- Challenges Faced by Cancer Survivors
- Physical Challenges
- Psychosocial Challenges
- Financial Challenges
- Unique Challenges Faced by Older Adult Cancer Survivors
- Unique Challenges Faced by Childhood, Adolescent, and Young Adult Cancer Survivors
- Strategies to Address Disparities in Cancer Survivorship
- Future Directions in Cancer Survivorship
Disparities in Cancer Survivorship
In this section, you will learn:
- Cancer survivorship is a growing public health priority, with more than 18.6 million survivors living in the United States in 2025. Yet substantial disparities in cancer survivorship persist across populations defined by race, ethnicity, geographic location, socioeconomic status, sexual orientation, and gender identity.
- Cancer survivors experience a wide range of long-term physical, psychosocial, and financial challenges, including late effects of treatment, mental health burdens, and financial toxicity, all of which can adversely affect quality of life.
- Medically underserved populations shoulder a disproportionate burden of survivorship challenges due to a complex interplay of systemic and structural barriers, social drivers of health, and financial constraints that limit access to high-quality survivorship care and supportive services.
- Certain survivor groups—including older adults and childhood, adolescent, and young adult cancer survivors—face unique and complex survivorship needs, requiring tailored, risk-based, and coordinated care approaches.
- Eliminating disparities in survivorship requires strategies that integrate supportive care, strengthen care coordination and follow-up, and address the broader social, economic, and structural drivers of inequities through patient-centered, multilevel approaches such as patient navigation, telehealth, and community partnerships.
- Emerging national survivorship care standards provide a framework to address disparities in survivorship outcomes by improving care coordination across health systems, expanding access to survivorship services, and supporting patient-centered, multidisciplinary care.
Contents
According to the National Cancer Institute (NCI), a person is considered a cancer survivor from the time of cancer diagnosis through the balance of the person’s life (789)Mollica MA, et al. (2025) Cancer, 131: e70039. . Unprecedented advances in cancer treatments over the past decade have led to more patients living longer and fuller lives after a cancer diagnosis. As of January 1, 2025, more than 18.6 million adults and children with a history of cancer were living in the United States (US), and this number is projected to exceed 22 million by 2035 (4)Wagle NS, et al. (2025) CA Cancer J Clin, 75: 308. .
Although these trends reflect substantial progress, advances in cancer prevention, detection, and treatment have not benefited all groups equally. Medically underserved populations continue to experience higher cancer-related morbidity and mortality (17)Islami F, et al. (2026) CA Cancer J Clin, 76: e70045. , and survivors from racial and ethnic minority groups, rural communities, low-income populations, and individuals belonging to sexual and gender minority (SGM) populations often encounter greater barriers to high-quality survivorship care and supportive services. As the US population ages and becomes more diverse, the number of survivors from historically underserved groups will continue to grow. Without focused efforts to ensure equitable access to high-quality survivorship care and support, disparities in long-term health outcomes and quality of life may persist or worsen.
As more people are living longer and fuller lives after a cancer diagnosis, a greater understanding of survivorship experiences is needed. These experiences include the physical, psychosocial, and financial adversities caused by a cancer diagnosis. Many cancer survivors also experience late effects or secondary health problems due to their cancer, cancer treatments, or both, and therefore require long-term follow-up care that includes screening for these late effects. While all cancer survivors have unique experiences, those from medically underserved populations often experience a greater burden of the adverse effects of cancer survivorship. Understanding the challenges faced by these groups will help inform cancer care strategies and personalized recommendations for those who are more vulnerable, ultimately improving long-term health outcomes and quality of life.
A diagnosis of cancer also impacts friends, family members, and other caregivers, who often serve as the primary support network of the survivor. Caregivers from medically underserved populations frequently face additional financial, emotional, and logistical burdens that can compound the challenges of survivorship. As a result, survivorship research, support, and care must extend beyond the cancer patient and survivor to include individuals who make up the broader support network.
The following sections highlight the challenges faced by cancer survivors and their support network, strategies to improve survival and quality of life, and approaches that have been shown to deliver survivorship care most effectively.
Challenges Faced by Cancer Survivors
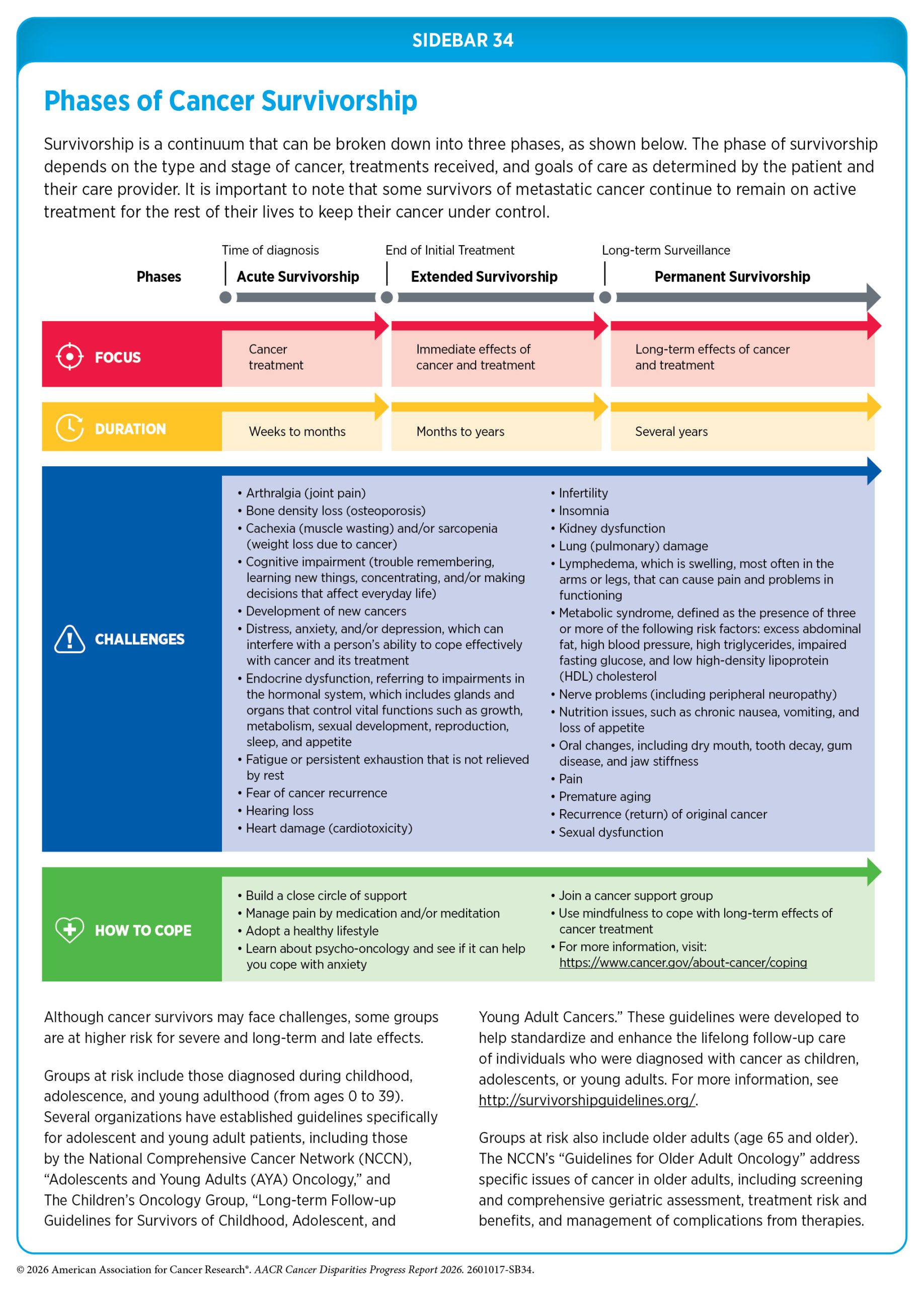
Depending on the cancer type and stage, as well as the age at diagnosis, survivorship encompasses a broad range of experiences related to living with, through, and beyond cancer (see Sidebar 34). Cancer survivors often face physical, psychosocial, and financial challenges that arise from the cancer itself and its treatment. These challenges can emerge during treatment or long after its completion, requiring ongoing care and support. Importantly, these burdens are not distributed equally. Survivors from medically underserved populations experience greater barriers to high-quality survivorship care, contributing to persistent disparities in long-term health outcomes and quality of life.
Physical Challenges
Survivors can experience a wide range of short- and long-term symptoms caused by cancer or its treatments. Short-term effects include hair loss, pain, nausea, vomiting, and loss of smell and appetite with varying severity of symptoms depending on the person, cancer type, and treatment regimen. As cancer survivors are living longer because of better therapies, the development of long-term side effects such as heart damage (cardiotoxicity), lung damage, loss of bone density, and treatment-related cognitive impairment is becoming more common. Growing evidence shows that medically underserved populations experience a higher burden of late effects of cancer treatment, including cardiovascular complications, lymphedema, peripheral neuropathy, metabolic disorders, and second primary cancers (790)Hassan AM, et al. (2025) Breast Cancer Res Treat, 215: 1. (791)Yarosh RA, et al. (2025) Cancer, 131: e35650. (792)Brandt C, et al. (2024) Int J Cancer, 155: 996. (793)Diaz AE, et al. (2026) JNCI Cancer Spectr, 10. (794)Ho K, et al. (2025) Cancer Causes Control, 36: 1813. (795)Zhang L, et al. (2025) J Am Heart Assoc, 14: e037780. (796)Schneider BP, et al. (2015) Clin Cancer Res, 21: 5082. .
Chronic pain, defined as persistent or recurrent pain lasting longer than 3 months, is one of the most common long-term effects of cancer treatment, occurring in approximately 40 percent of cancer survivors worldwide (797)Joshy G, et al. (2023) BMC Cancer, 23: 774. (798)Zhang Y, et al. (2025) BMC Public Health, 25: 325. . Cancer-related chronic pain is associated with reduced quality of life and increased risk of all-cause and cancer-specific mortality among survivors (797)Joshy G, et al. (2023) BMC Cancer, 23: 774. (798)Zhang Y, et al. (2025) BMC Public Health, 25: 325. . However, this burden is not equally shared across geographic regions. National data show that rural cancer survivors are more likely to experience chronic pain compared to urban survivors (799)Choi H, et al. (2025) JAMA Netw Open, 8: e2549972. . Survivors with lower incomes, less than a 4-year college degree, and comorbid health conditions are also more likely to experience chronic pain than their respective counterparts (799)Choi H, et al. (2025) JAMA Netw Open, 8: e2549972. . Racial and ethnic disparities in pain management are also evident. In a recent study of over 300,000 cancer survivors, Black and Asian or Pacific Islander (API) survivors had lower utilization of pain management treatments compared to White survivors (800)Bhattacharyya O, et al. (2026) Cancer Med, 15: e71536. . Among those receiving opioid pain medications, survivors from racial and ethnic minority groups received lower doses than White survivors, highlighting disparities in access to symptom management and supportive care resources.
Adult cancer survivors in the United States experience higher rates of physical disability than adults without a history of cancer (801)Brown JC, et al. (2025) JNCI Cancer Spectr, 9. (802)Cao C, et al. (2024) J Clin Oncol, 42: 2257. . Physical disabilities include limitations in mobility and self-care that affect an individual’s ability to move independently or perform basic daily activities. According to a recent study, more than one in four cancer survivors reported a mobility disability, defined as serious difficulty walking or climbing stairs, and nearly one in 10 reported a self-care disability, such as difficulty dressing or bathing (802)Cao C, et al. (2024) J Clin Oncol, 42: 2257. . Mobility and self-care disabilities were more common among survivors from racial and ethnic minority groups; individuals with lower income and educational attainment; and those with comorbid conditions or cancer-related pain. Evidence also indicates that SGM cancer survivors experience a disproportionate burden of disability and functional limitations, including a higher likelihood of hearing and vision disability, difficulty in daily activities (e.g., walking, dressing, and running errands), and cognitive limitations (difficulties with memory, attention, or decision-making), compared to non-SGM survivors, with the greatest burden observed among transgender and gender nonconforming individuals (803)Waters AR, et al. (2024) Cancer Epidemiol Biomarkers Prev, 33: 1405. .
Many common cancer therapies can adversely affect the cardiovascular system, contributing to long-term morbidity and mortality among cancer survivors (804)Li Q, et al. (2025) EClinicalMedicine, 84: 103274. (805)Strongman H, et al. (2022) JACC CardioOncol, 4: 113. . This treatment-related heart damage, known as cardiotoxicity, can occur during or after cancer therapy. Certain chemotherapeutic agents (e.g., anthracyclines), targeted therapies, and radiation exposure can cause cardiotoxicity, leading to cardiomyopathy, coronary artery disease, heart failure, and other cardiovascular complications (804)Li Q, et al. (2025) EClinicalMedicine, 84: 103274. . This risk, however, is not evenly distributed.
In a diverse cohort of patients treated with anthracyclines, Black and Hispanic patients had more than twice the risk of treatment-related cardiotoxicity and experienced greater declines in left ventricular function (the heart’s ability to pump blood effectively) compared to White patients (795)Zhang L, et al. (2025) J Am Heart Assoc, 14: e037780. . Cancer survivors also face elevated risks of developing cardiometabolic conditions and cardiovascular disease after diagnosis. In a large cohort of breast cancer survivors, Black and Asian women had higher risks of hypertension, diabetes, and cardiovascular disease compared to White women (793)Diaz AE, et al. (2026) JNCI Cancer Spectr, 10. . Disaggregated analysis of Asian subgroups further revealed that Filipino women had a higher risk of stroke, while South Asian women had elevated risks of coronary artery disease and heart failure, underscoring important heterogeneity in cardiovascular outcomes within Asian populations (793)Diaz AE, et al. (2026) JNCI Cancer Spectr, 10. .
