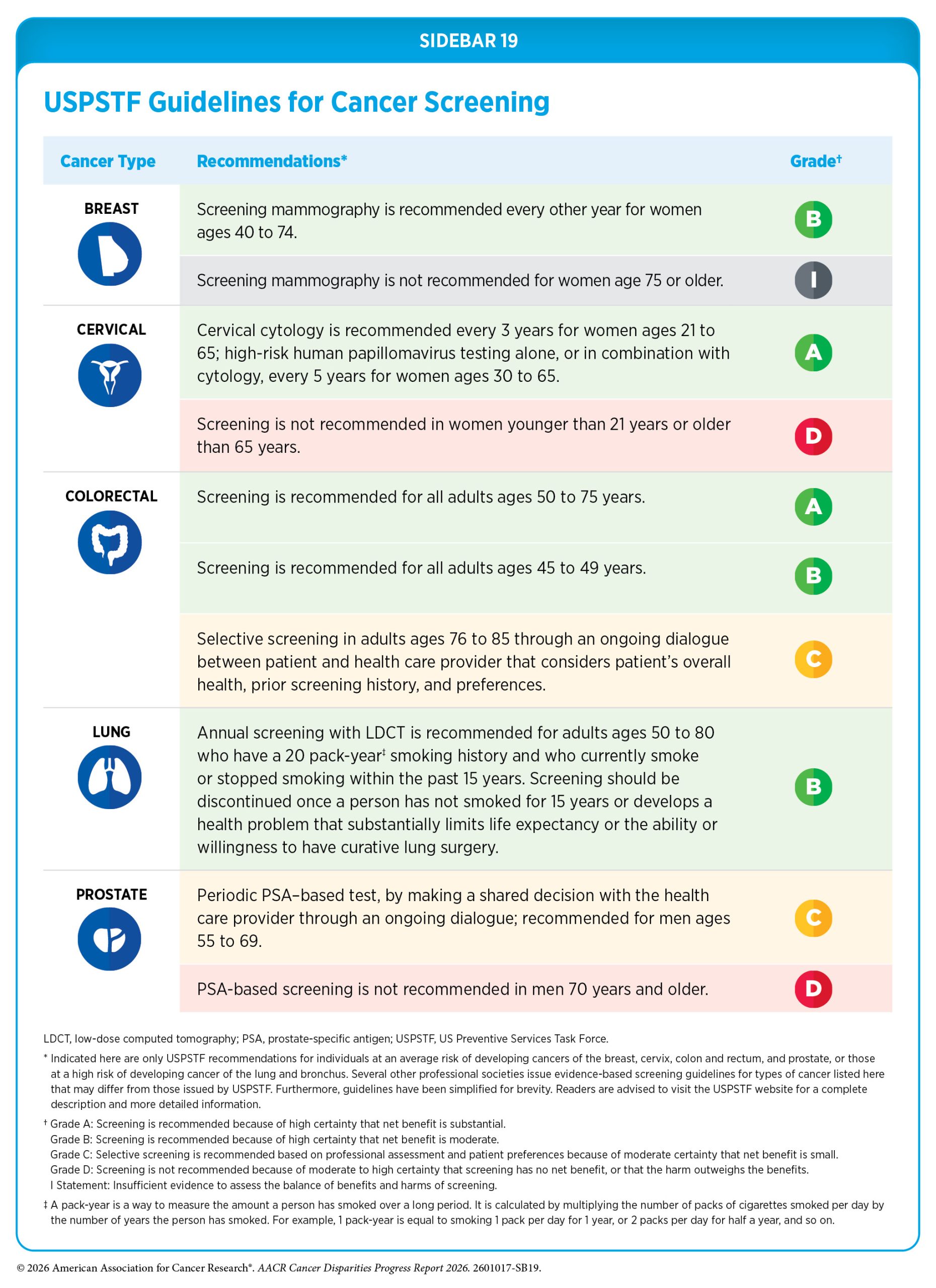
Each recommendation is assigned a letter grade reflecting the strength of the supporting evidence (see Sidebar 19). These grades also influence whether a screening test is covered without out-of-pocket costs under the Patient Protection and Affordable Care Act. In some instances, different population groups may receive different screening recommendation grades for the same cancer type based on available evidence. Final recommendations and supporting evidence reviews are published in peer-reviewed journals and on the USPSTF website.
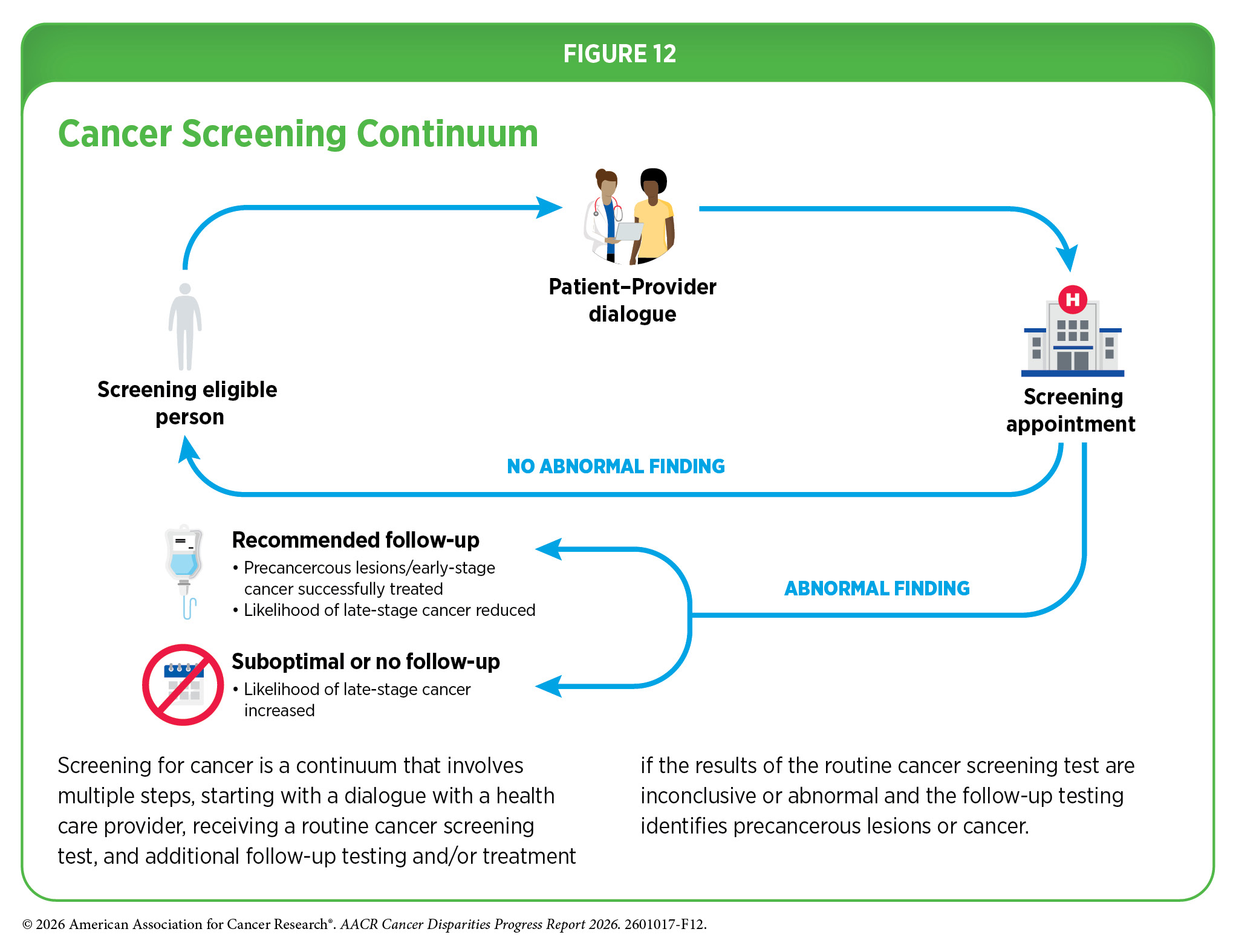
Cancer screening is not a single event but a process that involves several steps (see Figure 12). It typically begins with a discussion between individuals and their health care provider about the potential benefits and risks of screening based on personal factors such as age, family history, cancer risk behaviors, and overall health. If a screening test does not reveal a concerning finding, individuals return for screening after the recommended interval. However, if the test identifies possible abnormalities or produces unclear results, follow-up care may be needed. This may include additional diagnostic testing to confirm whether cancer is present and, if necessary, initiation of treatment. Each step in this continuum—from initial consultation to follow-up testing—represents a point at which barriers to care can affect whether individuals complete recommended screening and receive timely diagnosis.
