Understanding Cancer Development in the Context of Cancer Disparities
In this section, you will learn:
- Cancer is a collection of diseases in which some of the body’s cells acquire changes that cause them to grow uncontrollably, resist cell death, and spread to other parts of the body.
- Broader social, environmental, and structural conditions can influence biology and contribute to differences in cancer risk, tumor behavior, and treatment response across population groups.
- Increasing the representation of diverse populations in cancer research models, datasets, and biorepositories is essential to ensure discoveries accurately reflect and benefit all populations.
- Cancer development is driven by complex interactions among factors inside the cell, including inherited and/or acquired genetic alterations, RNA variations, protein modifications, and epigenetic changes, and outside the cell, including the blood, lymphatic, and immune systems, microbiome, and tumor microenvironment.
Advances in understanding cancer biology are enabling precision medicine approaches, but translating these discoveries into improved outcomes for all patients requires integrating biological, social, and environmental data and ensuring fair access for all populations.
Contents
Decades of medical research have provided insights into the underpinnings of cancer development. Knowledge gleaned from this research shows that cancer is not a single disease but a collection of diseases that can affect nearly any part of the body. Precise molecular mechanisms control normal cell growth and division, which are required for development, regeneration, and overall healthy tissue and organ functions. In cancer, these mechanisms go awry, enabling cells to multiply uncontrollably, resist cell death, and spread to other parts of the body.
Throughout the course of cancer development, abnormal or damaged cells acquire distinct traits—known as the “hallmarks of cancer”—that set them apart from normal cells. These hallmarks include the ability of cancer cells to multiply unchecked; ignore signals that stop normal cells from dividing; acquire changes that make their genetic code unstable; increase the supply of nutrients and oxygen to tumors; utilize different metabolic strategies to sustain rapid growth; evade the immune system, which typically eliminates abnormal or damaged cells; and leave the tissue of origin and spread to other organs (186)Hanahan D (2026) Cell. . Cancer that has spread to other parts of the body, which is called metastatic disease, is the main cause of most cancer-related deaths.