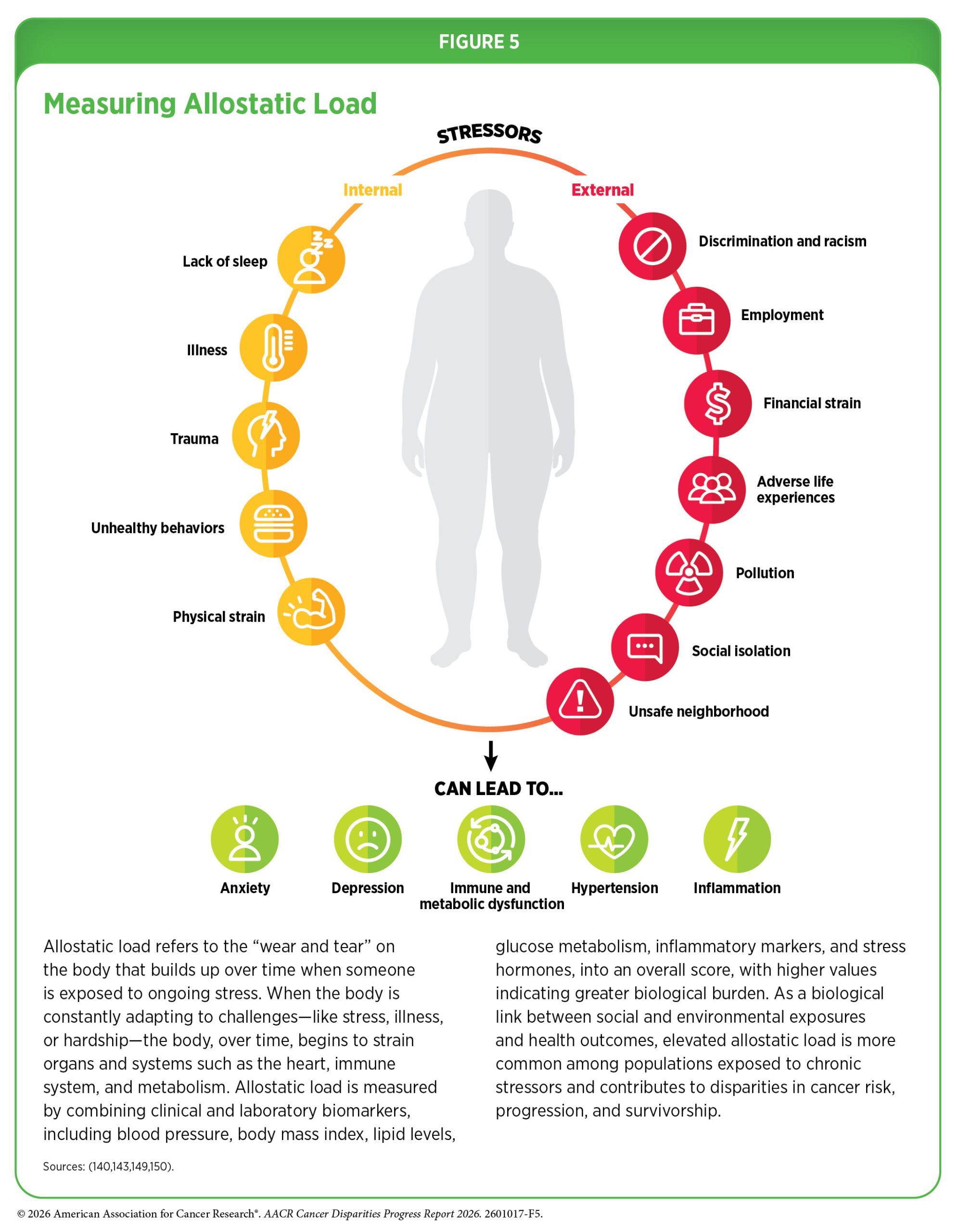
Lymphedema results from damage to the lymphatic system caused by cancer surgery or radiation therapy. This damage disrupts normal drainage of lymphatic fluid, leading to accumulation in surrounding tissues and resulting in painful swelling, most commonly in the arms and legs (806)Cheville AL, et al. (2025) BMJ, 390. . Research shows that not all cancer survivors are equally affected by lymphedema. Among long-term breast cancer survivors, Black women were significantly more likely than White women to experience persistent lymphedema (791)Yarosh RA, et al. (2025) Cancer, 131: e35650. . Where a person lives and the resources available in their community can also influence lymphedema risk. A recent study found that patients living in the most socioeconomically disadvantaged neighborhoods had substantially higher rates of breast cancer–related lymphedema than those living in more advantaged areas (16.3 percent vs. 3.9 percent) (790)Hassan AM, et al. (2025) Breast Cancer Res Treat, 215: 1. . Emerging research suggests that the stress of long-term social and economic hardship may also increase the risk of lymphedema. In a cohort of more than 3,000 breast cancer survivors, individuals with higher allostatic load—a measure of the body’s cumulative physiologic “wear and tear” from chronic stress (see Figure 5)—had higher odds of developing lymphedema compared to those with lower allostatic load (807)Obeng-Gyasi B, et al. (2025) Support Care Cancer, 33: 311. . Survivors who developed lymphedema were more likely to be Black and insured through Medicaid, highlighting how social and economic disparities can influence survivorship outcomes through biological pathways.
Chemotherapy-induced peripheral neuropathy (CIPN) is a common and often debilitating adverse effect of cancer treatment. Symptoms of CIPN include numbness, tingling, burning, painful, or electric shock–like sensations in the hands and feet that can impair daily functioning and overall quality of life (808)Karschnia P, et al. (2025) Nat Rev Cancer, 25: 887. . In severe cases, CIPN may require dose reductions or early treatment discontinuation to alleviate symptoms, potentially compromising treatment effectiveness and survival (808)Karschnia P, et al. (2025) Nat Rev Cancer, 25: 887. . Racial and ethnic disparities in CIPN are significant, with Black patients experiencing higher incidence and greater severity of neuropathy than White patients (796)Schneider BP, et al. (2015) Clin Cancer Res, 21: 5082. (809)Schneider BP, et al. (2024) J Clin Oncol, 42: 2899. . Several factors may contribute to this disparity, including higher prevalence of comorbidities such as diabetes and obesity, lower levels of vitamin D, preexisting nerve problems, and differences in how the body processes chemotherapy drugs (810)Nguyen-Hoang N, et al. (2025) Crit Rev Oncol Hematol, 211: 104739. . Emerging evidence suggests that the type of chemotherapy used may influence CIPN risk among Black patients. In particular, docetaxel and paclitaxel—two commonly used taxane chemotherapy drugs—have been associated with different CIPN risks among Black patients, with lower rates of CIPN observed among patients receiving docetaxel (809)Schneider BP, et al. (2024) J Clin Oncol, 42: 2899. . Additional research in diverse populations is needed to confirm these findings and inform treatment decisions that may help reduce disparities in CIPN risk.
Second primary cancers (SPCs) represent another important long-term risk faced by cancer survivors, and this risk is not evenly distributed across populations. Unlike recurrence of the original cancer, an SPC represents a new, biologically distinct cancer that can emerge months or years after the initial cancer has been diagnosed and treated. In a study of breast cancer survivors, API, Black, and Hispanic survivors experienced approximately 40 percent to 49 percent higher risk of developing an SPC while White women had a 9 percent higher risk compared to their racial and ethnic counterparts in the general population (792)Brandt C, et al. (2024) Int J Cancer, 155: 996. . Disparities also extend to survival after an SPC diagnosis. A recent analysis found that SPCs were associated with nearly six-fold higher risk of death among Pacific Islander survivors compared to their counterparts without an SPC, while White survivors experienced approximately 3.7-fold higher risk (811)Shao L, et al. (2025) J Natl Cancer Inst. .
Differences in SPC risk have also been observed across community and environmental contexts. For example, one study found that cancer survivors living in counties with higher smoking prevalence experience substantially higher risk of developing SPCs than those living in counties with lower smoking prevalence (812)Cheng HG, et al. (2026) Cancer Epidemiol Biomarkers Prev, 35: 165. . Similarly, an analysis of breast cancer survivors showed that those living in lower-income counties had a 7 percent higher risk of SPCs than those living in higher-income counties, while survivors living in rural counties had a 12 percent higher risk than those in urban areas (794)Ho K, et al. (2025) Cancer Causes Control, 36: 1813. . Notably, the highest risk was observed among survivors living in rural, low-income counties, who experienced a 20 percent higher risk of developing an SPC than those living in higher-income urban counties.
Psychosocial Challenges
A cancer diagnosis can pose serious challenges to an individual’s mental and emotional well-being. Studies consistently show that cancer survivors experience higher rates of mental health disorders than individuals without a history of cancer, including elevated risks of anxiety, depression, self-harm, and suicide (813)Forbes H, et al. (2024) EClinicalMedicine, 76: 102826. . Psychosocial challenges may arise during active treatment but often persist well into survivorship.
Mental health challenges do not affect all survivors equally. Socioeconomic disadvantage is strongly associated with worse psychological outcomes across the survivorship trajectory. Survivors with lower socioeconomic status (SES) experience higher levels of psychological distress and are more likely to meet criteria for mental health disorders (815)Springer F, et al. (2025) Psychooncology, 34: e70059. . Neighborhood-level deprivation and adverse social drivers of health (SDOH)—including lack of economic stability and barriers to health care access—have been associated with higher anxiety and depressive symptoms and poorer mental well-being among individuals with cancer (see Understanding and Addressing Drivers of Cancer Disparities) (816)Balogun Z, et al. (2024) JAMA Otolaryngol Head Neck Surg, 150: 295. (817)Zhong M, et al. (2026) Eur J Oncol Nurs, 80: 103103. . Material hardship—defined as the inability to meet basic needs such as food, housing, and medical care—can further compound these challenges. Housing instability, for example, has been associated with clinically meaningful increases in anxiety and depression among survivors, highlighting how unmet basic needs can directly affect mental health (818)Robinson JRM, et al. (2025) J Cancer Surviv, 19: 356. .
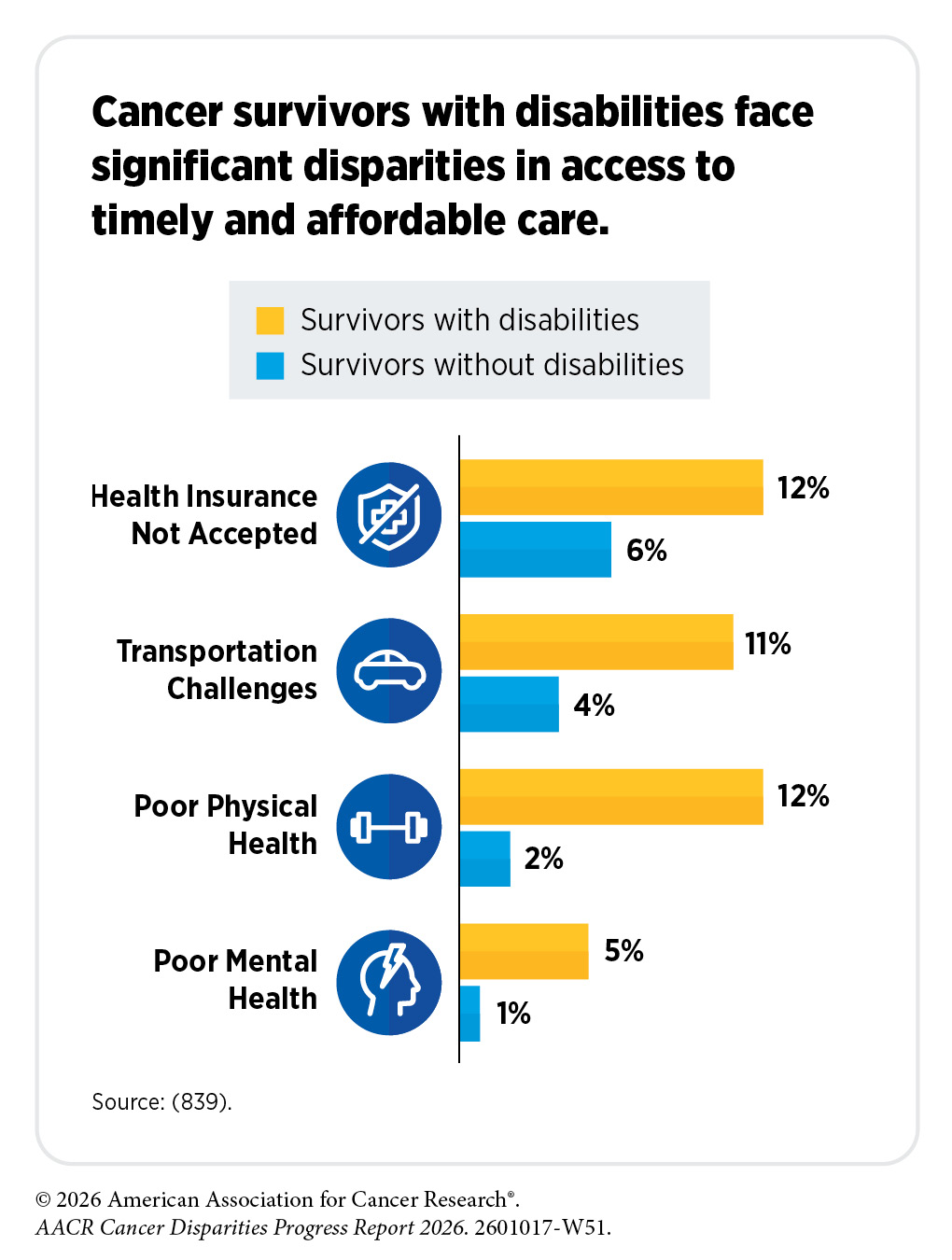
Cancer survivors living with disabilities may face additional challenges that compound psychosocial burdens. Evidence shows that individuals with intellectual, developmental, or functional disabilities experience greater severity of anxiety, depression, and psychological distress than survivors without these disabilities, reflecting complex care needs and interconnected barriers to appropriate support (819)Giblon R, et al. (2025) Psychooncology, 34: e70199. (820)Mevawalla A, et al. (2026) J Cancer Surviv. .