Tests for Cancer Screening
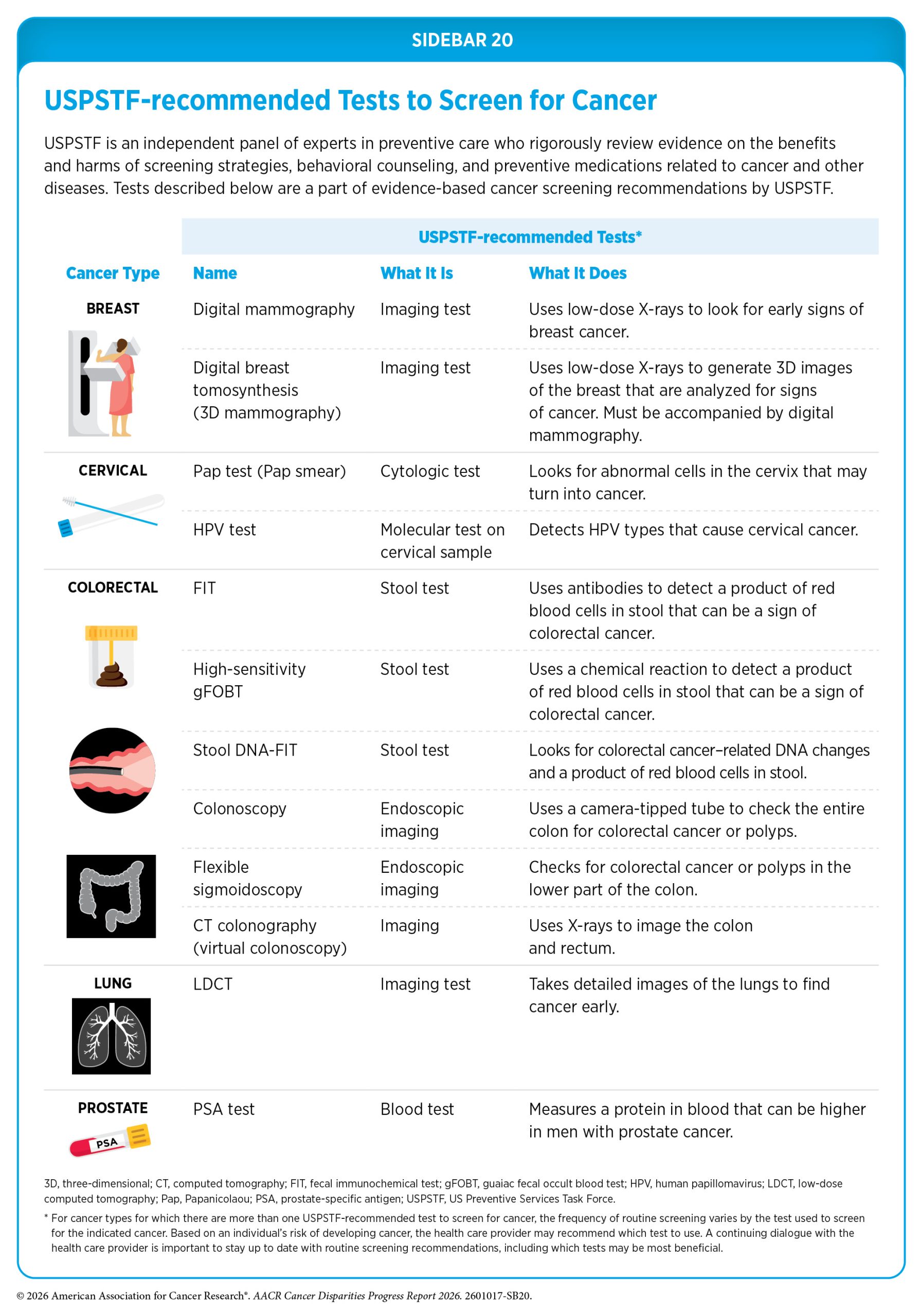
Cancer screening tests include laboratory procedures that detect cellular or molecular signals of cancer in blood or other biospecimens, as well as imaging or endoscopic procedures that identify tissue changes suggestive of cancer. USPSTF carefully weighs the potential benefits of these tests against any risks associated with screening to ensure that recommendations provide a net benefit to public health (see Sidebar 20).
Like all medical procedures, screening tests have limitations. As one example, although rare, complications from procedures such as colonoscopy can occur (473)Lv XH, et al. (2025) Am J Gastroenterol. . Furthermore, tests may yield false-positive results that lead to unnecessary follow-up or false-negative results that delay diagnosis. Screening can also detect slow-growing cancers that may never cause symptoms, leading to interventions with limited benefit. Researchers continue to refine screening methods to improve accuracy and reduce harm.
Even when recommendations are evidence-based, their benefits depend on access to screening, timely follow-up, and the ability to navigate the health care system. Differences in access, awareness, insurance coverage, and health system resources can limit screening uptake, contributing to persistent disparities in cancer detection and outcomes (see Understanding and Addressing Drivers of Cancer Disparities).
Disparities in Cancer Screening
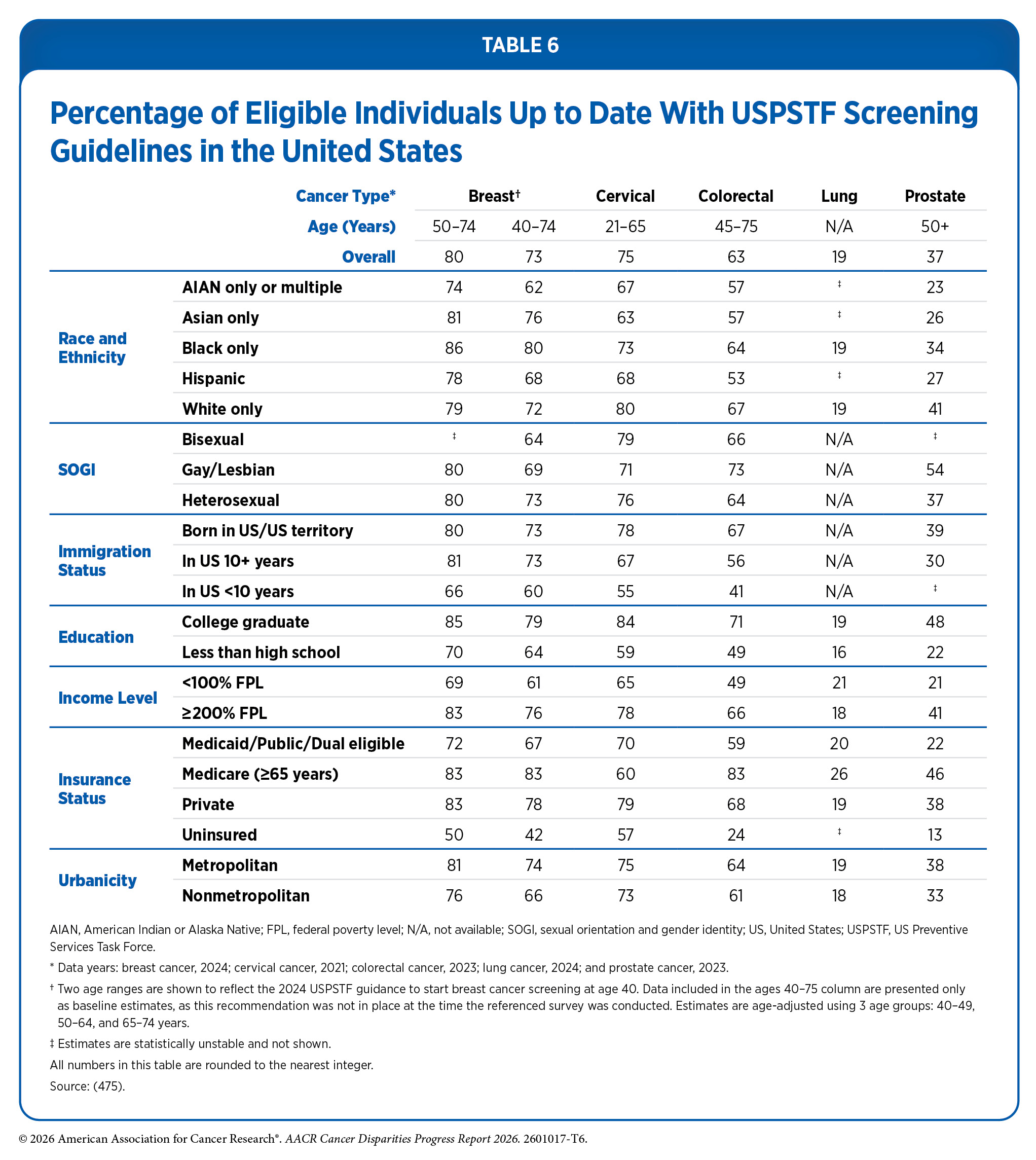
Following recommended cancer screening is one of the most effective ways to reduce cancer burden at the population level, yet adherence remains suboptimal. Screening patterns vary across cancer types and are lower among racial and ethnic minority groups, citizens of sovereign Native Nations, and other medically underserved populations. Lung cancer screening shows the lowest overall uptake at 19 percent, and disparities in routine screening across cancer types are most pronounced by insurance status, with uninsured individuals less likely to be screened than those with private insurance, and by immigration status, with recently arrived immigrants showing the lowest rates across all cancers examined (see Table 6). Population-level disruptions such as the COVID-19 pandemic can further exacerbate existing disparities in screening uptake. As one example, compared to 2019, routine cancer screening rates among eligible adults declined in 2021, with decreases of 12 percent for colorectal screening, 14 percent for cervical and prostate screening, and 7 percent for breast screening. Asian adults experienced the largest overall decreases, while Black adults were about 22 percent less likely to receive colorectal screening and Hispanic adults were about 17 percent less likely to receive breast cancer screening (474)Alba C, et al. (2024) JAMA Health Forum, 5: e235058. .