It is important to note that many biological, behavioral, and environmental factors influence cancer development. Research has uncovered differences in genetic variation and tumor biology observed among individuals from different population groups that may contribute to the higher incidence or aggressiveness of certain cancers and differential responses to therapy (187)Amuzu S, et al. (2025) Nat Genet, 57: 2655. (188)Luo M, et al. (2025) Cancer Discov, 15: 511. .
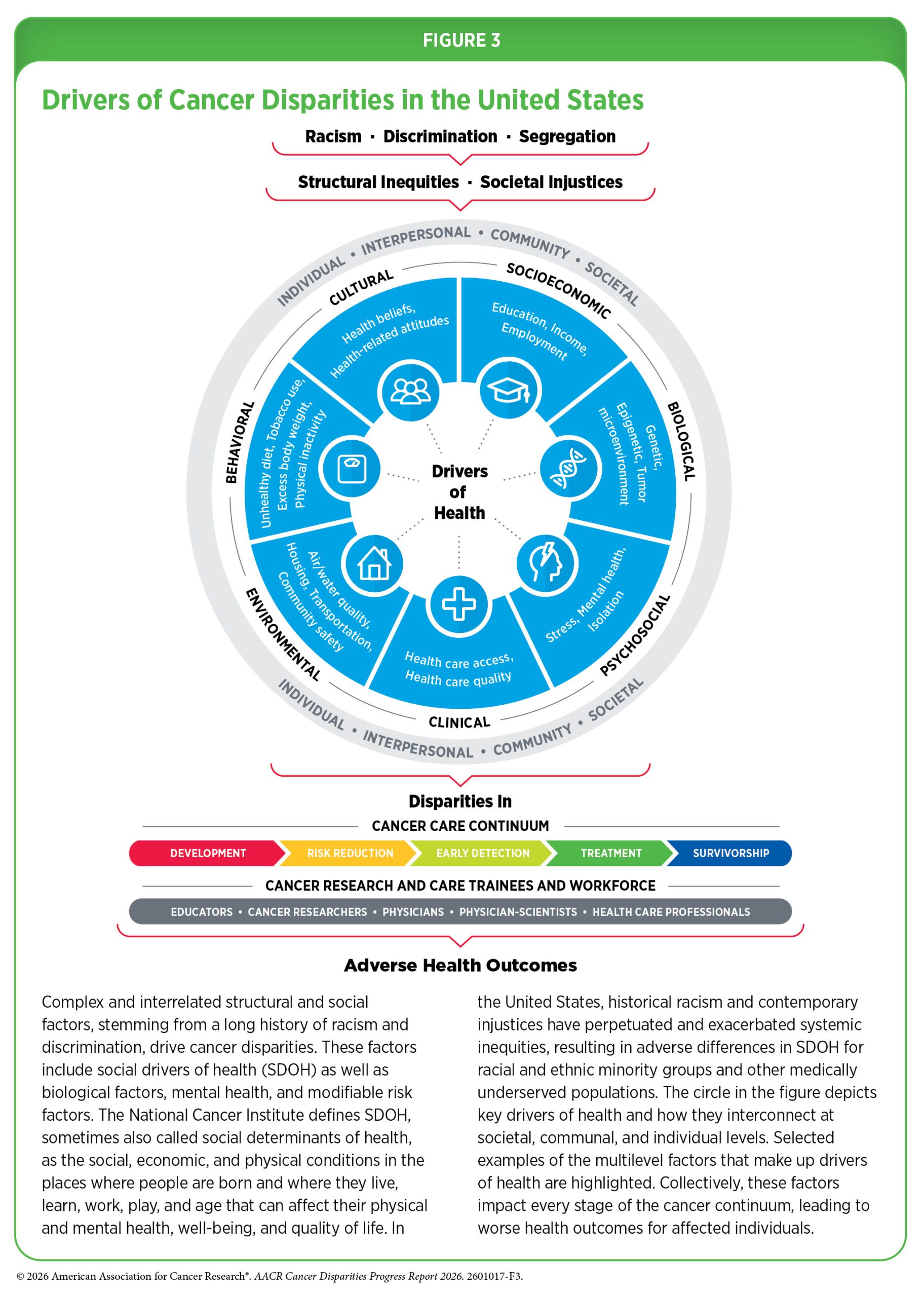
In the United States (US), centuries of systemic inequities and injustices have disproportionally exposed racial and ethnic minority groups and other medically underserved populations to adverse social and built environmental factors, collectively referred to as social drivers of health (SDOH) (see Figure 3). Adverse SDOH contribute to disparities in cancer burden by influencing access to health care and increasing exposure to behavioral risk factors, such as smoking and alcohol consumption, and environmental risk factors, such as air pollution and environmental carcinogens (see Understanding and Addressing Drivers of Cancer Disparities and Disparities in the Burden of Modifiable Behavioral Cancer Risk Factors). An active area of research is understanding how SDOH influence the complex biological mechanisms that contribute to cancer development, including genetic and epigenetic changes, chronic inflammation, and altered metabolism (189)Wagner M, et al. (2025) J Natl Cancer Inst, 117: 1981. (190)Turner DP, et al. (2024) Trends Cancer, 10: 673. . Experts emphasize the importance of understanding the interactions between biological factors and SDOH to identify opportunities to help mitigate the negative impacts of social factors on cancer risk and cancer-related health outcomes (191)National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Board on Health Care Services; National Cancer Policy Forum. Biological Effectors of Social Determinants of Health in Cancer: Identification and Mitigation: Proceedings of a Workshop. Nass S, Johnson A, Graig L, Balogh E, editors. Washington (DC): National Academies Press (US); 2025 Jan 15. PMID: 39446996.
Generating Knowledge Through Basic Research
The National Institutes of Health (NIH) defines basic research as the systematic study directed toward fuller knowledge or understanding of the fundamental aspects of a phenomenon and of observable facts without specific applications toward processes or products in mind. Basic research has broad implications because it is fundamental to our understanding and treatment of human diseases, including cancer.