Racial and ethnic disparities in mental health burden are also well documented among cancer survivors. Studies of colorectal and ovarian cancer survivors have shown worse self-reported mental health and overall well-being among Hispanic and Black survivors compared to White survivors (821)Mahoney DE, et al. (2024) Gynecol Oncol, 189: 24. (822)Yoon PS, et al. (2024) Qual Life Res, 33: 793. . These disparities extend beyond symptom burden to include inequities in the diagnosis and treatment of mental health conditions. For example, despite evidence of comparable or greater mental health burden, Black, Asian, and Hispanic survivors are less likely to be diagnosed with anxiety or depression than White survivors, suggesting potential underdiagnosis and barriers to accessing mental health care (823)Gallagher TJ, et al. (2025) Head Neck, 47: 1885. . National data also show lower use of antidepressant and anti-anxiety medications among Black and Hispanic survivors overall, as well as among individuals with lower income or inadequate insurance coverage, compared to more advantaged counterparts (824)Miro-Rivera D, et al. (2025) JAMA Netw Open, 8: e2527585. . These treatment differences likely reflect both lower rates of diagnosis and disparities in access to and utilization of mental health care.
Discrimination is a significant social stressor that can exacerbate mental health challenges among cancer survivors, particularly those from racial and ethnic minority groups and SGM populations. Minority survivors who experience discrimination in medical settings or in daily life report poorer mental and physical health-related quality of life and greater psychological distress than those who do not report such experiences (825)Arizpe A, et al. (2025) J Racial Ethn Health Disparities, 12: 1765. (826)Franco-Rocha OY, et al. (2025) Psychooncology, 34: e70154. (827)Karvonen KA, et al. (2023) Cancer, 129: 3023. . These experiences can erode trust in the health care system, discouraging engagement with follow-up and supportive care (828)Brown JA, et al. (2024) J Natl Cancer Inst, 116: 1845. (829)Garrett E, et al. (2024) J Natl Cancer Inst, 116: 258. . In a national study of lesbian, gay, bisexual, and transgender cancer survivors, bisexual and transgender individuals reported higher levels of discrimination and psychosocial stress than lesbian and gay survivors, and were more likely to experience substantial barriers to survivorship care (684)Brown-Savita M, et al. (2026) Cancers (Basel), 18. . Survivors with intersecting marginalized identities may face additional stressors that further intensify these challenges (826)Franco-Rocha OY, et al. (2025) Psychooncology, 34: e70154. (830)Boehmer U, et al. (2022) Cancer, 128: 284. . Reducing disparities in mental health care among cancer survivors will require addressing discrimination within health care systems and improving access to culturally responsive, affirming mental health services for survivors belonging to racial and ethnic minority and SGM groups.
Mental health challenges are a common and enduring component of cancer survivorship, shaped by social, economic, structural, and health system factors. Addressing psychosocial distress in survivorship requires not only routine mental health screening and access to mental health services, but also evidence-based approaches that address SDOH, improve culturally responsive care, and reduce structural barriers to supportive services. These interventions should also be tailored to the cultural and community contexts of survivors experiencing disparities to ensure that services address unmet needs and are accessible, acceptable, and effective.
Financial Challenges
Financial toxicity refers to the financial burden and distress experienced by patients and their families as a result of cancer diagnosis and treatment. Evidence suggests that nearly half of cancer survivors experience some degree of financial hardship due to high out-of-pocket medical costs, loss of income from employment disruptions, and gaps or limitations in insurance coverage (831)Kitaw TA, et al. (2025) BMJ Glob Health, 10. (832)Mollica MA, et al. (2024) Support Care Cancer, 32: 137. (833)Yabroff KR, et al. (2024) CA Cancer J Clin, 74: 341. . Survivors experiencing financial hardship are more likely to delay or forgo medical care, skip medications, and postpone supportive care services, undermining treatment effectiveness and quality of life (832)Mollica MA, et al. (2024) Support Care Cancer, 32: 137. (834)Anant S, et al. (2025) JCO Oncol Pract, 21: 41. . Those facing financial hardship are also more likely to report health-related social needs, including food insecurity, housing instability, and transportation barriers (834)Anant S, et al. (2025) JCO Oncol Pract, 21: 41. (835)Myers S, et al. (2025) Support Care Cancer, 33: 339. (836)Pak TY (2025) Health Econ Rev, 15: 22. . Financial toxicity is driven by structural inequities and SDOH, disproportionately affecting medically underserved populations. Understanding these disparities is essential to designing survivorship care models and policies that promote equitable access to care and long-term financial well-being.
Racial and ethnic disparities in financial toxicity are well documented. Evidence shows that a cancer diagnosis is associated with significant declines in income and wealth, with disproportionately greater losses among Black and Hispanic survivors, exacerbating preexisting economic disadvantage (837)Hammarlund N, et al. (2025) J Cancer Surviv. . These financial burdens can compound barriers to recommended treatment and follow-up care. For example, American Indian or Alaska Native (AIAN), Hispanic, Black, and multiracial survivors are more likely than White survivors to forgo physician visits because of cost (838)Gu C, et al. (2024) J Cancer Surviv, 18: 385. .
Financial hardship among AIAN and Asian cancer survivors reflects distinct structural, geographic, and cultural factors. Native American patients, many of whom reside in rural or remote areas, often face substantial financial challenges related to cancer treatment, including transportation and lodging costs to reach distant treatment centers, limited private insurance coverage, and resource gaps that can delay care and increase out-of-pocket expenses. Limited access to coordinated services across health care systems, including external, tribal, and those operated by the Indian Health Service, can further complicate care delivery and increase financial strain (840)Anderson-Buettner AS, et al. (2024) BMC Health Serv Res, 24: 928. .
Among Asian American populations, financial toxicity is frequently underrecognized because diverse subgroups are often aggregated into a single category (see Sidebar 4). Substantial heterogeneity in SES, health insurance coverage, language proficiency, and immigration status contributes to differences in financial vulnerability across ethnic subgroups (841)Wang S, et al. (2024) JAMA Oncol. , and cultural norms emphasizing family-centered caregiving and financial responsibility may amplify financial strain to extended households (842)Garg S, et al. (2025) Support Care Cancer, 33: 91. . Disaggregated data and culturally responsive approaches are essential to identifying subgroup-specific needs and informing targeted interventions—such as financial navigation, assistance programs, and policy changes—to reduce financial hardship in these populations.
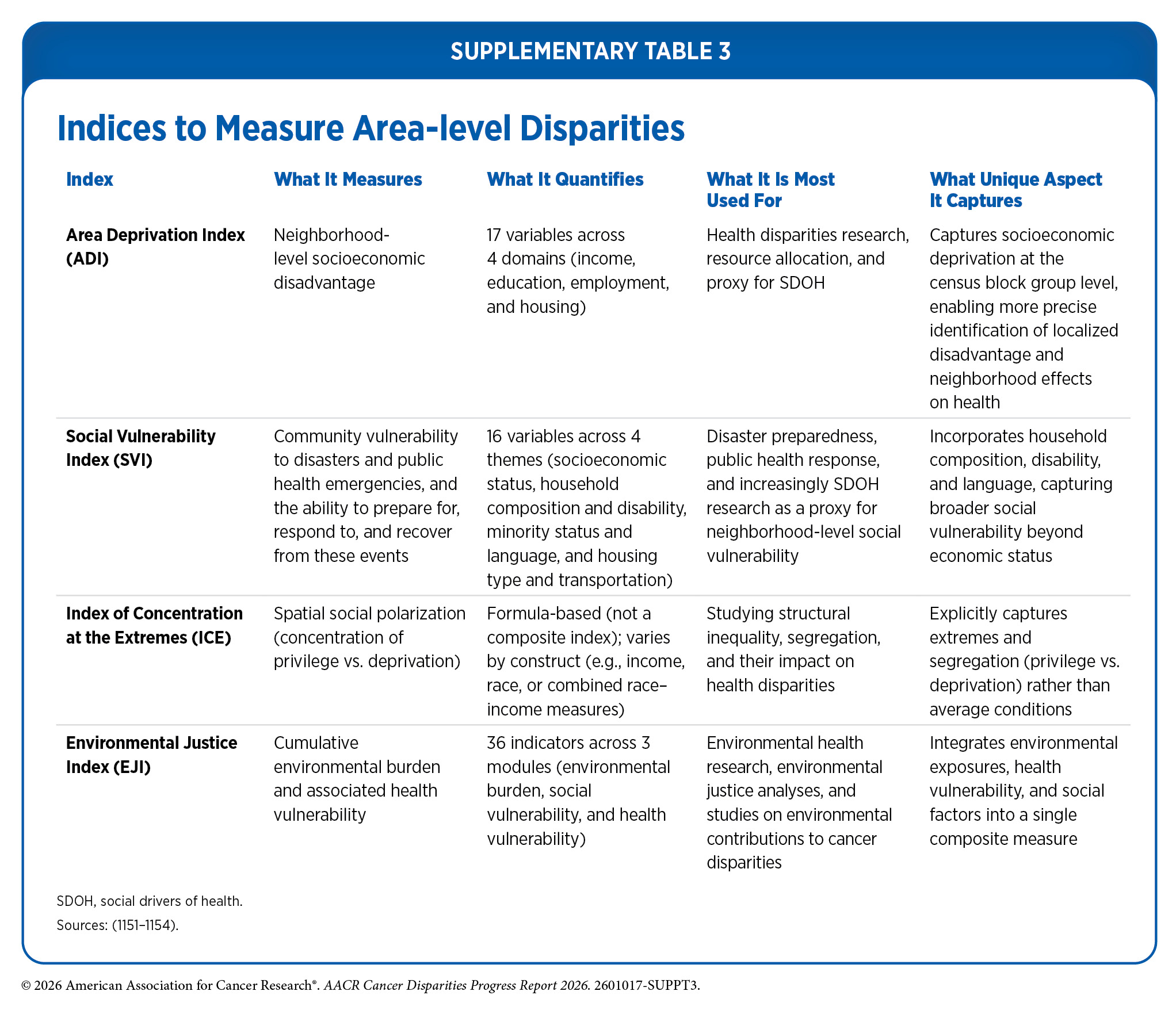
Financial toxicity disproportionately affects cancer survivors living in poverty. This burden is shaped not only by individual income (see Socioeconomic Status (SES)), but also by structural barriers and community-level factors. Social vulnerability refers to the demographic and socioeconomic conditions—such as poverty, limited access to transportation, and crowded housing—that adversely affect health and economic stability (see Social and Built Environments and Supplementary Table 3). Survivors living in socially vulnerable communities experience greater financial hardship than those in less vulnerable areas, underscoring the compounding effects of place-based disadvantage (843)Dhir A, et al. (2024) JAMA Netw Open, 7: e2429286. .
Neighborhood socioeconomic context also influences survivors’ ability to remain productive in the workforce. According to a 2025 study, cancer survivors miss, on average, approximately one month of work per year due to cancer or treatment-related late effects, including fatigue, pain, and other physical and cognitive limitations (844)Deng YF, et al. (2025) J Psychosoc Oncol: 1. . However, this burden is not evenly distributed; survivors living in lower-income neighborhoods missed, on average, at least an additional week (8 to 9 days) of work annually compared to survivors in higher-income neighborhoods, highlighting disparities in work disruption that may exacerbate financial strain during survivorship (844)Deng YF, et al. (2025) J Psychosoc Oncol: 1. .
SGM cancer survivors also face substantial financial toxicity. In a national study of more than 36,000 survivors, lesbian, gay, bisexual, transgender, queer or questioning, and other SGM individuals experienced significantly higher rates of financial hardship and care disruptions than non-SGM survivors (845)Waters AR, et al. (2025) Cancer Control, 32: 10732748251351105. . The burden was greatest among gender minority survivors, bisexual women, and SGM survivors of color. These findings highlight the compounded effects of intersecting marginalized identities and emphasize the need for addressing financial toxicity among SGM survivors through interventions that span clinical care, health systems, workplace protections, and policy reform.