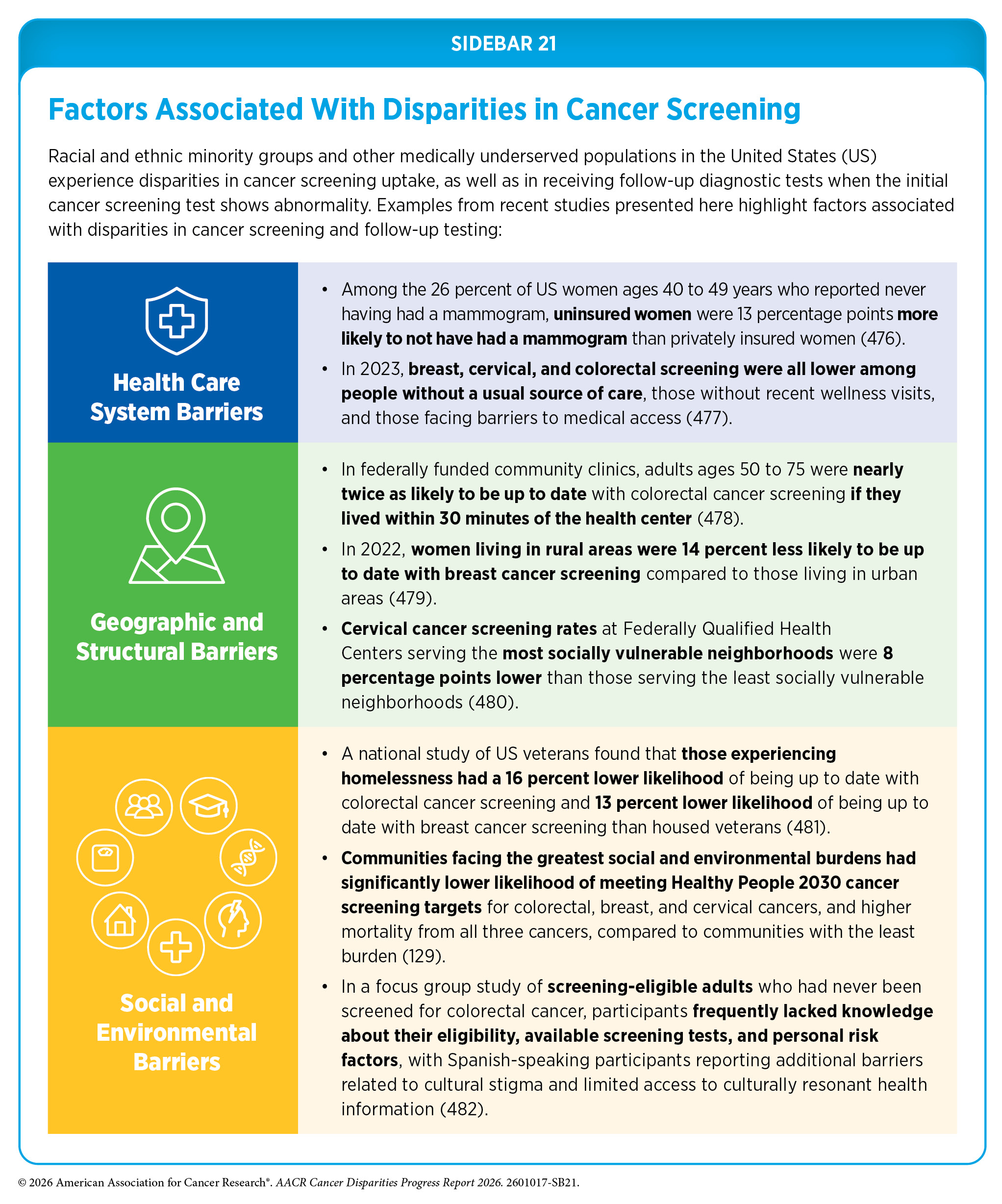
Gaps in cancer screening are driven by multiple barriers, including structural and social factors, lack of awareness about recommendations, bias and discrimination in the health care system, and limited access to quality insurance and care (see Sidebar 21). This report examines disparities in screening for breast, cervical, colorectal, lung, and prostate cancers, and highlights evidence-based interventions to reduce them.
Breast Cancer Screening
Breast cancer is the most diagnosed cancer among women in the United States. There are stark disparities in the incidence, mortality, and survival of breast cancer between White women and those from racial and ethnic minority populations and other medically underserved populations (see The State of US Cancer Disparities in 2026). Disparities in the breast cancer burden may arise from differences in access to and uptake of routine screening (see Table 6), the follow-up diagnostic testing if the initial screening test indicates an abnormality, and whether screening is used appropriately.
Only 59 percent of US women ages 40 to 49 reported biennial mammography, while 15 percent were overdue and 26 percent had never been screened (476)Gu T, et al. (2024) JAMA Netw Open, 7: e2451827. . Screening rates were significantly lower among women of other races (i.e., American Indian or Alaska Native, alone or in combination with another race, and other unspecified groups), lesbian and bisexual women, rural residents, and those with incomes at or below 138 percent of the federal poverty level. Lack of a usual source of health care was strongly associated with both overdue and no screening, highlighting the role of access, coverage, and affordability in driving disparities (476)Gu T, et al. (2024) JAMA Netw Open, 7: e2451827. . A recent study found that while Black women were somewhat more likely to be screened than White women, they were also more likely to receive screening outside the recommended age when the potential benefit of routine screening is limited. These findings indicate that disparities can involve both too little and too much screening (483)Lui ML, et al. (2026) Cancer Epidemiol Biomarkers Prev, 35: 456. .
Safety-net hospitals, often the primary point of care for underserved populations, show some of the starkest gaps in screening, and those gaps translate directly into later-stage cancer diagnosis. In one large safety-net system, compared to 13 percent of White women, 46 percent of Hispanic women and 37 percent of Black women had never been screened. The proportion of women diagnosed at advanced stage varied significantly by screening history, with 20 percent of never-screened patients diagnosed at stage IV compared to 8 percent of ever-screened and 3 percent of recently screened patients (484)Su M, et al. (2025) Am J Prev Med, 69: 108014. . These findings show how gaps in routine screening lead to late-stage diagnosis, which has its own adverse downstream effects, such as worse health outcomes and higher care costs.
Breast cancer screening disparities extend beyond the initial mammogram. A recent study on diagnostic testing after abnormal screening mammography found disparities in use of same-day advanced diagnostic services and biopsy (485)Lawson MB, et al. (2025) Radiology, 314: e241673. . Compared to White patients, Asian patients were 26 percent less likely, Black patients 44 percent less likely, and Hispanic patients 39 percent less likely to receive same-day follow-up tests after an abnormal mammogram. Furthermore, after an abnormal finding from the follow-up diagnostic testing, Black patients were 54 percent less likely than White patients to receive a same-day biopsy (485)Lawson MB, et al. (2025) Radiology, 314: e241673. .