Basic research plays a central role in the medical research cycle. Findings from basic research generate new hypotheses and identify potential targets for cancer prevention, early detection, diagnosis, and treatment. Promising approaches are then tested in preclinical models before advancing to evaluation in clinical trials. If clinical studies demonstrate safety and benefit, new interventions undergo regulatory review and approval. Once approved, therapies continue to be monitored in real-world use, providing insights that inform future research, prevention strategies, and public health policies (see Clinical Research).
Advances in genetics and genomics have been central to understanding cancer biology, enabling the identification of molecular alterations that drive cancer development and response to therapy. To ensure that discoveries benefit all populations, it is essential that genomic research includes individuals from diverse backgrounds, particularly populations that experience a disproportionate burden of cancer. Limited representation in research can obscure important biological variation and contribute to gaps in knowledge that may perpetuate disparities in cancer outcomes.
At the same time, accurately describing populations included in research studies, including how sociodemographic and biological characteristics are measured and reported, is essential for understanding the biological and social factors that influence cancer risk and outcomes. Broad population characteristics—such as race, ethnicity, ancestry, indigeneity, and geography—are often used to classify population groups and capture complex patterns of human diversity shaped by migration, evolution, and social and environmental exposures.
Racial and ethnic categories are commonly used population descriptors in research studies. These categories are self-identified or socially ascribed based on physical traits, cultural affiliation, shared heritage, and social experiences. Differences in socioeconomic conditions, environmental exposures, cultural practices, and access to health care often align with socially defined racial and ethnic population groups and can strongly influence cancer risk, detection, and outcomes. However, because race and ethnicity can differ across cultures, countries, and time periods, they are not biologically meaningful proxies for genetic variation.
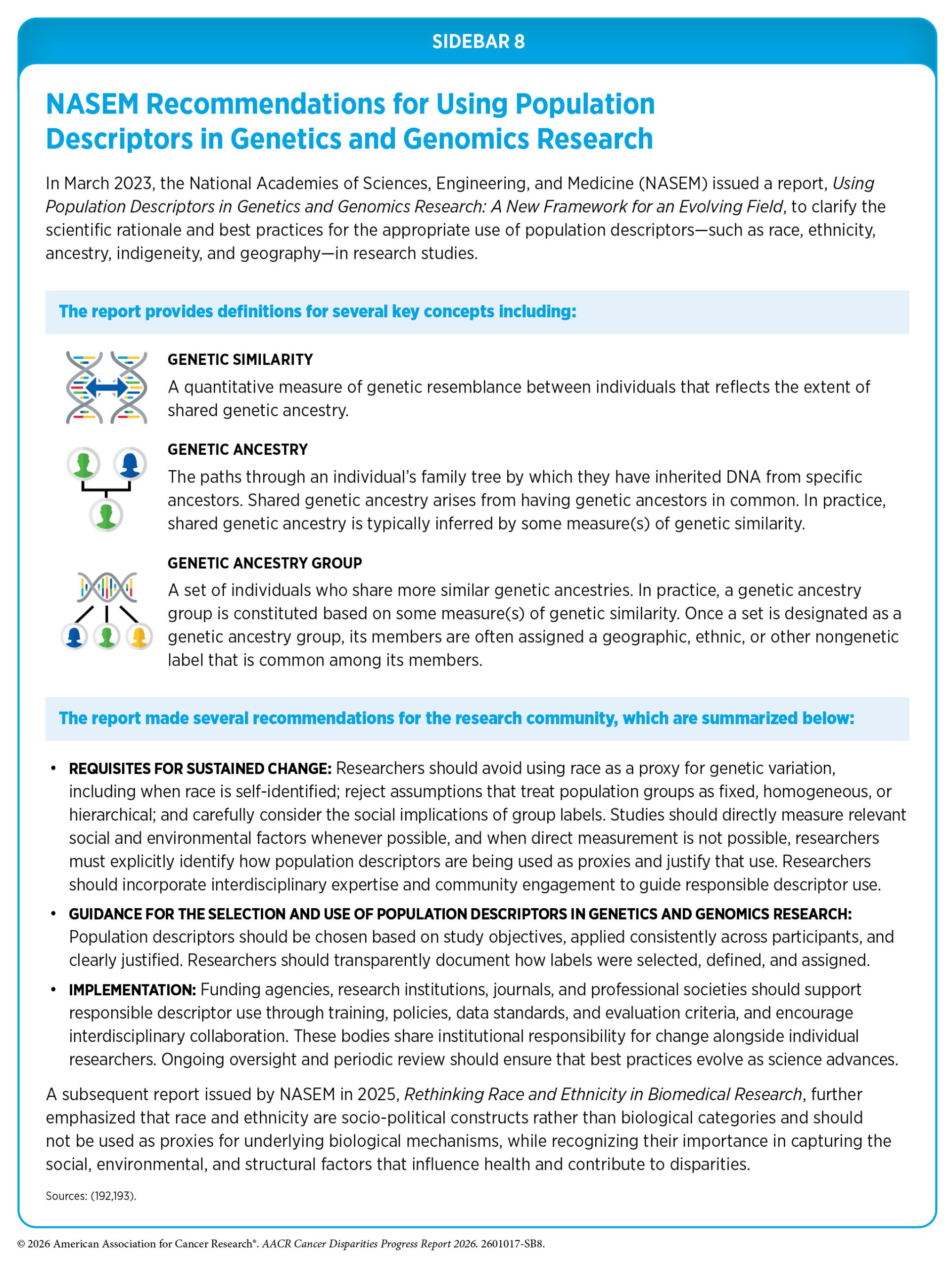