Unique Challenges Faced by Older Adult Cancer Survivors
Older adults, defined as individuals age 65 and over, represent the fastest-growing segment of the cancer survivor population. In 2022, older adults accounted for 67 percent of all cancer survivors in the United States, and this proportion is projected to rise to 73 percent by 2040 (846)Bluethmann SM, et al. (2016) Cancer Epidemiol Biomarkers Prev, 25: 1029. (847)Miller KD, et al. (2022) CA Cancer J Clin, 72: 409. . As the population of older cancer survivors continues to grow, so too does the need to understand and address the unique challenges they face throughout survivorship.
Cancer and its treatments in older adults occur in the context of normal aging processes and a higher burden of chronic health conditions. It is estimated that more than 90 percent of older adults with cancer have at least one chronic condition—such as cardiovascular disease, hypertension, obesity, or diabetes—and over 30 percent live with three or more comorbidities (848)Chen W, et al. (2024) J Natl Cancer Inst, 116: 1730. (849)Rees-Punia E, et al. (2024) Cancer, 130: 312. (850)Williams GR, et al. (2018) Oncologist, 23: 433. . Cancer and its treatments can also increase vulnerability to geriatric conditions that may compromise independence and quality of life. Frailty—an age-related condition characterized by weakness, fatigue, slower movement, weight loss, and diminished physical functioning—is associated with increased risk of disability, poor quality of life, and mortality among older cancer survivors (851)Singla C, et al. (2026) Clinical Oncology: 104097. (852)Duchesneau ED, et al. (2025) JAMA Netw Open, 8: e250614. (853)Lee HN, et al. (2025) J Geriatr Oncol, 16: 102277. . Cancer and its treatments can further accelerate frailty and functional decline and contribute to the accumulation or worsening of chronic health conditions in this age group (852)Duchesneau ED, et al. (2025) JAMA Netw Open, 8: e250614. (854)Sedrak MS, et al. (2024) J Cancer Surviv, 18: 1131. .
The high prevalence of chronic health conditions among older cancer survivors often results in the use of multiple medications. Polypharmacy, defined as the routine use of five or more medications, is common among older adults with cancer (855)Masnoon N, et al. (2017) BMC Geriatr, 17: 230. . Complex medication regimens used to manage both cancer-related symptoms and chronic conditions can increase the risk of drug interactions, medication-related complications, and declines in physical functioning (856)La J, et al. (2025) J Natl Compr Canc Netw, 23: 363. (857)Mohamed MR, et al. (2024) Support Care Cancer, 32: 674. . These challenges can impair treatment management and increase the overall burden of survivorship care for older adults.
In addition to physical health challenges, older cancer survivors frequently experience psychosocial and financial burdens that can affect quality of life and access to care. Mental health conditions, such as anxiety and depression, are common among older cancer survivors and may persist or emerge years after diagnosis (858)Taylor M, et al. (2025) JAMA Netw Open, 8: e2544812. . In a study of Medicare beneficiaries with cancer, nearly one in three patients had a diagnosis of anxiety or depression, and newly diagnosed mental health conditions were associated with significantly higher health care costs compared to patients without these conditions (859)Birch K, et al. (2023) JCO Oncol Pract, 19: e660. . Social isolation and loneliness are also prevalent among older cancer survivors and have been linked to poorer health outcomes and increased risk of death (860)Pilleron S, et al. (2023) J Geriatr Oncol, 14: 101519. (861)Zhao J, et al. (2024) J Natl Compr Canc Netw, 22: 244. . Older cancer survivors are also vulnerable to financial toxicity despite having health insurance through Medicare (835)Myers S, et al. (2025) Support Care Cancer, 33: 339. (862)Davis ES, et al. (2024) Cancer, 130: 3487. . Studies show that cancer-related costs, including treatment expenses, transportation, and other out-of-pocket costs, can contribute to financial hardship, food insecurity, and difficulties meeting basic needs among older adults living with and beyond cancer (835)Myers S, et al. (2025) Support Care Cancer, 33: 339. (836)Pak TY (2025) Health Econ Rev, 15: 22. (862)Davis ES, et al. (2024) Cancer, 130: 3487. (863)Owsley KM, et al. (2025) J Cancer Surviv. .
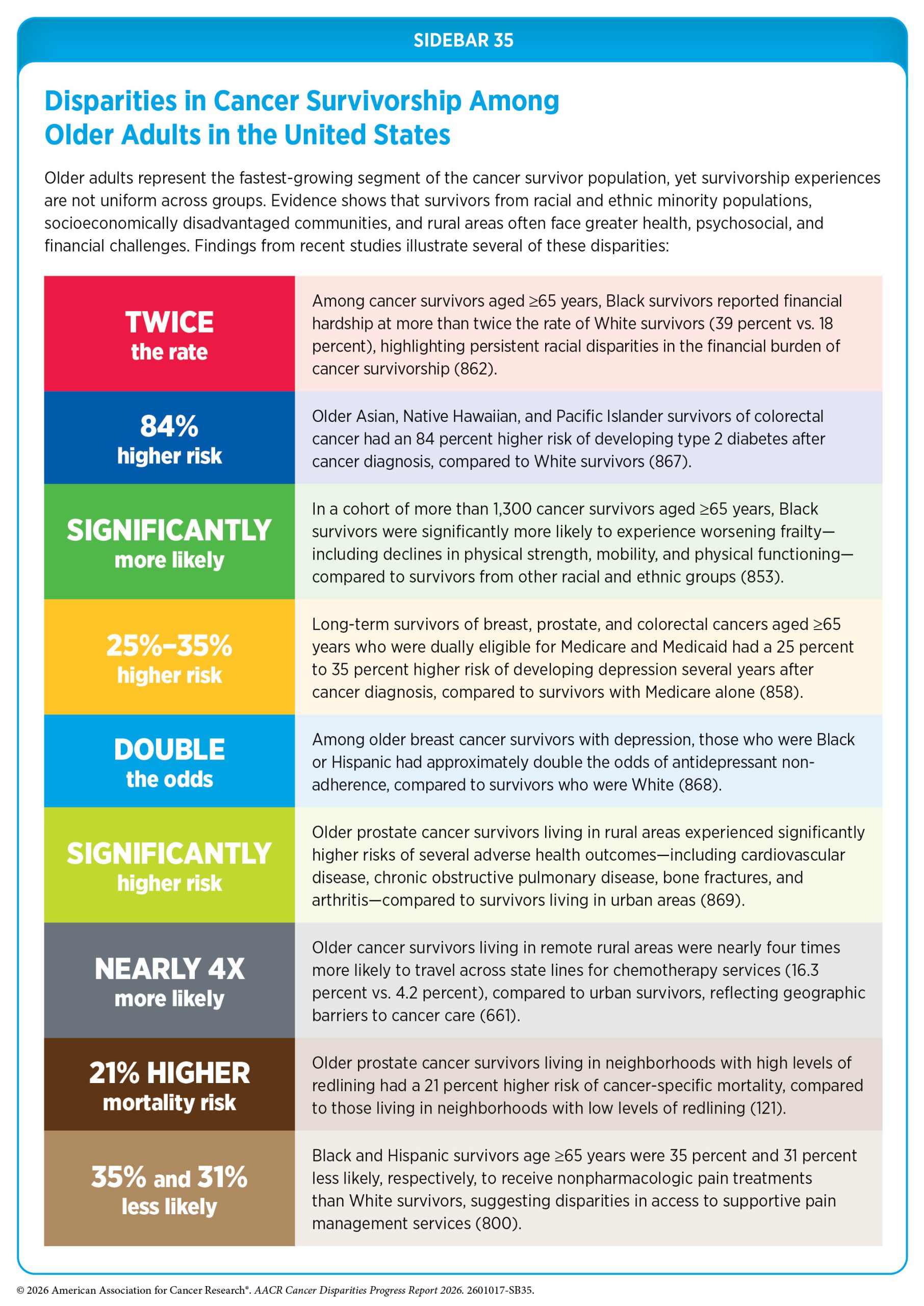
The challenges described above disproportionately affect older cancer survivors from medically underserved populations, including individuals from racial and ethnic minority groups, those with lower SES, and those living in rural or underserved communities (see Sidebar 35). These disparities often reflect the combined effects of age-related health vulnerabilities and broader SDOH (864)Dotan E, et al. (2024) Cancer Med, 13: e6790. . Comprehensive geriatric assessment has emerged as a valuable tool for improving the care of older adults with cancer. Geriatric assessment provides a multidimensional evaluation of health status that can identify vulnerabilities not captured by routine oncology assessments, including functional limitations, comorbidities, cognitive impairment, medication use, and social support needs (865)Loh KP, et al. (2024) ESMO Open, 9: 103657. (866)Magnuson A, et al. (2024) CA Cancer J Clin, 74: 496. . Integrating geriatric assessment with structured evaluation of unmet needs and other SDOH can help identify clinical and social risks that influence treatment tolerance and access to care, enabling a more personalized approach that may reduce disparities in survivorship outcomes in this population.
Unique Challenges Faced by Childhood, Adolescent, and Young Adult Cancer Survivors
Childhood cancer survivors include individuals diagnosed with cancer between the ages of 0 and 14 years, while adolescent and young adult (AYA) survivors include individuals diagnosed between ages 15 and 39 years. Advances in treatment have dramatically improved outcomes for childhood, adolescent, and young adult (CAYAs) cancer survivors, with 5-year survival rates now exceeding 85 percent, resulting in a rapidly growing population of long-term survivors (870)NCCR*Explorer: An interactive website for NCCR cancer statistics [Internet]. National Cancer Institute; 2025 Sep 24. [updated: 2026 Apr 30; cited 2026 May 11]. (871)Page LL, et al. (2025) J Natl Cancer Inst, 117: 529. .

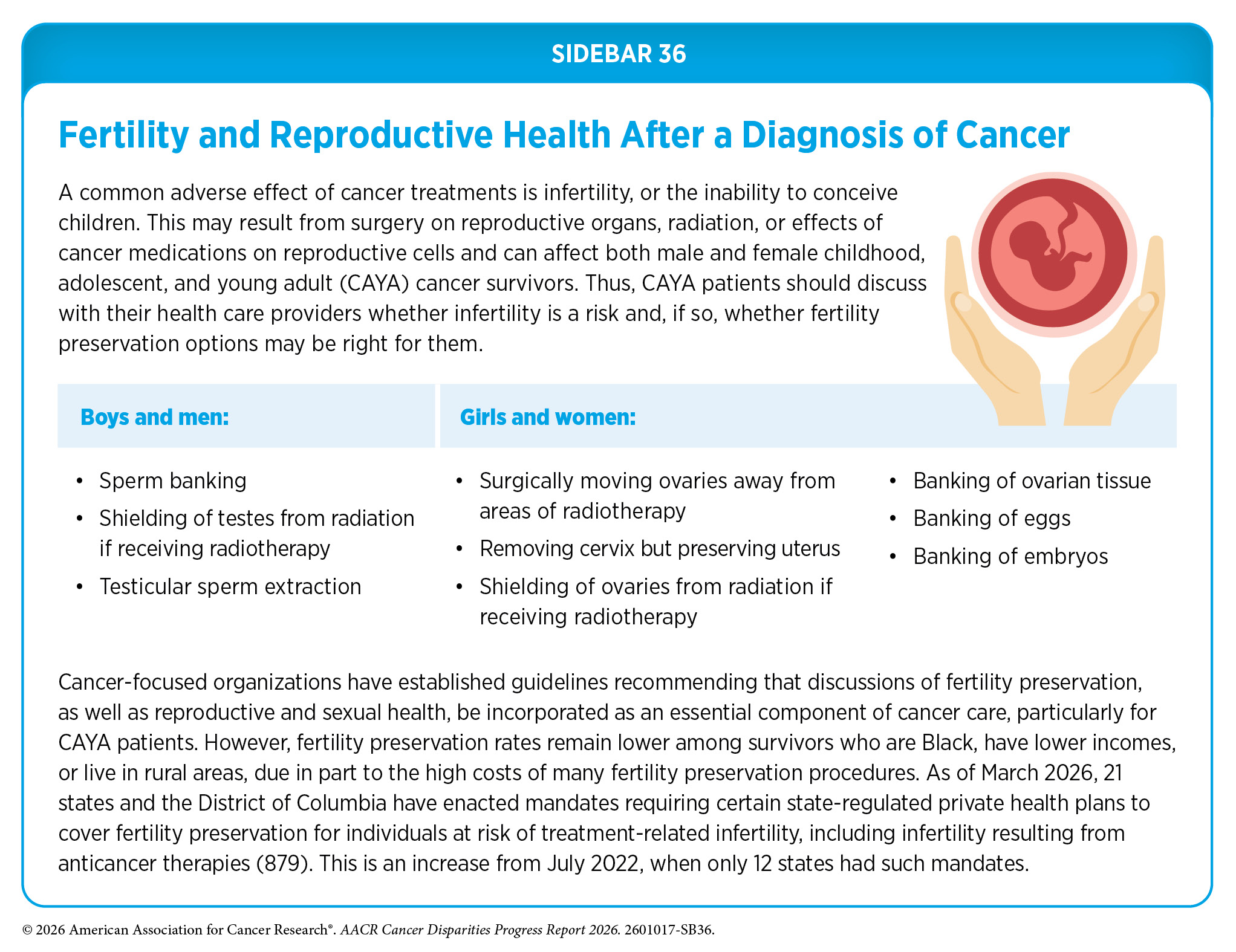
As detailed in the inaugural AACR Pediatric Cancer Progress Report 2025 (563)American Association for Cancer Research. AACR Pediatric Cancer Progress Report 2025. Accessed: March 17, 2026. , CAYA survivors remain at an increased risk for developing long-term health problems arising from their cancer or its treatments (872)Freyer DR, et al. (2026) J Cancer Surviv. . These late effects can affect multiple organ systems and include cardiovascular disease, endocrine dysfunction, neurocognitive impairment, and SPCs (873)Bhatia S, et al. (2023) JAMA, 330: 1175. (874)Hudson MM, et al. (2021) Pediatrics, 148. (875)Roganovic J (2025) World J Clin Cases, 13: 98000. . Infertility is another common adverse effect of CAYA cancer treatment and may result from surgery involving reproductive organs, radiation, or systemic therapies that damage reproductive cells (see Sidebar 36). Many CAYA survivors also experience accelerated biological aging, characterized by the premature onset of chronic, age-related conditions, such as for patients like Sebastián (Sebas) Casaus Natale. Accelerated biological aging is driven in part by treatment-related tissue damage and persistent inflammation (876)Bhandari R, et al. (2025) J Clin Oncol, 43: 2998. (877)Guida JL, et al. (2024) Nat Cancer, 5: 731. (878)Yeh JM, et al. (2025) JAMA Oncol, 11: 535. .