There are also substantial disparities in routine cancer screening among SGM communities (see Table 6). A combined analysis of two national surveys indicates that bisexual or queer women face greater health care access barriers, including inconsistent access to care and more difficulty affording care, and these disadvantages are associated with lower mammography adherence. For example, compared to straight women, lesbian, gay, bisexual, or queer women overall were more likely to be uninsured and report financial barriers to care. Bisexual and queer women were about 9 percent less likely to be up to date with mammography screening, and these patterns appeared more pronounced for bisexual or queer women than for lesbian women (487)Zhang H, et al. (2025) Cancer, 131: e35852. .
Cervical Cancer Screening
A recent analysis showed that 100 percent of 160,000 deaths from cervical cancer averted between 1975 and 2020 were because of routine screening (313)Goddard KAB, et al. (2025) JAMA Oncol, 11: 162. . Conversely, studies have consistently shown that persistent screening gaps translate into worse health outcomes. In a national analysis of more than 1,000 US counties, counties with repeatedly low cervical cancer screening coverage had 83 percent higher cervical cancer incidence and 96 percent higher mortality compared to counties with high screening coverage (488)Amboree TL, et al. (2025) JAMA Netw Open, 8: e2526709. .
Yet there is overall suboptimal uptake of cervical cancer screening among eligible individuals, as well as uneven screening uptake across several population groups (see Table 6). A nationwide study found that only 75 percent of screening-eligible women were up to date in 2023 (477)Sabatino SA, et al. (2025) Prev Chronic Dis, 22: E52. . Cervical cancer screening uptake was consistently lower in Asian and Hispanic women compared to White women. Furthermore, women with lower educational attainment, those who were uninsured or underinsured and those who experienced hardships, such as lack of transportation, food insecurity, housing and utility strain, and medical financial hardship, had lower cervical cancer screening uptake (see Table 6) (477)Sabatino SA, et al. (2025) Prev Chronic Dis, 22: E52. .
Residential segregation and other structure-level drivers of health (see Understanding and Addressing Drivers of Cancer Disparities) significantly influence screening uptake. As one example, a study of five US health systems found that higher levels of racial residential segregation were associated with lower overall uptake of cervical cancer screening among Black patients compared to White patients (489)Issaka RB, et al. (2024) Cancer, 130: 4287. . Within this pattern, however, neighborhood composition influenced screening uptake: Black patients living in neighborhoods with more Black residents were 46 percent more likely to receive screening than Black patients living in neighborhoods with fewer Black residents, suggesting that shared cultural norms and informal social networks within those communities may partially offset structural barriers. Conversely, White patients living in neighborhoods with more Black residents were 12 percent less likely to receive screening (489)Issaka RB, et al. (2024) Cancer, 130: 4287. . Screening rates were also influenced by how easy or difficult it was for residents to access screening through the health system serving them, indicating that uptake reflects both neighborhood social context and the structural relationship between residents and health care systems.
Stark disparities in cervical cancer screening uptake also exist among other medically underserved populations, including people with physical or learning disabilities, immigrants and refugees, and sexual and gender minority (SGM) populations.
Data on cervical cancer screening in SGM populations remain limited, but available studies describe barriers including discrimination, discomfort with gendered clinical environments, low trust in health care systems, and lack of tailored guidelines (490)Mayer G, et al. (2025) Am Soc Clin Oncol Educ Book, 45: e473608. (491)LeBlanc ME, et al. (2025) Reprod Health, 22: 135. . Emerging evidence also highlights disparities among individuals with physical or learning disabilities. Only about half of women with physical disabilities were up to date with screening, with reported barriers including inaccessible exam settings, physical challenges during pelvic exams, and negative clinical interactions (492)Vinson AH, et al. (2025) JAMA Netw Open, 8: e2457290. . In a safety-net clinic, adults with learning disabilities were 56 percent less likely to be up to date with screening, compared to other adults who were admitted to the clinic (493)Schuering KM, et al. (2026) J Gen Intern Med. .
Disparities are also evident among immigrant and refugee populations (see Table 6). African immigrant women in the United States have lower screening uptake, with variation by country of origin, language, and duration of US residence (494)Suleman DB, et al. (2026) Palliat Support Care, 24: e68. . Among Black immigrant women, those with high social connectedness were nearly twice as likely to be screened, although private insurance remained a strong predictor of being up to date (495)Cofie LE, et al. (2026) J Racial Ethn Health Disparities, 13: 117. . Refugee populations face additional barriers, including language challenges, limited familiarity with preventive care, and competing socioeconomic priorities, all of which contribute to lower screening uptake (496)Nassur J, et al. (2025) J Immigr Minor Health, 27: 609. .
Barriers to cervical cancer screening among medically underserved populations are further compounded by the rapid evolution of screening guidelines, which has created knowledge gaps at both the patient and provider level. Studies have found that clinician awareness of updated guidelines is incomplete; few providers have adopted primary human papillomavirus (HPV) testing as recommended, and many fail to counsel patients about evolving screening options, compounding patient-level knowledge gaps (497)Brennan L, et al. (2024) J Clin Transl Sci, 8: e118. (498)Cannizzaro NT, et al. (2024) J Womens Health (Larchmt), 33: 1614. (499)Michel AD, et al. (2024) Cancer, 130: 2325. . Self-collected HPV testing, in which individuals collect their own cervical sample at home, may help address some of these barriers by reducing reliance on in-person clinical encounters. The recent US Food and Drug Administration (FDA) approval of self-collected HPV testing and its inclusion in updated Health Resources & Service Administration (HRSA) guidelines, which provide programmatic guidance for community health centers serving underserved populations, presents an opportunity to reduce these structural barriers, but realizing that potential will require targeted provider education and system-level support to ensure that all populations benefit from these medical innovations (500)Christine B, et al. (2026) JAMA, 335: 661. .
Colorectal Cancer Screening
Colorectal cancer (CRC) is rapidly emerging as a major public health concern because of the rising incidence and mortality rates among those younger than 50 years of age, underscoring the need to ensure that those eligible are up to date with routine screening and that there are no disparities in screening uptake among various population groups. Unfortunately, CRC screening uptake has remained uneven in recent years (see Table 6). In one analysis of 2021 National Health Interview Survey data, CRC screening rates among screening-eligible adults were 74 percent among White adults, 71 percent among Black adults, 62 percent among Hispanic adults, and 59.5 percent among Asian adults. Furthermore, Asian adults were 27 percent less likely to have received a colonoscopy compared to White adults (501)Wang YR (2025) Am J Manag Care, 31: e235. . The study showed that immigrant status, lack of insurance, and lower educational attainment explained many of these differences (501)Wang YR (2025) Am J Manag Care, 31: e235. .
CRC incidence is rising sharply among younger adults, even as rates decline among older populations (see The State of US Cancer Disparities in 2026). In response, USPSTF lowered the eligibility for CRC screening from age 50 to age 45 in 2021, adding millions of newly eligible individuals to the screening pool, yet uptake in this group has remained far below that of older adults (502)Siddique S, et al. (2024) JAMA Netw Open, 7: e2436358. . In 2023, only 37 percent of adults ages 45 to 49 years were up to date with screening, compared to 73 percent of those ages 50 to 75 years, and overall uptake across all eligible age groups reached just 67 percent (477)Sabatino SA, et al. (2025) Prev Chronic Dis, 22: E52. . Those who are screened are also not representative of all population groups; a majority of individuals up to date with CRC screening live in urban areas and have high socioeconomic status (SES) (477)Sabatino SA, et al. (2025) Prev Chronic Dis, 22: E52. (503)Star J, et al. (2024) J Natl Cancer Inst, 116: 613. . Expanding the eligible population without addressing the structural barriers that limit access may further exacerbate the existing disparities in CRC screening.
Ensuring equitable receipt of CRC screening can be further complicated by the rapid emergence of new noninvasive CRC tests, including next-generation stool DNA, stool RNA, and blood-based tests, several of which received approval from FDA in 2024 (504)Carethers JM, et al. (2026) Annu Rev Med, 77: 161. . Because FDA approval and inclusion in USPSTF recommendations are distinct processes—FDA approval establishes that a test is safe and effective for its intended use; USPSTF recommendation establishes that the net benefit of using that test in a defined population is sufficient to recommend it as a routine screening strategy and ensures reimbursement—coverage of these newer tests under preventive services mandate of the Patient Protection and Affordable Care Act is not yet guaranteed, raising concerns about equitable access across insurance types and income levels. In practice, this means that patients whose providers recommend these newer tests may face out-of-pocket costs, creating an access gap that will disproportionately affect uninsured and low-income individuals.