Recognizing this, researchers have increasingly emphasized the importance of using appropriate population descriptors when describing human genetic variation. Recent guidance from the National Academies of Sciences, Engineering, and Medicine recommends that researchers use population descriptors deliberately, tailor them to the scientific question, avoid using race as a proxy for genetic variation, and provide transparent justification for how and why descriptors are applied (see Sidebar 8) (192)National Academies of Sciences, Engineering, and Medicine. 2023. Using Population Descriptors in Genetics and Genomics Research: A New Framework for an Evolving Field. Washington, DC: The National Academies Press. This guidance also distinguishes genetic similarity, which is a quantitative measure of genetic resemblance between individuals, from genetic ancestry, which describes the inheritance of DNA from ancestral populations and is typically inferred using measures of genetic similarity. This distinction helps avoid conflating what is being measured (genetic similarity) with what is being inferred from that measurement (genetic ancestry), promoting clarity and transparency in genomics research.
Additionally, researchers have modeled genetic ancestry both as a set of broad categories, such as African, European, East Asian, South Asian, and Admixed American/Native or Indigenous American, and as continuous measures that can take on a full range of values along a spectrum, rather than being restricted to discrete categories. For example, researchers found that in head and neck cancer, a 10 percent increase in the proportion of inferred African or Native American ancestry was associated with a 9 percent and 36 percent higher risk of mortality, respectively, highlighting how modeling genetic ancestry, inferred from genetic similarity, as a continuous variable can reveal associations not captured by categorical groupings alone (194)Lee KK, et al. (2022) Cancer Res, 82: 1222. . Importantly, such associations should not be interpreted as causal effects of genetic ancestry itself and likely reflect a complex interplay of genetic variation, social and environmental exposures, and access to care.
Integrating genetic similarity and ancestry, which inform patterns of genetic variation, with race and ethnicity, which capture structural and social drivers of health, can improve the interpretation of research findings, enhance scientific rigor, and help ensure that discoveries benefit all populations.