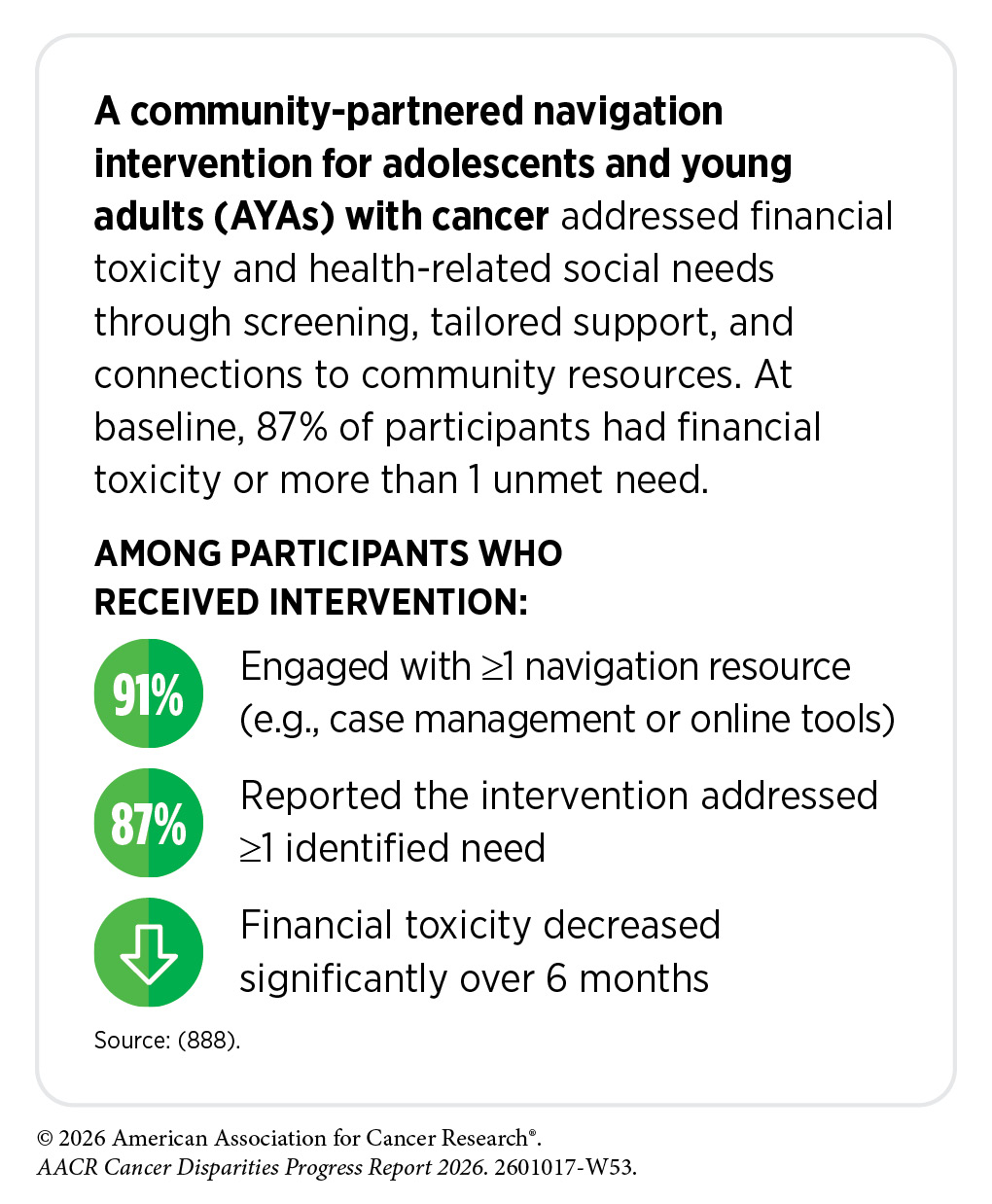
Beyond physical health challenges, CAYA survivors also experience a range of psychological and financial challenges that can persist well into adulthood. Research indicates that survivors of CAYA cancer are at increased risk of emotional distress, including anxiety, depression, and posttraumatic stress, compared to individuals without a history of cancer (880)Pizzo A, et al. (2024) JAMA Netw Open, 7: e2436144. (881)Zhang A, et al. (2025) JAMA Netw Open, 8: e2511430. . Psychological concerns particularly salient during this developmental stage—such as fear of cancer recurrence, body image concerns, sexual health challenges, and worries about social acceptance or stigma—can compound this burden (882)McGrady ME, et al. (2024) J Clin Oncol, 42: 707. (883)Yang M, et al. (2026) Qual Life Res, 35: 75. . Financial hardship is also common among CAYA cancer survivors, who are more likely to be uninsured or underinsured and often experience delays in completing education or entering the workforce due to ongoing health needs or treatment-related late effects (884)Hernadfoi MV, et al. (2024) JAMA Pediatr, 178: 548. (885)Kim Y, et al. (2025) Pediatr Blood Cancer, 72: e31980. (886)Kirchhoff AC, et al. (2024) J Natl Cancer Inst, 116: 1466. (887)Kirchhoff AC, et al. (2024) J Clin Oncol, 42: 642. . These disruptions can contribute to financial strain, reduced earning potential, and long-term economic vulnerability in adulthood.
Because of these complex and long-term health needs, survivorship care for CAYA cancer survivors requires lifelong, risk-based follow-up and coordinated care to monitor late effects, support transitions from pediatric to adult health systems, and address psychosocial needs (889)Berkman AM, et al. (2024) J Natl Cancer Inst, 116: 1417. (890)Ehrhardt MJ, et al. (2024) J Clin Oncol, 42: 743. (891)Wong CL, et al. (2024) BMJ Open, 14: e087343. . In recognition of these challenges, The Children’s Oncology Group Long-Term Follow-Up Guidelines for Survivors of Childhood, Adolescent, and Young Adult Cancers (COG LTFU Guidelines) provide a standardized, evidence-based framework for survivorship care for children, adolescents, and young adults with cancer (874)Hudson MM, et al. (2021) Pediatrics, 148. (892)DeVine A, et al. (2025) JAMA Oncol, 11: 544. .
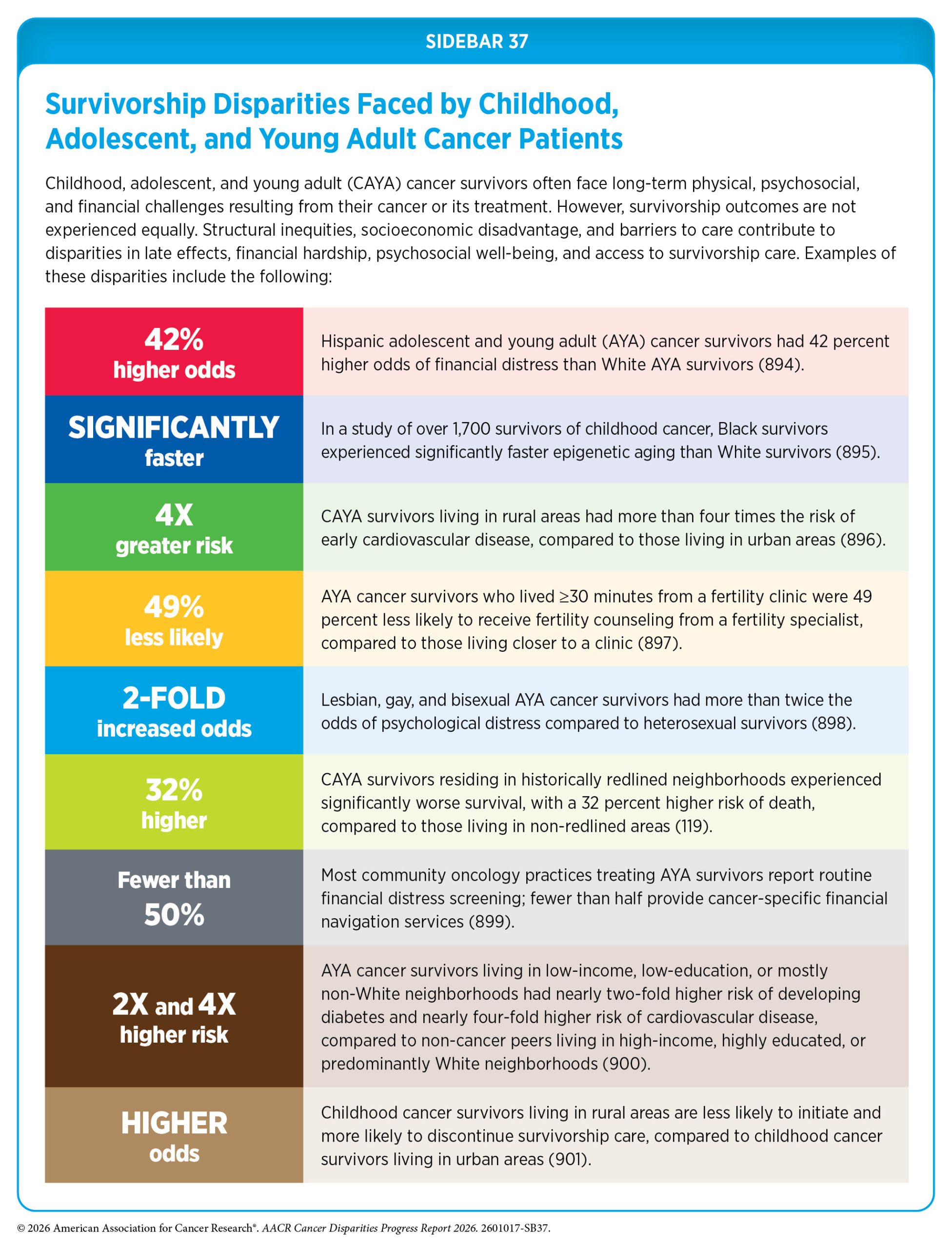
Although COG LTFU Guidelines exist, many CAYA survivors do not receive recommended follow-up care, reflecting barriers related to care coordination, access, and health system complexity (889)Berkman AM, et al. (2024) J Natl Cancer Inst, 116: 1417. (893)Milam J, et al. (2024) Pediatr Blood Cancer, 71: e31328. . These challenges may be further compounded for survivors from medically underserved populations, underscoring the importance of equitable access to survivorship care and support services to optimize long-term health and well-being (see Sidebar 37). Addressing these barriers is essential to improving survivorship care and improving long-term health and well-being among CAYA cancer survivors from all populations.
Strategies to Address Disparities in Cancer Survivorship

Disparities in survivorship outcomes are shaped by factors beyond clinical care, including psychosocial support, health behaviors, and access to supportive care services, as evident from the personal experiences of Pastor Rhonda Holbert and Freddie Muse Jr. A growing body of evidence suggests that interventions targeting these areas can improve patient outcomes and may help reduce disparities among medically underserved populations. The following sections highlight key domains of survivorship care, including promoting healthy behaviors, improving mental health, integrating supportive care, and supporting caregivers, all of which play an important role in addressing disparities across the survivorship continuum.
Promoting Healthy Behaviors
Maintaining a healthy lifestyle—through regular physical activity, a healthy diet, and eliminating alcohol and tobacco use—is one of the most effective strategies for reducing the risk of developing cancer and other chronic diseases (see Disparities in the Burden of Modifiable Behavioral Cancer Risk Factors). These behaviors can also improve health outcomes and quality of life for cancer survivors. A growing body of evidence indicates that healthy lifestyle behaviors are associated with improved outcomes among cancer survivors, including lower risk of cancer recurrence, reduced cardiovascular disease risk, improved mental health and quality of life, and longer survival.
Despite the well-documented benefits of healthy lifestyle behaviors for cancer survivorship, opportunities to engage in these behaviors are not equally distributed across populations. Cancer survivors from medically underserved populations often face structural, social, and economic barriers that limit their ability to adopt and sustain healthy behaviors. For example, Black and Hispanic survivors, as well as those with lower incomes, lower levels of acculturation, or no health insurance, are less likely to meet recommended physical activity guidelines than their more advantaged counterparts (903)Wojcik KM, et al. (2024) Cancer Epidemiol Biomarkers Prev, 33: 1610. (904)Zamora AN, et al. (2025) BMC Public Health, 25: 737. .