Other recent evidence likewise shows that CRC screening remains particularly low among medically underserved groups. As one example, an analysis of 10 studies reporting disparities in CRC screening between rural and urban populations found that rural residents were 19 percent less likely to report any type of screening at any time period (505)Sepassi A et al. Oncologist. 29:e431. .
Socioeconomic and geographic disadvantages continue to shape CRC screening uptake. In an analysis of more than 21.7 million privately insured adults ages 50 to 75 at average risk, screening recovery after the COVID-19 pandemic was uneven by sex, area-level SES, and metropolitan status. Individuals in low-SES areas had consistently lower screening rates than those in high-SES areas, and this gap widened by 4 percentage points after the pandemic began. Screening uptake was also higher in metropolitan than nonmetropolitan areas before and after the pandemic (506)Siddique S, et al. (2025) J Gen Intern Med, 40: 611. .
In Federally Qualified Health Centers, CRC screening rates were rising before the pandemic, then declined and remained below prepandemic levels. Screening rates were 8.5 percentage points higher in centers with consistent patient-centered medical home (PCMH) recognition—a model of primary care that focuses on comprehensive, team-based, and patient-centered care—and better hypertension management than in centers without PCMH recognition. These findings indicate that both care setting and health system structure influence screening uptake (507)Zaire PJ, et al. (2026) Health Serv Res, 61: 1. . Similarly, studies examining neighborhood-level structural factors have found that individuals living in communities with higher levels of residential racial segregation are less likely to receive CRC screening (489)Issaka RB, et al. (2024) Cancer, 130: 4287. .
Immigration-related factors also influence adherence to CRC screening recommendations. One study evaluating screening adherence among immigrants ages 50 through 75 found that only 48 percent were up to date with screening. Immigrants who had lived in the United States for at least 15 years had 63 percent higher likelihood of screening adherence compared to those with shorter duration of residence, highlighting the importance of acculturation, health system familiarity, and access to health care resources (508)Okitondo C, et al. (2025) J Cancer Policy, 43: 100516. .
Some of the most consequential disparities in CRC screening arise after an abnormal stool test. Recent studies show that fewer than half of patients complete follow-up colonoscopy within 6 months after an abnormal stool test, with rates around 48 percent overall, with only 37 percent of Black patients and 39 percent of patients with Medicaid coverage receiving timely follow-up in a large multisystem analysis (509)Ciemins EL, et al. (2024) JAMA Netw Open, 7: e242693. . Another study found that receipt of follow-up colonoscopy within 6 months of an abnormal stool test result was only 36 percent in safety-net settings (510)Avilez L, et al. (2026) J Gen Intern Med. .
Related studies further corroborate multilevel barriers to follow-up diagnostic testing after abnormal stool-based screening (510)Avilez L, et al. (2026) J Gen Intern Med. (511)Issaka RB, et al. (2024) Clin Gastroenterol Hepatol, 22: 1967. (512)Wang CP, et al. (2026) J Gen Intern Med. . Eliminating these barriers can significantly reduce the burden of CRC. In fact, researchers estimate that eliminating disparities between Black and White individuals in follow-up colonoscopy and adenoma detection could reduce CRC incidence by 15 percent and mortality by 19 percent, while increasing life-years gained from screening by 7 percent (513)Alagoz O, et al. (2024) J Natl Cancer Inst, 116: 1807. .
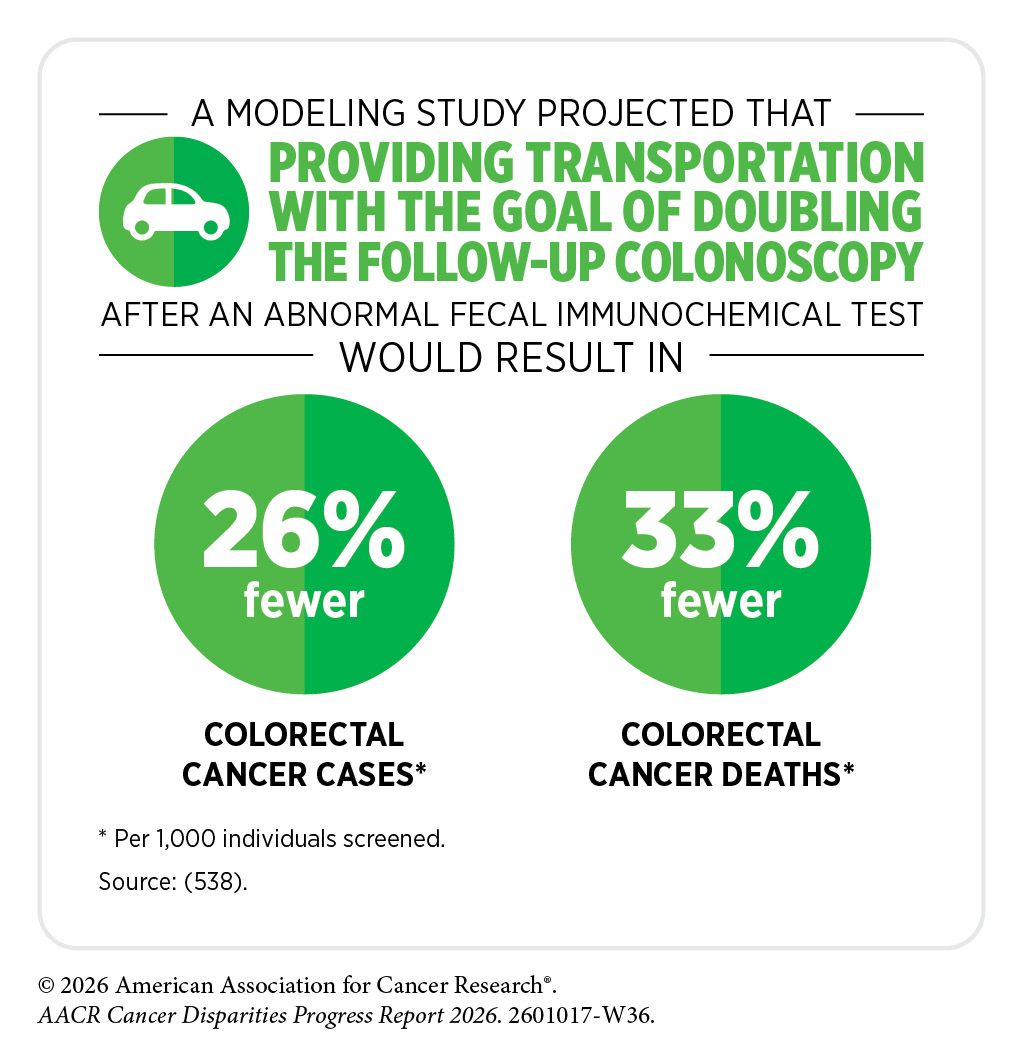
Taken together, these findings demonstrate that the transition from abnormal screening to follow-up diagnostic testing remains one of the most significant challenges in the CRC screening continuum, particularly for populations facing socioeconomic and health system barriers, and eliminating this disparity can significantly reduce the burden of CRC.
Lung Cancer Screening
Lung cancer screening has the lowest uptake overall, with just 19 percent of eligible individuals having received low-dose computed tomography (LDCT) in 2024 (see Table 6) (514)Bandi P, et al. (2025) JAMA, 334: 2225. . Researchers have projected that a 100 percent screening uptake would prevent 62,110 lung cancer deaths over 5 years, four times more than being averted at the current screening rate (514)Bandi P, et al. (2025) JAMA, 334: 2225. . In addition to low uptake, lung cancer screening disparities are numerous and arise from several intersecting barriers. Recent evidence shows that inequity begins with screening eligibility criteria, continues through whether screening is offered and accepted, and is exacerbated by geographic, linguistic, socioeconomic, and systemic barriers.