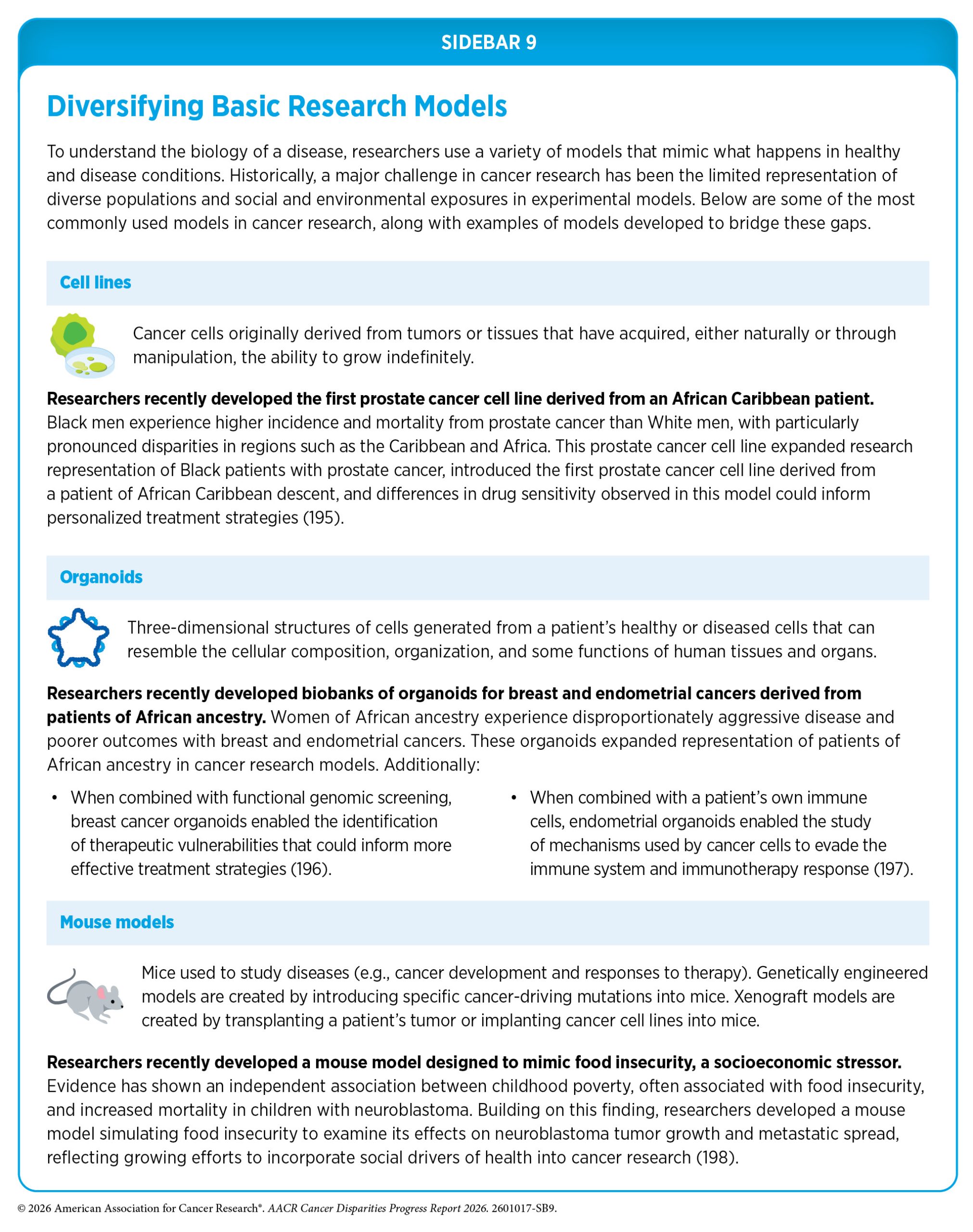
A major challenge in cancer research, and one of the main barriers to studying cancer disparities, has been the historical lack of diverse biospecimens in basic research models (see Sidebar 9). Many of these models have been developed using biospecimens derived from individuals of European ancestry, limiting their relevance across diverse populations. While researchers are working to address this challenge, representation of many populations remains limited. Lack of representation of diverse population groups in research models and biorepositories can result in data that may not be generalizable to all populations, thereby minimizing the applicability of research findings. Broad representation in cancer research models is especially important when studying diseases that disproportionately affect certain populations.