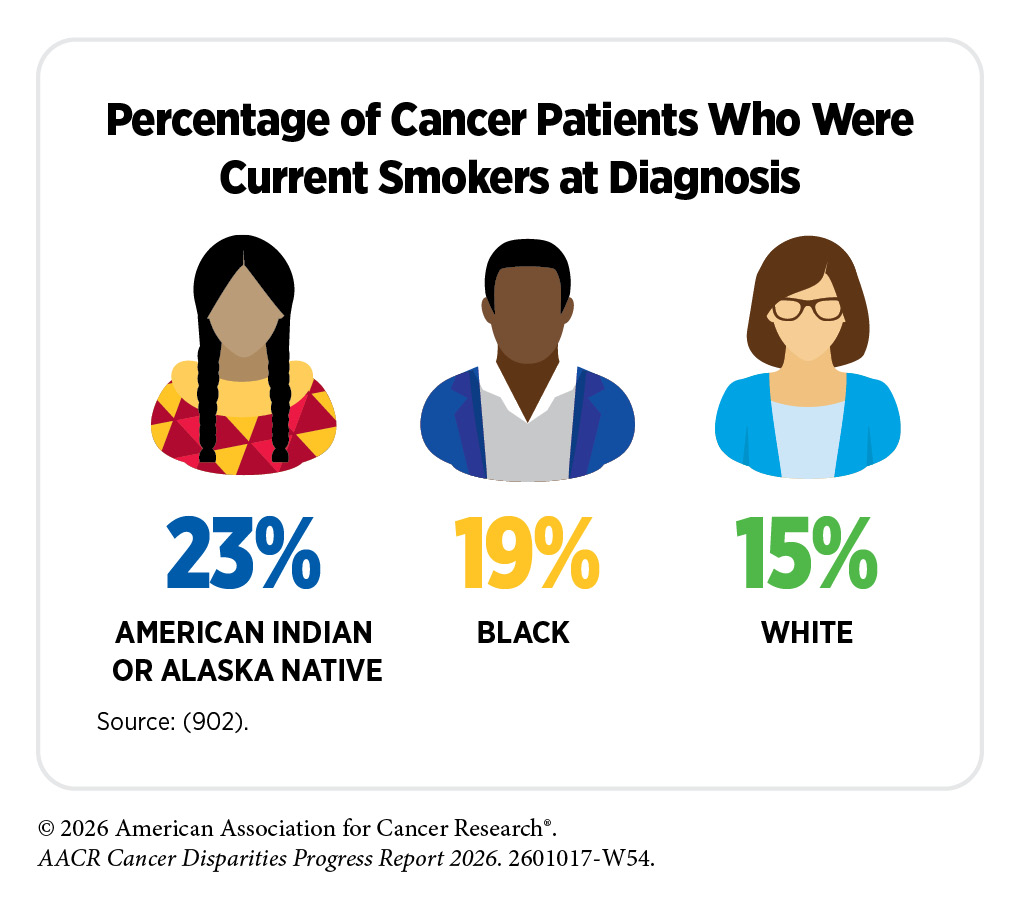
Disparities in tobacco and alcohol use are also evident among cancer survivors. In a study of more than 1.5 million individuals with cancer, nearly half reported a history of smoking, and approximately 15 percent were current smokers at the time of diagnosis (902)Caturegli G, et al. (2025) JAMA Oncol, 11: 564. . Current smoking was more common among AIAN (22.5 percent) and Black (18.9 percent) patients than among White patients (15.2 percent), and was more than twice as prevalent among those living in the lowest-income areas compared to those living in the highest-income areas (22.1 percent vs. 9.7 percent) (902)Caturegli G, et al. (2025) JAMA Oncol, 11: 564. . These disparities extend to SGM cancer survivors. In a recent study, approximately 15 percent of SGM survivors reported current tobacco use, with a similar proportion reporting current alcohol use (906)Robertson T, et al. (2025) Cancer Causes Control, 36: 1869. . These patterns were particularly pronounced among Black SGM survivors, who had more than double the odds of current tobacco and alcohol use compared to White counterparts. There were also differences by disability status: Compared to non-disabled survivors, disabled SGM survivors had lower odds of current alcohol use but higher odds of current tobacco use (906)Robertson T, et al. (2025) Cancer Causes Control, 36: 1869. . These differences likely reflect intersecting structural and social stressors, including experiences of discrimination and systemic inequities, that can adversely affect health behaviors.
Food insecurity, which is characterized by limited or uncertain access to adequate food, is a widespread issue that disproportionately affects medically underserved populations, including cancer survivors (see Diet). A recent study found that approximately 10 percent of cancer survivors report food insecurity, and those experiencing food insecurity have an increased risk of all-cause mortality when compared to their food-secure counterparts (907)Lin JC, et al. (2025) JAMA Health Forum, 6: e251381. . Cancer survivors living in food deserts—geographic areas with limited access to healthy and affordable food—face additional barriers to maintaining a healthy diet. In a study of endometrial cancer survivors in South Carolina, those with lower SES were more likely than higher-SES individuals to live in food deserts and travel greater distances to access nutritious food options (908)Patel KB, et al. (2024) Gynecol Oncol, 188: 8. .
Several emerging interventions aim to promote healthy behaviors among cancer survivors while addressing structural barriers that contribute to disparities. Community-based physical activity programs are one promising approach. For example, the Active Living After Cancer (ALAC) program is a 12-week group-based intervention delivered through community partners that provides behavioral skills training and physical activity support for cancer survivors and their caregivers. Studies of medically underserved survivors have shown that participation in ALAC substantially increases the proportion of survivors meeting recommended physical activity guidelines and improves physical functioning and quality of life (909)Lee CY, et al. (2025) J Cancer Surviv, 19: 1861. (910)Mama SK, et al. (2024) J Natl Cancer Inst, 116: 1333. . The program’s community-based delivery model, which partners with local organizations serving underserved populations, demonstrates the potential for scalable approaches to promote physical activity and improve survivorship outcomes.
Telehealth-based exercise interventions represent a promising strategy to expand access to exercise programs, particularly for cancer survivors living in rural areas. In one study, a 12-week telehealth exercise program that incorporated remote supervision, personalized exercise prescriptions, and symptom monitoring was feasible and resulted in improvements in cancer-related fatigue (911)Marker RJ, et al. (2025) JMIR Cancer, 11: e59478. .
Interventions that address barriers to accessing healthy foods are also emerging as promising strategies to support healthy behaviors among cancer survivors. For example, the Cardiovascular Health Equity through Food (CHEF) program is an intervention designed for childhood cancer survivors experiencing food insecurity (912)Aziz-Bose R, et al. (2025) J Cancer Surviv. . The program provides home-delivered meal kits alongside assistance with enrollment in federal nutrition programs, such as the Supplemental Nutrition Assistance Program (SNAP) and Women, Infants, and Children (WIC). Early evaluation of this intervention found high levels of acceptability and engagement among participating families and suggests that strategies that directly address food insecurity may help improve diet quality and support long-term health among childhood cancer survivors (912)Aziz-Bose R, et al. (2025) J Cancer Surviv. .
Interventions to support smoking cessation represent another critical component of survivorship care. Smoking cessation after a cancer diagnosis is associated with substantial improvements in survival. In a large cohort of more than 13,000 patients with cancer, those who continued smoking had nearly twice the risk of death compared to those who quit within 6 months of diagnosis (913)Tohmasi S, et al. (2025) J Natl Compr Canc Netw, 23. . Similarly, a recent study found that participation in structured smoking cessation programs that included counseling and pharmacotherapy was associated with significant improvements in overall survival, particularly when initiated soon after diagnosis (914)Cinciripini PM, et al. (2024) JAMA Oncol, 10: 1689. . These findings underscore the importance of integrating evidence-based tobacco cessation interventions into oncology care, particularly for populations disproportionately affected by tobacco use, and the need for tailored approaches to reduce disparities in cessation support.
Improving Mental Health

Given the substantial psychological burden experienced by many cancer survivors, strategies to support mental well-being are an essential component of survivorship care, as emphasized in the cancer journey of Mikey Shock. Several approaches—including counseling, mind–body interventions, support groups, physical activity programs, and routine screening for mental health concerns—have been shown to improve psychological outcomes and quality of life among cancer survivors (915)Andersen BL, et al. (2023) J Clin Oncol, 41: 3426. . However, survivors from underserved populations often face significant barriers to accessing these services, including financial constraints, stigma surrounding mental health care, and geographic barriers that limit access to psychosocial support.
To address these challenges, researchers and clinicians are exploring models that integrate mental health services directly into oncology care. One such approach is the collaborative care model, a team-based framework in which behavioral health services are embedded within routine cancer care and delivered through coordinated collaboration among oncologists, social workers, mental health specialists, and care managers (916)Li M, et al. (2017) Psychooncology, 26: 573. . Collaborative care models typically incorporate screening for psychological distress, monitoring of symptoms, and stepped treatment strategies in which counseling, medication management, and other supportive services are adjusted based on patients’ needs. In addition to improving psychological outcomes, collaborative care models are designed to address fragmentation between oncology and mental health systems, reduce barriers to care, and strengthen communication across providers (916)Li M, et al. (2017) Psychooncology, 26: 573. (917)Irwin KE, et al. (2022) Contemp Clin Trials, 123: 106975. (918)Steel JL, et al. (2024) Lancet, 403: 1351. .
Growing evidence suggests that collaborative care interventions not only improve mental health and quality of life among cancer survivors, but also expand access to psychosocial support for populations facing barriers to mental health services (917)Irwin KE, et al. (2022) Contemp Clin Trials, 123: 106975. (918)Steel JL, et al. (2024) Lancet, 403: 1351. (919)Aburizik A, et al. (2023) Psychooncology, 32: 1675. . For example, a collaborative depression care program designed to meet the needs of underserved cancer patients included bilingual care managers who worked with oncology teams to monitor symptoms, provide counseling, and coordinate medication management when needed (920)Price S, et al. (2024) J Psychosoc Oncol, 42: 90. . The program demonstrated strong engagement among a socioeconomically and ethnically diverse population of cancer survivors, and was associated with improvements in depression, anxiety, social isolation, and suicidal thoughts.
Mental health interventions should also consider the cultural and social factors that influence how individuals experience and cope with cancer. Cultural values often shape how people interpret illness, communicate with health care providers, and seek emotional and social support, and these factors can strongly influence engagement with mental health services. Interventions that incorporate culturally relevant values, beliefs, and social contexts may improve participation and effectiveness among populations that have historically been underrepresented in psycho-oncology research. A systematic review of psychosocial and behavioral interventions for medically underserved cancer populations found that culturally adapted interventions were associated with improvements in quality of life, distress, and anxiety (921)Llave K, et al. (2024) Int J Behav Med, 31: 848. . These interventions often incorporate family-centered approaches, culturally relevant coping strategies, and partnerships with community-based organizations to improve accessibility and trust. As discussions of mental health continue to evolve, policymakers like Congressman Troy A. Carter (D-LA) are working to address the needs of men’s mental health, to address the potential stigma around health care.
Integrating Supportive Care
Supportive care aims to prevent and manage the adverse effects of cancer and its treatment across the entire cancer care continuum, from diagnosis through survivorship and end-of-life care (922)Olver I, et al. (2020) Support Care Cancer, 28: 3467. . Palliative care is a component of supportive care that focuses on improving quality of life for individuals with cancer and their families (923)Sanders JJ, et al. (2024) J Clin Oncol, 42: 2336. (924)Taylor A, et al. (2025) Clin Med (Lond), 25: 100487. . The goal of palliative care is to prevent or treat symptoms of disease and side effects of treatment as early as possible, while also addressing related psychological, social, and spiritual challenges. Importantly, palliative care is appropriate at any stage of disease and can be provided alongside curative treatment. Evidence suggests that palliative care is most effective when delivered by multidisciplinary teams comprising physicians, nurses, psychologists, nutritionists, pharmacists, social workers, chaplains, and other health care professionals (923)Sanders JJ, et al. (2024) J Clin Oncol, 42: 2336. (925)Hart NH, et al. (2024) JCO Oncol Pract, 20: 1160. . Integrating palliative care early in the treatment trajectory can improve quality of life, reduce symptom burden, and facilitate communication about treatment goals and end-of-life preferences (926)Petrillo LA, et al. (2024) Am Soc Clin Oncol Educ Book, 44: e100038. .