A recent study examined patients already diagnosed with lung cancer to evaluate whether they would have qualified for lung cancer screening under the updated 2021 USPSTF criteria—younger age and less intense smoking history. Researchers found that only 47 percent (ages 50 to 54) and 62 percent (ages 50 to 59) of Black patients would have qualified, compared to 80 percent and 89 percent of White patients in the corresponding age groups (471)Potter AL, et al. (2025) Cancer, 131: e35676. . For younger Black patients who were ineligible, the main reason was because they had smoked fewer than 20 pack-years, that is, packs of cigarettes smoked every year multiplied by the number of smoking years (471)Potter AL, et al. (2025) Cancer, 131: e35676. . It is important to note that Black individuals develop lung cancer at lower levels of tobacco exposure than White individuals (470)Potter AL, et al. (2024) J Clin Oncol, 42: 2026. . Smoking-based eligibility thresholds do not account for this difference, thus potentially excluding a population that already carries a disproportionate lung cancer burden.
A 2025 systematic review found overall lower screening eligibility among Black, Hispanic, and Asian populations compared to the White population, with estimated gaps ranging from 3 to 33 percentage points (515)Yambao Yang Y, et al. (2025) BMC Public Health, 25: 3978. . Emerging research shows that eligibility requirements tailored to race-specific risks may help reduce disparities in lung cancer screening (516)Manful A, et al. (2026) J Natl Cancer Inst, 118: 343. .
Even among those who participate in screening programs, adherence is unequal. In one centralized lung screening program, Asian participants were 58 percent less likely to stay up to date with annual lung cancer screening compared to other racial groups. Additionally, individuals with lower educational attainment were 26 percent less likely to adhere to annual screening (517)Tasevac B, et al. (2024) CHEST Pulmonary, 2: 100051. . Among Hispanic populations, barriers to lung cancer screening are shaped not only by ethnicity but also by nativity, language, and SES (518)Barrazueta SG, et al. (2026) J Racial Ethn Health Disparities, 13: 1527. . In a multistate study of community health centers, US-born Hispanic patients had similar likelihood of receiving a screening as White patients, while non–US-born Hispanic patients were 53 percent less likely and those without a recorded place of birth were 37 percent less likely to have screening ordered (519)Heintzman J, et al. (2025) J Am Board Fam Med, 38: 451. .
Geographic barriers are key contributors to low uptake of lung cancer screening in rural communities (see Table 6). A recent review of rural-urban disparities identified limited availability of accredited screening facilities, long travel distances, fewer outreach efforts, limited familiarity of clinicians with eligibility criteria, and higher uninsured rates as key contributing barriers (520)Gargapati A, et al. (2026) Cancers (Basel), 18. . Health insurance remains one of the most important determinants of up-to-date lung cancer screening, with one recent study showing that uninsured individuals were 67 percent less likely to have received lung cancer screening than those with private insurance (521)Gudina AT, et al. (2025) Cancer Epidemiol Biomarkers Prev, 34: 35. .
Health care system trustworthiness also plays a significant role in uptake of lung cancer screening. In a recent study of current smokers, Black participants reported higher levels of medical mistrust than White participants. In both groups, the willingness to get screened consistently decreased as mistrust increased. People with higher mistrust were noticeably less likely to view screening positively, felt less confident they could get screened, and were less likely to intend to get screened, even after receiving basic information about lung cancer and screening (522)Aspiras O, et al. (2025) Psychol Health Med, 30: 1057. . These findings underscore the need for health care systems to implement strategies that engender trustworthiness among all patients they serve.
Evidence on outcomes after participation in routine lung cancer screening further emphasizes why barriers to screening must be eliminated. In a study of Black and White patients with lung cancer who had participated in routine lung cancer screening, researchers found that Black patients were more than five times less likely to be diagnosed with advanced-stage lung cancer, while White patients were 3.5 percent less likely (523)Sabakhtarishvili G, et al. (2025) JTO Clin Res Rep, 6: 100899. . These findings indicate that removing barriers to lung cancer screening uptake can help reduce burden of the disease in all populations.
Prostate Cancer Screening
Disparities in the prostate cancer burden are apparent across the cancer continuum (see The State of US Cancer Disparities in 2026 and Disparities in Clinical Research and Cancer Treatment), including in screening across medically underserved populations (see Table 6). USPSTF currently recommends shared decision-making between the patient and the provider for initiating prostate cancer screening. Evidence is emerging that this recommendation introduces a barrier to uptake of prostate cancer screening.
A recent, population-based study found that among 9,723 men, only 24 percent reported discussing both the benefits and the harms of prostate-specific antigen (PSA) testing with a provider, while 63 percent had no discussion at all, with markedly lower engagement among men with less education (524)Bhojani N, et al. (2025) Prostate Cancer Prostatic Dis, 28: 400. . In a survey-based study, Black men described primary care clinicians as gatekeepers who often did not bring up PSA testing or did not provide race-specific information about prostate cancer risk (525)Lee JR, et al. (2025) JAMA Netw Open, 8: e2530946. .
Downstream effects of such observations are reflected in population-level screening uptake: A 2024 analysis found that Black men had 32 percent less likelihood of getting screened for prostate cancer after the 2018 USPSTF recommendation (see Table 6) (526)VanderVeer-Harris N, et al. (2024) J Med Screen, 31: 239. . When providers do not initiate the conversation or offer race-specific information about prostate cancer risk, as these studies show is common, the burden of pursuing screening falls disproportionately on patients who already face the greatest structural barriers. These findings suggest that reliance on shared decision-making alone may not be sufficient to close existing disparities.
In addition to low uptake among eligible individuals, overscreening outside recommended age groups remains a concern. In 2023, PSA testing was 24 percent higher among men age 70 and older than among those ages 55 to 69, despite not being recommended for the older group (527)Kratzer TB, et al. (2025) CA Cancer J Clin, 75: 485. . Overscreening increases the risk of harm without clear benefit. A recent systematic review found that PSA-based screening offers only modest mortality benefit but carries a substantial risk of overdiagnosis, leading to unnecessary biopsies and treatment, complications, and reduced quality of life, particularly in older or lower-risk populations (528)Oh CU, et al. (2025) Healthcare (Basel), 13. .
Evidence also shows that external disruptions, such as the COVID-19 pandemic, can worsen disparities across population groups (529)Carethers JM (2025) Cancer Prev Res (Phila), 18: 313. . In a nationally representative study of US adults, prostate cancer screening declined during the pandemic period, with eligible men about 14 percent less likely to receive PSA testing in 2021 compared to 2019. This decline was not uniform across populations, as Asian men experienced the largest drop, with screening about 52 percent lower (474)Alba C, et al. (2024) JAMA Health Forum, 5: e235058. .
Transgender women or transfeminine individuals are people who were assigned male at birth, typically have a prostate, and identify as women or along the feminine spectrum. Individuals belonging to this population group face significant disparities in prostate cancer screening, with consistently low screening uptake and uncertain clinical interpretation. In a study of transgender women age 50 years and older, only 23 percent had ever received PSA screening (530)Lacombe-Duncan A, et al. (2025) Urol Oncol, 43: 664 e1. . These findings highlight the urgent need for tailored outreach to vulnerable and understudied populations.
Disparities in Access to High-risk and Hereditary Cancer Surveillance
Beyond population-level screening, individuals with inherited genetic variants or a strong family history of cancer may be candidates for risk-stratified surveillance, a more intensive monitoring approach tailored to their elevated risk. Disparities in access to this form of early detection are substantial and follow patterns similar to those seen in routine screening. For individuals with pathogenic germline variants or strong familial risk for cancer, including carriers of DNA repair gene mutations (e.g., BRCA1, BRCA2, PALB2, and ATM), hereditary pancreatitis genes (e.g., PRSS1), and mismatch repair genes associated with Lynch syndrome (see Genetic Alterations), risk-stratified surveillance offers an opportunity to detect cancer at earlier, more treatable stages. This is especially consequential for individuals who are diagnosed with pancreatic ductal adenocarcinoma (PDAC), a highly lethal cancer with limited population-level screening options and a 5-year survival rate of 14 percent (2)SEER*Explorer: An interactive website for SEER cancer statistics [Internet]. Surveillance Research Program, National Cancer Institute; 2026 Apr 22. [cited 2026 May 11]. Data source(s): SEER Incidence Data, November 2025 Submission (1975-2023), SEER 21 registries. . In a cohort of individuals with genetic or familial predisposition to PDAC, those undergoing surveillance had a higher proportion of stage I cancers at diagnosis (31 percent vs. 10 percent), improved 5-year survival (50 percent vs. 9 percent), and lower cancer-specific mortality (43 percent vs. 86 percent) compared to matched population-based controls (531)Blackford AL, et al. (2024) JAMA Oncol, 10: 1087. . These findings highlight the potential of surveillance to improve outcomes in high-risk populations.