Expanding the representation of diverse populations in research resources requires coordinated efforts across the medical research community to develop cancer models and datasets that capture the biological, environmental, and social contributors to cancer disparities. Some initiatives are working to address this need by developing research models—such as patient-derived xenografts (PDXs), which are created by transplanting a patient’s tumor into mice—to better represent populations that have historically been underrepresented in cancer research. The PDX Development and Trial Centers Research Network (PDXNet) was launched by the National Cancer Institute (NCI) to coordinate collaborative, large-scale development and preclinical testing in PDX models to accelerate translational research (199)Lott PC, et al. (2024) Cancer Res Commun, 4: 2147. . PDXNet currently includes six PDX Development and Trial Centers, two of which were funded through the NCI Center to Reduce Cancer Health Disparities to develop and study PDX models to explore the biological drivers contributing to differences in cancer therapy outcomes in patient populations that are underrepresented in research.
Another initiative is the Florida–California Cancer Research, Education and Engagement (CaRE2) Health Center, which develops cancer model systems derived from participants identified as Black or Hispanic to study disparities in pancreatic, prostate, and lung cancers. These models are used for drug development and studying cancer biology (200)Reams RR, et al. (2023) Cancer Control, 30: 10732748231197878. .
Interpreting Knowledge to Understand the Biology of Cancer
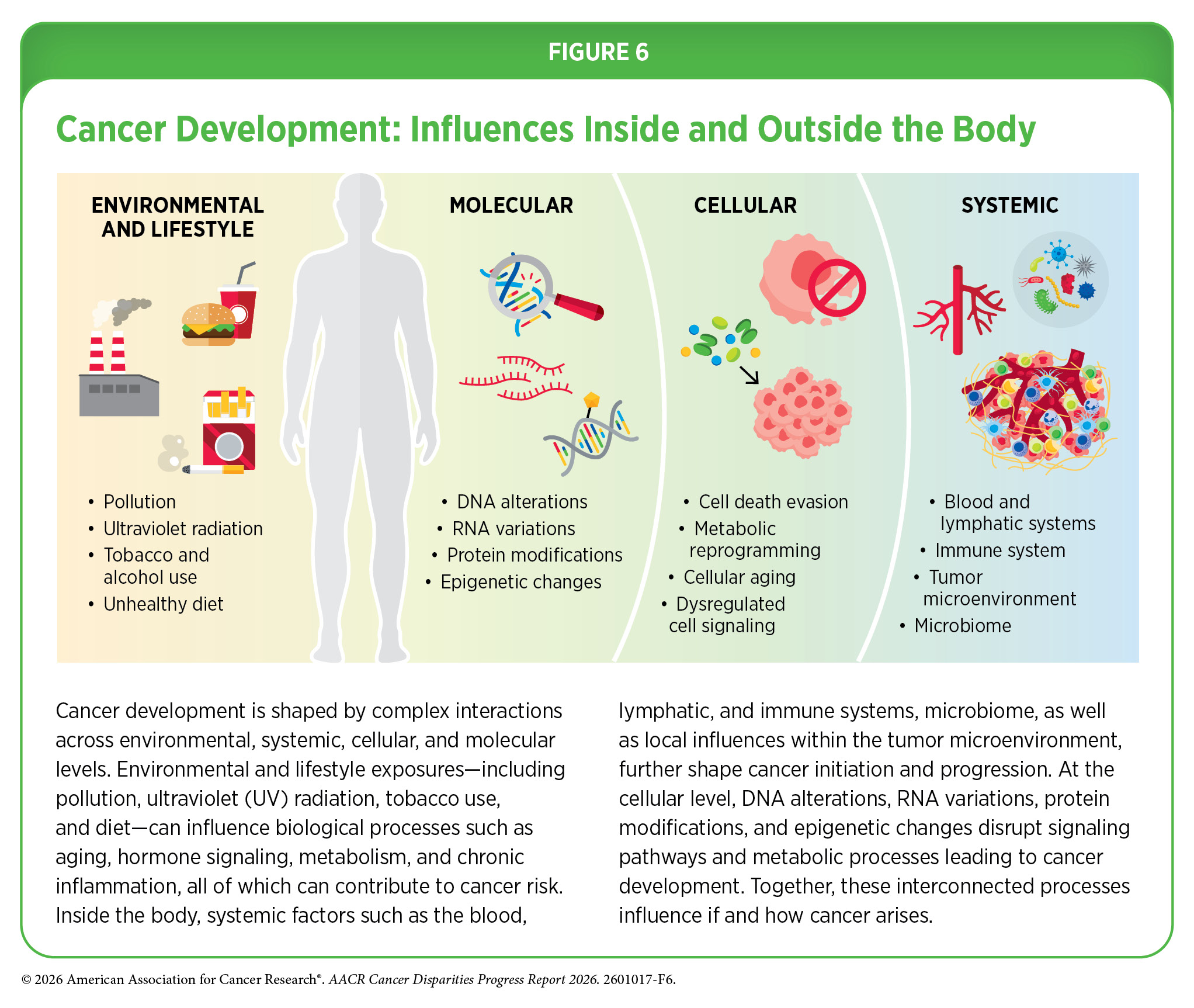
Cancer development is a complex and multistep process shaped by interactions among influences outside the body, throughout the body, within tissues, and inside individual cells (see Figure 6).
In the following sections, we describe the complex factors both inside and outside the cell that influence cancer initiation and progression. We also highlight differences in these biological processes across populations defined by race, ethnicity, and genetic ancestry, recognizing that these patterns may reflect a combination of genetic variation, environmental exposures, and structural and social factors that contribute to disparities in cancer risk, tumor behavior, and outcomes.
Influences Inside the Cell