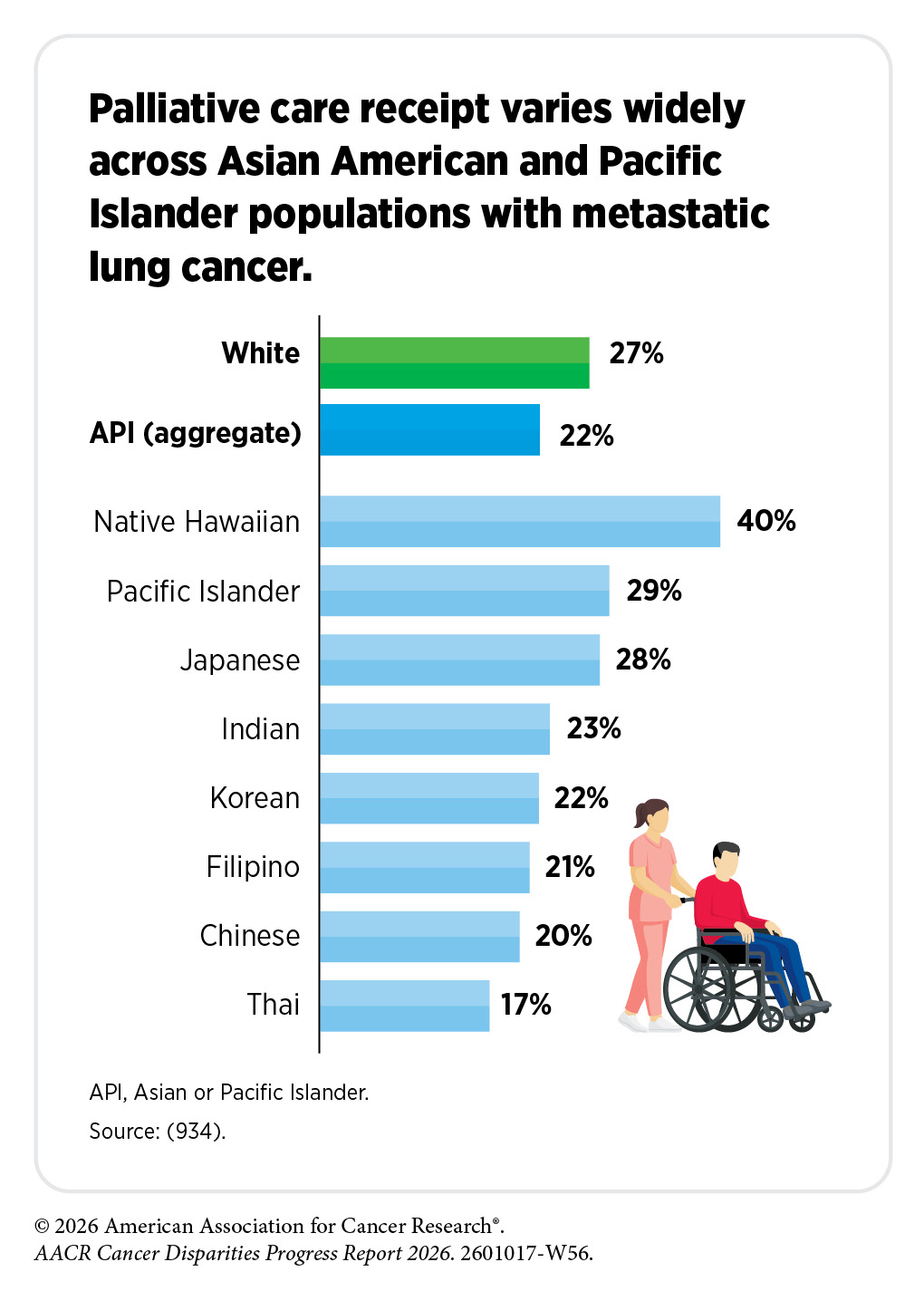
Despite the well-documented benefits of supportive care, access to and utilization of these services remain uneven across populations. Survivors living in rural areas and those with lower incomes are less likely to receive palliative care than their urban and higher-income counterparts (927)Freeman JQ, et al. (2024) J Rural Health, 40: 602. (928)Iqbal J, et al. (2024) JAMA Netw Open, 7: e240503. (929)Osakwe ZT, et al. (2024) Am J Hosp Palliat Care, 41: 309. (930)Ramkumar N, et al. (2023) J Rural Health, 39: 557. (931)Whitman J, et al. (2026) Am J Hosp Palliat Care: 10499091261425959. . Similar disparities exist across racial and ethnic groups, with Black, Asian, and Hispanic survivors receiving palliative care less often than White survivors (932)Freeman JQ, et al. (2024) J Palliat Med, 27: 763. . Disparities also exist in the timing of supportive care delivery, with racial and ethnic minority patients often receiving palliative care later in the course of illness, which may limit the potential benefits of these services (933)Khayal IS, et al. (2025) Lancet Reg Health Am, 47: 101135. .
Supportive care also includes hospice services. In contrast to palliative care, hospice refers to care provided near the end of life, when treatment is no longer aimed at cure and the focus shifts to comfort, symptom management, caregiver support, and alignment with patients’ end-of-life priorities (924)Taylor A, et al. (2025) Clin Med (Lond), 25: 100487. (935)Currow DC, et al. (2020) J Clin Oncol, 38: 937. . Disparities in palliative care also extend to hospice and end-of-life care. For example, patients with cancer living in rural areas have lower odds of hospice enrollment than those in metropolitan areas, reflecting structural barriers such as limited provider availability and greater travel distances to care (585)Chua AV, Jr., et al. (2025) JCO Oncol Pract, 21: 408. (927)Freeman JQ, et al. (2024) J Rural Health, 40: 602. (928)Iqbal J, et al. (2024) JAMA Netw Open, 7: e240503. (929)Osakwe ZT, et al. (2024) Am J Hosp Palliat Care, 41: 309. (930)Ramkumar N, et al. (2023) J Rural Health, 39: 557. (931)Whitman J, et al. (2026) Am J Hosp Palliat Care: 10499091261425959. . Compared to White patients, Black, Hispanic, API, and AIAN patients are less likely to enroll in hospice and are more likely to experience high-intensity or aggressive care near the end of life, including repeated emergency department visits, intensive care unit admission, mechanical ventilation, or cardiopulmonary resuscitation (936)Abdallah M, et al. (2024) J Geriatr Oncol, 15: 101810. .
Racial and ethnic minority patients are also less likely to complete advance directives or engage in advance care planning (ACP), further contributing to disparities in end-of-life care (937)Bazargan M, et al. (2021) Am J Hosp Palliat Care, 38: 688. (938)Jawed A, et al. (2024) Ann Palliat Med, 13: 309. (939)Lenko RA, et al. (2024) J Am Geriatr Soc, 72: 2412. . Medical mistrust rooted in historical and ongoing experiences of discrimination and disparities in the quality of end-of-life communication contribute to less informed decision-making (938)Jawed A, et al. (2024) Ann Palliat Med, 13: 309. . For certain groups, cultural beliefs and stigma surrounding cancer and death may further discourage conversations about advance care planning or end-of-life care (940). Evidence suggests that patient–provider racial and ethnic concordance improves communication and engagement in advance care planning. For example, Black patients are more likely to have ACP conversations when cared for by a Black physician, which may help address disparities in ACP completion (941)Carter B, et al. (2026) J Gen Intern Med. .
At the structural and systems level, unequal access to hospice care, geographic and financial barriers, and variation in care quality in hospitals that disproportionately serve racial and ethnic minority populations further contribute to disparities in end-of-life care (942)Weiss M, et al. (2025) Am Soc Clin Oncol Educ Book, 45: e472842. (943)Fariman S, et al. (2026) Am J Hosp Palliat Care: 10499091251414863. (944)Cole AP, et al. (2019) JAMA Netw Open, 2: e187633. . Collectively, disparities in hospice and end-of-life care among racial and ethnic minority populations reflect differences in awareness, access, communication, and quality of care, not patient preference, underscoring the need for culturally tailored interventions to ensure equitable end-of-life experiences.
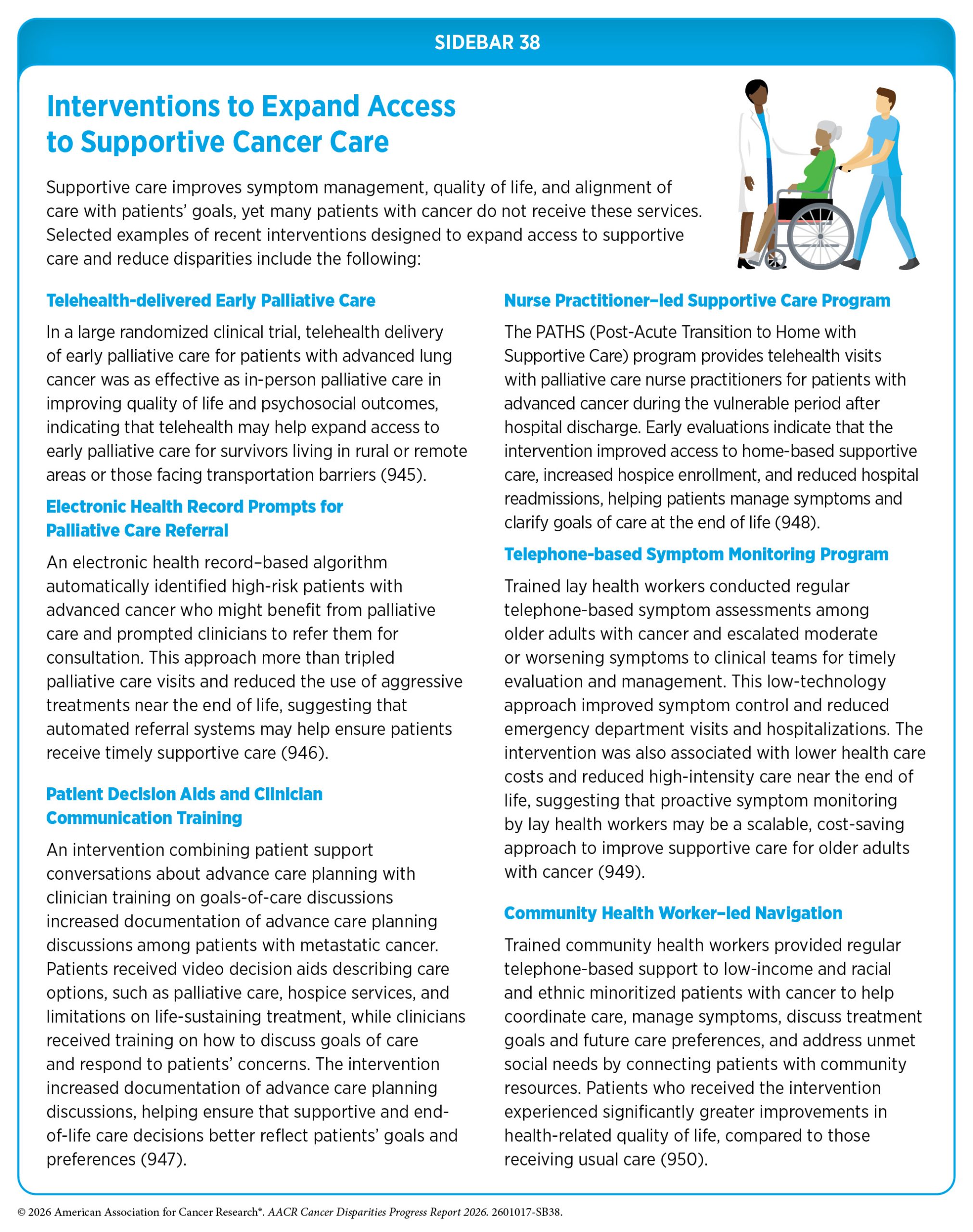
Several innovative care delivery models have emerged to expand access to supportive care services for populations that have historically faced barriers to care. These approaches include telehealth-based palliative care programs, community health worker– and navigator-led models, and communication tools designed to support advance care planning and discussions about treatment preferences. Early evidence suggests these strategies can improve symptom management, strengthen communication about goals of care, and increase timely use of supportive services (see Sidebar 38).
Supporting Caregivers
Caregivers comprise family members and/or friends who help patients with long-term chronic illness and manage any and all aspects of their care. In 2025, an estimated 63 million US adults provided care for another person, representing nearly one-quarter of all adults in the United States (951)AARP. Caregiving in the US. Accessed: March 30, 2025. . It is further estimated that more than four million of these caregivers were supporting an adult with cancer. Cancer caregivers help patients across the cancer care continuum, including managing medications, coordinating medical appointments, arranging transportation, assisting with clinical decision-making, and providing emotional and financial support. These responsibilities can place considerable strain on caregivers, often resulting in emotional, physical, and financial burdens that negatively affect their quality of life. Importantly, the same structural and social drivers of health that affect cancer survivors also shape the experiences and challenges faced by caregivers.
Cancer caregivers from racial and ethnic minority groups often experience greater caregiving-related burdens than caregivers from other population groups. For example, studies have shown that Black and Hispanic caregivers provide more hours of care each week and perform a greater number of caregiving tasks than White caregivers (952)Fenton A, et al. (2022) Support Care Cancer, 30: 9625. (953)Tan KR, et al. (2023) Curr Oncol Rep, 25: 803. . Furthermore, Black and Hispanic caregivers are more likely than White caregivers to serve as sole unpaid caregivers, provide more intensive medical and nursing care, and experience greater financial strain and employment disruptions related to caregiving responsibilities (952)Fenton A, et al. (2022) Support Care Cancer, 30: 9625. (953)Tan KR, et al. (2023) Curr Oncol Rep, 25: 803. (954)Love B, et al. (2026) JMIR Cancer, 12: e76266. . These challenges often occur within broader structural and social contexts that are shaped by long-standing disparities and systemic injustices, which may contribute to heightened stress, financial hardship, and barriers to obtaining caregiver support services (953)Tan KR, et al. (2023) Curr Oncol Rep, 25: 803. (954)Love B, et al. (2026) JMIR Cancer, 12: e76266. . At the same time, strong family networks, cultural values around family caregiving, and faith-or community-based support systems serve as important sources of resilience that help sustain caregiving within many racial and ethnic communities (953)Tan KR, et al. (2023) Curr Oncol Rep, 25: 803. .