Access to high-risk surveillance requires navigating a multistep process, including risk identification, referral, genetic counseling and testing, and enrollment in a surveillance program. The complexity of this pathway creates points at which disparities can emerge and compound at each stage. Evidence from the international Pancreatic Cancer Early Detection (PRECEDE) Consortium, a large global surveillance registry, shows that among more than 1,200 high-risk individuals, non-White populations are significantly underrepresented relative to demographics of the communities served by participating centers (532)Katona BW, et al. (2023) Cancer Prev Res (Phila), 16: 343. . This underrepresentation persists despite similar willingness of non-White individuals to participate once enrolled, indicating that barriers arise upstream, particularly in risk identification, referral, and access to genetic testing. Across the PRECEDE network, there was also notable heterogeneity in clinical practice; only 44 percent of centers offered the recommended surveillance to BRCA2 carriers without a family history, illustrating how inconsistent guideline interpretation can amplify disparities among those eligible for surveillance (533)Manam A, et al. (2025) JCO Precis Oncol, 9: e2500696. .
Barriers to genetic testing extend beyond PDAC to hereditary cancers broadly. In an analysis of more than 14,500 individuals at risk for hereditary cancer, Black patients were less likely than White patients to complete genetic counseling, a disparity largely attributable to referral processes (534)Wagner IM, et al. (2024) Cancer Epidemiol Biomarkers Prev, 33: 55. . When genetic testing was integrated into the point of care rather than requiring a separate referral, this disparity was no longer observed (534)Wagner IM, et al. (2024) Cancer Epidemiol Biomarkers Prev, 33: 55. , providing a clear example of how modifying care delivery can improve equal access. Community-based research has shed further light on the specific barriers faced by Black and Hispanic individuals at risk for PDAC, including medical mistrust, financial concerns, limited awareness of inherited cancer risk, language barriers, and a lack of culturally concordant provider communication (535)Rodriguez NJ, et al. (2025) Dig Dis Sci, 70: 2635. . Trusted primary care providers were identified as a key facilitator in the risk assessment process, reinforcing the importance of the primary care encounter to hereditary cancer surveillance for underserved populations.
Together, these findings indicate that disparities in access to high-risk and hereditary cancer surveillance are driven by modifiable system-level factors, and that targeted reforms, including integrating genetic risk assessment into primary care, simplifying referral process, and expanding community-based outreach, have the potential to deliver the benefits of surveillance with the populations most likely to benefit (see Policies to Address Disparities in Screening for Hereditary Cancer Syndromes).
Eliminating Disparities in Cancer Screening Through Evidence-based Interventions
A large body of research shows that when screening programs are designed to address structural barriers—such as access to care, logistical constraints, cultural mistrust, and fragmentation of follow-up testing—screening participation and diagnostic completion improve substantially (536)National Cancer Institute. Transforming Research into Community and Clinical Practice. Accessed: March 31, 2026. (537)National Cancer Institute. Division of Cancer Control and Population Sciences. Accelerating Colorectal Cancer Screening and follow-up through Implementation Science (ACCSIS). Accessed: March 31, 2026. . Evidence points to several interventions, including patient navigation, mailed outreach and home-based testing, community engagement strategies, and broader health system redesign, that are particularly effective in improving the uptake of routine screening among underserved population groups.
Overcoming Systemic Barriers Through Health Care Navigation
Patient navigation helps individuals overcome barriers to timely, high-quality cancer care across the continuum from screening through diagnosis and treatment (539)Freeman HP, et al. (2011) Cancer, 117: 3539. . Evidence has consistently proven patient navigation to be one of the most effective strategies for reducing disparities in cancer screening and follow-up care. Navigation programs typically provide individualized assistance with medical appointments, education, transportation, insurance questions, and coordination of diagnostic follow-up after abnormal results. These services directly address many of the logistical and structural barriers that disproportionately affect underserved populations.
A meta-analysis of 42 randomized clinical trials with more than 39,000 participants found that patient navigation significantly improved completion of both screening and diagnostic follow-up for breast and cervical cancers (540)Nelson HD, et al. (2025) JAMA Intern Med, 185: 976. . For breast cancer, navigation increased screening by 50 percent and follow-up by 23 percent. For cervical cancer, the intervention increased screening by 62 percent and follow-up by 63 percent. The effect was particularly strong in medically underserved populations, including racial and ethnic minority groups and individuals with low household income and limited access to health care (540)Nelson HD, et al. (2025) JAMA Intern Med, 185: 976. .
Navigation interventions have also improved screening in populations facing extreme barriers to care, including individuals experiencing homelessness. In a randomized clinical trial within a large Health Care for the Homeless program serving nearly 10,000 patients annually, patient navigation was evaluated for its impact on lung cancer screening in this population that has more than double the lung cancer mortality of the general population (541)Baggett TP, et al. (2024) JAMA Intern Med, 184: 892. (542)Baggett TP, et al. (2015) Am J Prev Med, 49: 694. . Among 260 eligible participants, those receiving navigation were nearly five times more likely to complete LDCT screening within 6 months than those receiving usual care (43 percent vs. 9 percent). The intervention included education, shared decision-making support, appointment coordination, follow-up, and tobacco cessation counseling. Qualitative findings indicated that multidimensional social support and care coordination were central to the intervention’s effectiveness (541)Baggett TP, et al. (2024) JAMA Intern Med, 184: 892. .
Patient navigation also extends to how screening options are delivered, particularly when interventions are designed to meet people where they are. In a randomized trial within a safety-net health system, cervical cancer screening participation increased from 17 percent with telephone reminders alone to 41 percent with mailed self-collection kits and 47 percent when self-collection was combined with patient navigation (544)Montealegre JR, et al. (2025) JAMA Intern Med, 185: 1119. . Conducted in a predominantly racial and ethnic minority population, this study illustrates how combining patient navigation with accessible, home-based options can substantially improve participation in underserved groups.
Navigation is critical for CRC screening because follow-up colonoscopy is required if the results of stool-based testing are abnormal. In a randomized trial across 28 rural clinics serving Medicaid enrollees, mailed stool-based test kits combined with patient navigation more than doubled screening completion within 6 months compared to usual care (12.0 percent vs. 4.5 percent) among 5,614 participants (545)Coronado GD, et al. (2025) JAMA Netw Open, 8: e250928. . The program mailed fecal immunochemical test kits and provided navigation for patients with abnormal results. Implementation was high, with all eligible participants receiving kits and most receiving reminders. Despite these gains, overall participation remained low, highlighting persistent structural barriers. These findings show that combining outreach with navigation improves screening, but additional efforts are needed to increase overall uptake and follow-up (545)Coronado GD, et al. (2025) JAMA Netw Open, 8: e250928. .
Collectively, these studies suggest that patient navigation helps overcome one of the most persistent drivers of disparity: the complexity of the screening continuum (see Figure 12). By actively guiding patients through screening and follow-up, navigation programs can reduce barriers at multiple stages of care.
Building Trust Through Community Engagement
Community trust in medical research and health care systems is shaped by interrelated and often unaddressed factors, including unresolved historical wounds from documented abuses against marginalized populations in medical research—such as the Tuskegee Study, the suppression of Indigenous healing practices, and many others—and the failure to recognize community and Indigenous knowledge or to include communities as equal partners in research design and delivery (see Structural Inequities and Social Injustices) (546)National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Policy and Global Affairs; Roundtable on Black Men and Black Women in Science, Engineering, and Medicine; Laurencin CT, Morgan RC Jr., Bright CM, editors. Leveraging Trust to Advance Science, Engineering, and Medicine in the Black Community: Proceedings of a Workshop. Washington (DC): National Academies Press (US); 2025 Jan 21. 3, Historical Roots of Medical Mistrust. (547)Hall MJ, et al. (2025) Cancers (Basel), 17. . These factors erode trust and limit the effectiveness of interventions across the cancer care continuum in historically marginalized communities (548)Naserrudin NA, et al. (2025) Int J Public Health, 70: 1607763. (549)Rink E, et al. (2024) Prev Sci, 25: 474. (550)Ponce RKM, et al. (2025) J Community Health, 50: 750. . Community engagement strategies that address these drivers through culturally tailored study design and trusted community partnerships have shown promise in improving both awareness and participation in cancer screening among medically underserved populations.
One approach involves the use of community health advisors or community health workers who share cultural, linguistic, or social backgrounds with the populations they serve. In a CRC screening intervention among Black individuals at a community health center, participants were assigned to receive either an educational brochure alone or a more involved intervention that combined tailored education with support from a community health advisor. Over 12 months, stool-based CRC screening increased substantially in both groups, with about 60 percent of participants completing testing. Furthermore, the addition of community health advisor support significantly improved knowledge about CRC and individuals’ understanding of their own risk of developing CRC (551)Luque JS, et al. (2025) BMC Glob Public Health, 3: 47. . Long-term follow-up studies will be important to determine whether an increase in knowledge about benefits and risks of CRC screening leads to increased uptake in routine screening.
Community engagement is particularly important in contexts where the level of trustworthiness in health care systems or cultural stigma associated with routine cancer screening creates barriers to participation. In this regard, faith-based organizations and other trusted local institutions represent important platforms for community engagement. In one study, researchers developed a community-based program with input from members of Black churches to improve awareness and engagement with lung cancer screening using culturally tailored messaging and trained lay health advisors. Pilot testing in community and faith-based settings in New York and New Jersey showed high acceptability, strong participant satisfaction, and increased knowledge about lung cancer screening (552)Carter-Bawa L, et al. (2025) BMC Public Health, 25: 379. . The findings suggest that delivering screening education through trusted community networks and leaders is a feasible and promising approach to reaching eligible Black individuals for lung cancer screening.
Recent evidence also shows the effectiveness of community engagement using digital tools when messaging is culturally tailored and outreach is through trusted partners. In a recent study of a predominantly Hispanic population, a brief bilingual educational video delivered through community health workers, social media, and partner organizations significantly improved breast cancer knowledge, perceived benefits of screening, and intention to receive screening (553)Dadha P, et al. (2026) PEC Innovation, 8: 100470. .
Importantly, these approaches work not only by increasing knowledge but also by reshaping how screening is delivered and perceived, and often by providing navigation to screening. Community-engaged interventions often address multiple barriers simultaneously, including cultural beliefs, language barriers, logistical challenges, access to care, and mistrust of health systems. They also help normalize screening within social networks, which can influence behavior beyond the individual level.
Improving Health Care Access and Health Care System Efficiency
Evidence shows that screening disparities can be significantly reduced by making the health care system easier to navigate and more responsive to the needs of underserved populations. This includes insurance expansion, stronger follow-up, more coordinated care, and better communication between patients and providers.
Studies have consistently shown that expanding access to health insurance and having routine sources of care are among the clearest system-level strategies to reduce disparities. For example, expanding Medicaid eligibility to cover more low-income adults was associated with meaningful increases in cancer screening among Hispanic women in community health centers, particularly for those who were previously uninsured. In states that expanded Medicaid coverage, breast cancer screening increased in Spanish-preferring Hispanic women by 9 percentage points and cervical cancer screening by 11 percentage points compared to similar patients in non-expansion states, with even larger gains over time (554)Holderness H, et al. (2025) Am J Prev Med, 70: 108241. .
In another study, expanding Medicaid eligibility to include low-income adults regardless of immigration status was associated with notable increases in CRC screening among Hispanic patients in community health centers. Screening rates rose by nearly 20 percentage points among uninsured English-preferring patients and by about 9 percentage points among Spanish-preferring Hispanic women compared to similar patients in non-expansion states (555)Huguet N, et al. (2026) JAMA Netw Open, 9: e2559100. . These findings underscore how expanding health insurance coverage alone can substantially increase cancer screening uptake by removing one of the most persistent barriers to care.
Another persistent barrier to reducing screening disparities is how patients interact with health care systems. Research has shown that training clinicians and equipping health systems with resources, such as digital health records, can substantially improve cancer screening in underserved populations. In clinics serving Black communities, implementing risk-adapted PSA guidance with clinician-focused strategies—including presentations, in-clinic reminders, and on-site visits by the research team to review progress of the intervention—increased screening uptake from 19 percent to 33 percent, with greater gains among younger Black men and increased detection of clinically significant cancers (556)Gann PH, et al. (2026) Cancer, 132: e70340. . Similarly, the Pacific Against Cervical Cancer initiative in the US-affiliated Pacific Islands demonstrated that combining provider training, diagnostic laboratory capacity building, and health system improvements, such as better health record collection, can enable adoption of primary HPV screening in low-resource settings (184)Qin J, et al. (2024) J Womens Health (Larchmt), 33: 839. . Together, these studies show that strengthening clinical workflows and infrastructure can reduce disparities by making screening more accessible and actionable.
Having a usual source of care is a critical determinant of cancer screening uptake, particularly among underserved populations. In a national analysis of Hispanic survivors of adolescent and young adult cancer, nearly three-quarters of survivors reported a usual source of care, and within survivors, those connected to care had consistently higher screening participation for CRC, breast, and cervical cancers (557)Choi E, et al. (2026) J Adolesc Young Adult Oncol, 15: 102. . Findings show that those with a usual source of care had nearly double the screening rates for cervical cancer (44.0 percent vs. 25.5 percent) and CRC (43 percent vs. 22 percent), compared to those without a usual source of care. Despite these gains, overall screening rates remained well below national targets, underscoring that establishing a usual source of care is a foundational, but not sufficient, step toward improving cancer screening uptake and reducing disparities (557)Choi E, et al. (2026) J Adolesc Young Adult Oncol, 15: 102. .
Encounters with primary care providers represent critical and underutilized opportunities to initiate timely cancer screening, particularly for underserved populations. Studies have shown that primary care providers can play a pivotal role in helping participate in screening trials (see Equity in Quality Cancer Care). A study of patients with a documented smoking history found that only one-third of eligible individuals reported the provider discussing lung cancer screening with them. In the same study population, 90 percent of individuals who were eligible reported that their provider had discussed CRC screening with them (558)Japuntich SJ, et al. (2024) BMC Prim Care, 25: 202. . Importantly, when screening was discussed and recommended, completion rates were high for both cancer types, highlighting that gaps in provider-initiated screening conversations with patients are a key driver of missed opportunities (558)Japuntich SJ, et al. (2024) BMC Prim Care, 25: 202. .
Research has shown that patient–provider concordance can also help improve preventive care by building trust, improving communication, and strengthening patient engagement. In a nationally representative sample, women with sex-concordant clinicians had higher uptake of breast (85.0 percent vs. 80.5 percent), cervical (87 percent vs. 80 percent), and CRC screening (81 percent vs. 77 percent). Racial and ethnic concordance with providers was uncommon among non-White populations, often below 25 percent, indicating the importance of diversifying the workforce (see Disparities in the Cancer Training Pathway and Cancer Research and Care Workforce) (559)Green AL, et al. (2026) J Gen Intern Med, 41: 767. . There is also evidence that removing language barriers between patients and providers can further improve the quality of cancer care, including improved screening uptake (560)van Lent LGG, et al. (2025) Patient Educ Couns, 136: 108767. (561)Kim HS, et al. (2025) BJC Rep, 3: 80. .
Studies consistently show that the capacity of the health care system, including how practices are organized and staffed, plays a meaningful role in whether patients receive recommended cancer screenings. A study of more than 100,000 Medicaid enrollees found that patients seen by mid-sized group practices were approximately 20 percent more likely to receive breast and cervical cancer screening during the COVID-19 pandemic than those seen by solo providers (562)Corredor-Waldron A, et al. (2026) Health Serv Res, 61: e70030. . Larger medical practices were better able to maintain routine screening overall, likely because they had greater capacity to absorb disruption caused by the pandemic through backup staffing, patient tracking systems, and administrative infrastructure. These findings suggest that investments in organizational capacity at safety-net institutions, such as Federally Qualified Health Centers and Medicaid-serving primary care practices, are as important as individual outreach efforts in closing persistent screening gaps (562)Corredor-Waldron A, et al. (2026) Health Serv Res, 61: e70030. .
Effective interventions reduce disparities in screening uptake by addressing awareness, logistical barriers, and access to care, but their impact is limited by persistent system-level barriers that require coordinated policy and programmatic solutions. Realizing the full potential of cancer screening to reduce mortality across all populations requires targeted and sustained efforts by health systems, researchers, and policymakers to eliminate the barriers that limit equitable access.
Next Section: Disparities in Clinical Research and Cancer Treatment Previous Section: Disparities in the Burden of Modifiable Behavioral Cancer Risk Factors