For caregivers from SGM populations, the demands of cancer caregiving are often compounded by experiences of minority stress, including stigma, discrimination, invisibility, and fear of exclusion within health care settings. Caregiving responsibilities can lead to substantial financial hardship for SGM caregivers, particularly when caregiving-related employment disruptions intersect with anti-SGM stigma and workplace discrimination (845)Waters AR, et al. (2025) Cancer Control, 32: 10732748251351105. . Higher levels of anti-SGM stigma are also associated with worse mental and physical health outcomes among caregivers, including higher levels of anxiety, depression, fatigue, and sleep disturbance (955)Allison K, et al. (2024) BMC Cancer, 24: 36. (956)Waters AR, et al. (2026) Psychooncology, 35: e70379. . At the same time, health care systems often fail to recognize or affirm SGM caregivers, who report experiences of invisibility in clinical interactions, heteronormative assumptions about relationships, and uncertainty about whether their roles will be acknowledged in care discussions and decision-making (683)Insalaco ME, et al. (2026) Oncologist, 31. . These challenges are further compounded by limited availability of culturally competent, caregiver-inclusive support resources, leaving many SGM caregivers without services that reflect their identities, relationships, and caregiving needs (953)Tan KR, et al. (2023) Curr Oncol Rep, 25: 803. .
Cancer survivors who provide care to others represent a particularly vulnerable population, with substantial health and psychosocial support needs. A national analysis estimated that nearly four million cancer survivors in the United States also serve as informal caregivers to family members or friends (957)Wang Q, et al. (2024) J Cancer Surviv, 18: 553. . Evidence suggests that survivors who also serve as caregivers experience worse physical and mental health outcomes than caregivers without a history of cancer, including a higher likelihood of depression, sleep disturbances, and physical inactivity (957)Wang Q, et al. (2024) J Cancer Surviv, 18: 553. . These individuals are also more likely to report unmet social needs, including food, housing, or transportation, compared to survivors who were not caregivers, suggesting that caregiving responsibilities may compound the social and economic burdens already faced by cancer survivors (958)Wang Q, et al. (2025) JCO Oncol Pract: OP2500388. . Despite reporting higher levels of unmet social needs, many survivors with caregiving responsibilities report that they do not feel comfortable discussing these challenges with health care providers, highlighting the need for more proactive screening for unmet social needs and targeted support for this vulnerable population (958)Wang Q, et al. (2025) JCO Oncol Pract: OP2500388. .
Burdens associated with cancer caregiving are shaped by structural and social factors and are not experienced equally across populations. For example, Hispanic cancer caregivers report significantly greater caregiving burden than their White counterparts, particularly related to financial strain, family responsibilities, and time demands associated with caregiving (959)Badger T, et al. (2024) J Psychosoc Oncol, 42: 333. . Evidence also suggests that Black caregivers are more likely than White caregivers to serve as sole unpaid caregivers, provide more hours of care each week, and receive less external support, while also facing greater financial strain and employment disruptions. Cultural and historical factors such as medical mistrust and stigma surrounding mental health may further exacerbate these caregiving challenges.
Efforts to reduce disparities in cancer outcomes must also address the needs of caregivers through coordinated strategies that integrate caregiver support into oncology care, expand access to culturally appropriate resources, and implement policies that reduce financial and structural burdens.
Future Directions in Cancer Survivorship
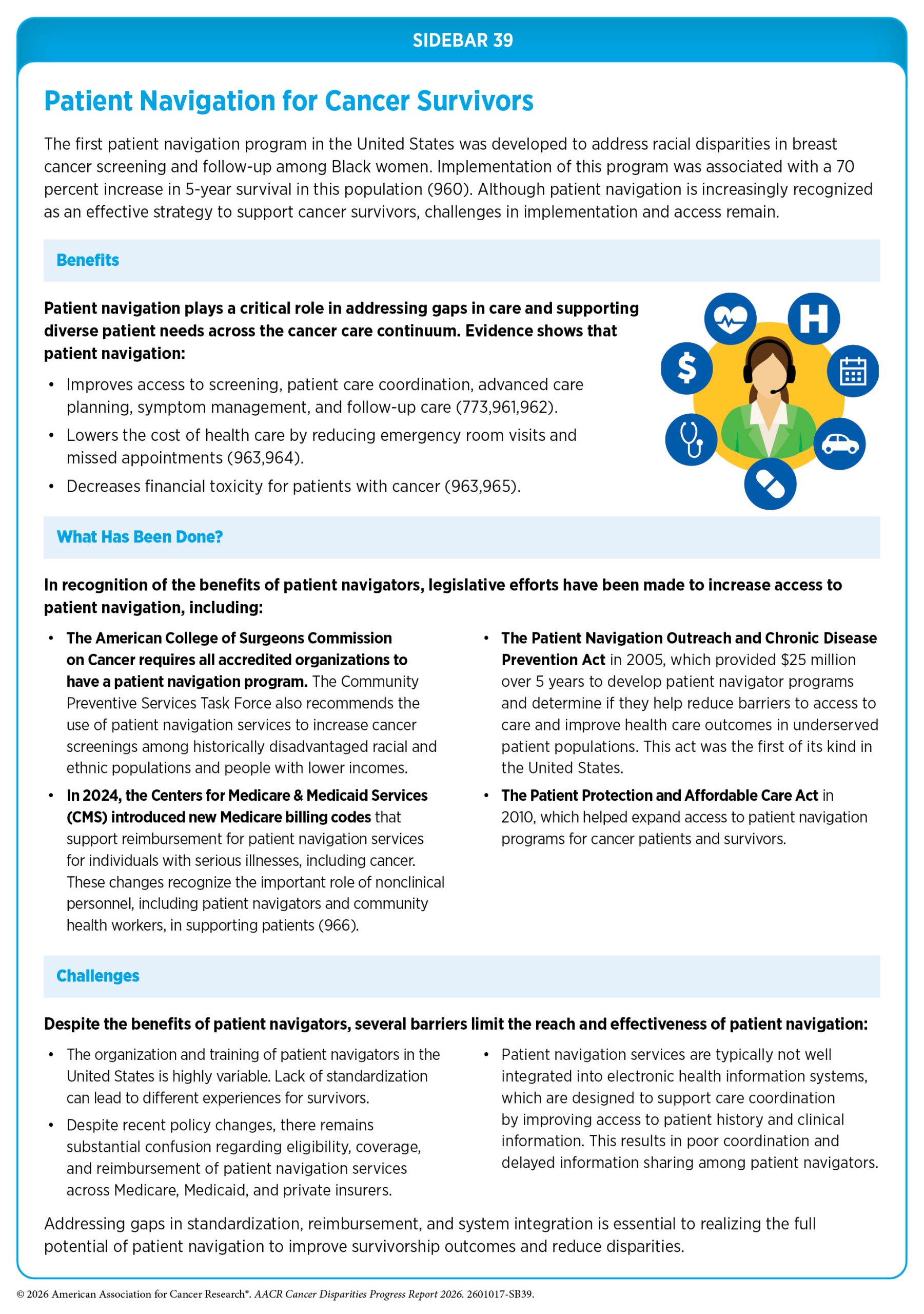
Survivorship care may be most effective when a designated individual or a team of people helps a cancer patient or survivor gain access to the resources they need. Patient navigators are individuals dedicated to assisting patients with cancer, survivors, family members, and caregivers by helping them navigate complex health care systems and access timely, high-quality care (see Sidebar 39). Navigation programs are designed to address structural barriers that delay treatment or limit access to supportive services, including financial hardship, transportation challenges, language barriers, and difficulties coordinating care across providers. These services may be particularly important for individuals facing structural barriers to survivorship care, including those from racial and ethnic minority groups, SGM populations, rural communities, and those with limited financial resources or low health literacy.
A growing body of evidence shows that patient navigation improves multiple aspects of cancer care delivery, particularly for medically underserved populations. Community-focused navigation programs can increase trust in health care providers, reduce system-level barriers, and improve continuity of care (962)Ver Hoeve ES, et al. (2024) BMC Health Serv Res, 24: 550. . One such program, the Integrated Cancer Care Access Network (ICCAN), is a multidisciplinary initiative that provides underserved cancer patients with one-on-one, culturally and linguistically tailored navigation and assistance with essential needs, such as food, housing, and financial support. Researchers have found that patients who received these services experienced significantly higher treatment completion rates and greater improvements in quality of life, depression, and stress, compared to those receiving standard care (778)Gany F, et al. (2025) J Natl Compr Canc Netw, 23. .
However, patient navigation alone may be insufficient to address disparities in cancer care delivery for some populations. AIAN patients with cancer, for example, often receive care across the Indian Health Service, tribal health programs, and community-based clinics that may lack comprehensive oncology services, necessitating referral to external cancer centers (967)Daley MP, et al. (2026) Oncologist, 31. (968)Warne D, et al. (2025) Front Health Serv, 5: 1469501. . The involvement of multiple providers across these systems, combined with limited integration and communication gaps, can contribute to fragmented care, treatment delays, and worse outcomes (967)Daley MP, et al. (2026) Oncologist, 31. (968)Warne D, et al. (2025) Front Health Serv, 5: 1469501. (969)Janitz AE, et al. (2025) N Engl J Med, 393: 940. . Innovative care coordination models that incorporate structured, interdisciplinary communication have shown promise in addressing these gaps. One such approach involves regular “huddles,” or team-based meetings, that bring together oncology providers, care coordinators, patient navigators, and referring clinicians to review care plans, address barriers to care, and align treatment decisions (967)Daley MP, et al. (2026) Oncologist, 31. . These models facilitate real-time information sharing and improve care continuity, particularly for patients navigating complex referral networks or multiple care systems.
Survivorship care plans (SCPs) are another important tool for improving care coordination. These plans typically include a summary of the patient’s diagnosis and treatment, along with guidance for follow-up care, including recommended health screenings, surveillance for recurrence and SPCs, and management of long-term and late effects. By facilitating communication among patients, oncologists, and primary care providers, SCPs help ensure coordinated, continuous care as patients transition from active treatment to long-term survivorship.
SCPs have been shown to improve several aspects of survivorship care delivery and patient outcomes. Survivors who receive SCPs are more likely to adhere to recommended surveillance and screening for second cancers and other late effects (970)Yan AP, et al. (2020) J Clin Oncol, 38: 1711. . SCPs can also improve care coordination between oncology and primary care providers, increase survivors’ knowledge of their cancer history and follow-up needs, and enhance self-efficacy and confidence in managing survivorship care (971)Tarver WL, et al. (2025) J Cancer Surviv, 19: 1956. . These improvements in care delivery and patient engagement are increasingly recognized as important mechanisms through which SCPs may influence longer-term outcomes. A recent study found that SCP receipt was associated with a 38 percent lower risk of death among childhood cancer survivors (972)Ji X, et al. (2026) J Natl Cancer Inst, 118: 85. . Despite these benefits, disparities in the receipt and use of SCPs persist, with medically underserved populations, including racial and ethnic minority groups, rural residents, and low-income populations less likely to receive SCPs and more likely to report unmet survivorship needs compared to their more advantaged counterparts (971)Tarver WL, et al. (2025) J Cancer Surviv, 19: 1956. .
Persistent disparities in survivorship outcomes are driven in part by fragmented and variable survivorship care delivery across health systems. This lack of coordination can exacerbate disparities among medically underserved populations. To address these challenges, NCI and the US Department of Veterans Affairs developed the first National Standards for Cancer Survivorship Care to guide health systems in delivering high-quality survivorship services (973)Mollica MA, et al. (2024) J Cancer Surviv, 18: 1190. . These standards outline key components across health system policy, care delivery processes, and evaluation, with an emphasis on coordinated, patient-centered care.
At the health system policy level, the standards call for the establishment of formal survivorship programs supported by multidisciplinary teams, clear leadership, and sustainable funding. They also call for policies that ensure support services, including patient navigation and interpretation services, are provided based on survivors’ needs, particularly for individuals from diverse and underserved populations (973)Mollica MA, et al. (2024) J Cancer Surviv, 18: 1190. . At the care delivery level, the standards emphasize routine assessment and management of physical late effects, psychosocial challenges, and health-related social needs, such as financial hardship, employment disruptions, and barriers to insurance coverage, all of which disproportionately affect underserved populations. The standards also highlight the importance of coordinated care across providers and settings, including transitions from oncology to primary care and from pediatric to adult services, to minimize loss to follow-up. Expanding telehealth and referral pathways may help improve access to survivorship services and support care coordination, particularly for patients in rural or remote areas. At the evaluation level, the standards underscore the importance of accountability through ongoing assessment of survivorship outcomes. Routine collection of data on patient-reported outcomes, quality-of-life measures, care experiences, and patterns of care use can help identify populations at risk for poor outcomes and guide targeted strategies to improve survivorship care (973)Mollica MA, et al. (2024) J Cancer Surviv, 18: 1190. .
Together, the National Standards for Cancer Survivorship Care provide a comprehensive framework for organizing services and evaluating their impact, offering health systems a roadmap to strengthen survivorship care delivery, expand access to survivorship services, and ensure that all survivors—regardless of race, ethnicity, sexual orientation, gender identity, SES, or geographic location—receive coordinated, patient-centered support across the cancer care continuum.
Next Section: Disparities in the Cancer Training Pathway and Cancer Research and Care Workforce Previous Section: Disparities in Clinical Research and Cancer Treatment
{kind=link}