Cells store their genetic information in deoxyribonucleic acid (DNA), a molecule comprising a double helix made of paired chemical bases—adenine (A), thymine (T), cytosine (C), and guanine (G)—arranged in repeating units called nucleotides. The entirety of a person’s DNA is called the genome. In cells, DNA is packaged with proteins called histones into structures known as chromatin, which are further compacted into chromosomes. Each chromosome contains hundreds to thousands of genes, which are segments of DNA that contain the instructions for making proteins. Through a process called transcription, these instructions in DNA are used to make a molecule called messenger ribonucleic acid (mRNA), which is then translated to make specific proteins that carry out essential functions in the body. When the genetic instructions or the processes that interpret them to make protein are altered, the finely tuned molecular and cellular programs that guide normal growth and development can be disrupted, leading to cancer development.
All humans share roughly 99.9 percent of their DNA sequence, with only 0.1 percent differing from one individual to another. However, this 0.1 percent encompasses millions of changes that contribute to what makes each person unique. Many of the genetic differences observed among individuals, which can vary in frequency across ancestry groups, are a result of human migration out of continental Africa approximately 100,000 years ago to other parts of the world, a process referred to as the human diaspora. As populations adapted to new climates, pathogens, diets, and environments, these factors shaped patterns of molecular variation that contribute to the diversity seen among human populations today (201)Nielsen R, et al. (2017) Nature, 541: 302. (202)Timmermann A, et al. (2016) Nature, 538: 92. .
Biological traits that arise from genetic differences can be positive, such as adaptation to unfavorable climates and altitudes, tolerance of specific diets, or resistance to infectious diseases. However, genetic differences can also influence susceptibility to complex diseases, including cancer, with some variants occurring at different frequencies across populations. Human migration, both voluntary and forced, has led to genetic mixture of ancestral groups. Genetic ancestry reflects the genomic contributions of different ancestral populations, and when inferred using measures of genetic similarity, can help identify molecular features associated with variation in disease risk across populations.
The following sections explore the changes inside the cell that can drive cancer development and highlight how these changes may vary among individuals from different population groups and contribute to disparities in cancer risk and outcomes.
Genetic Alterations
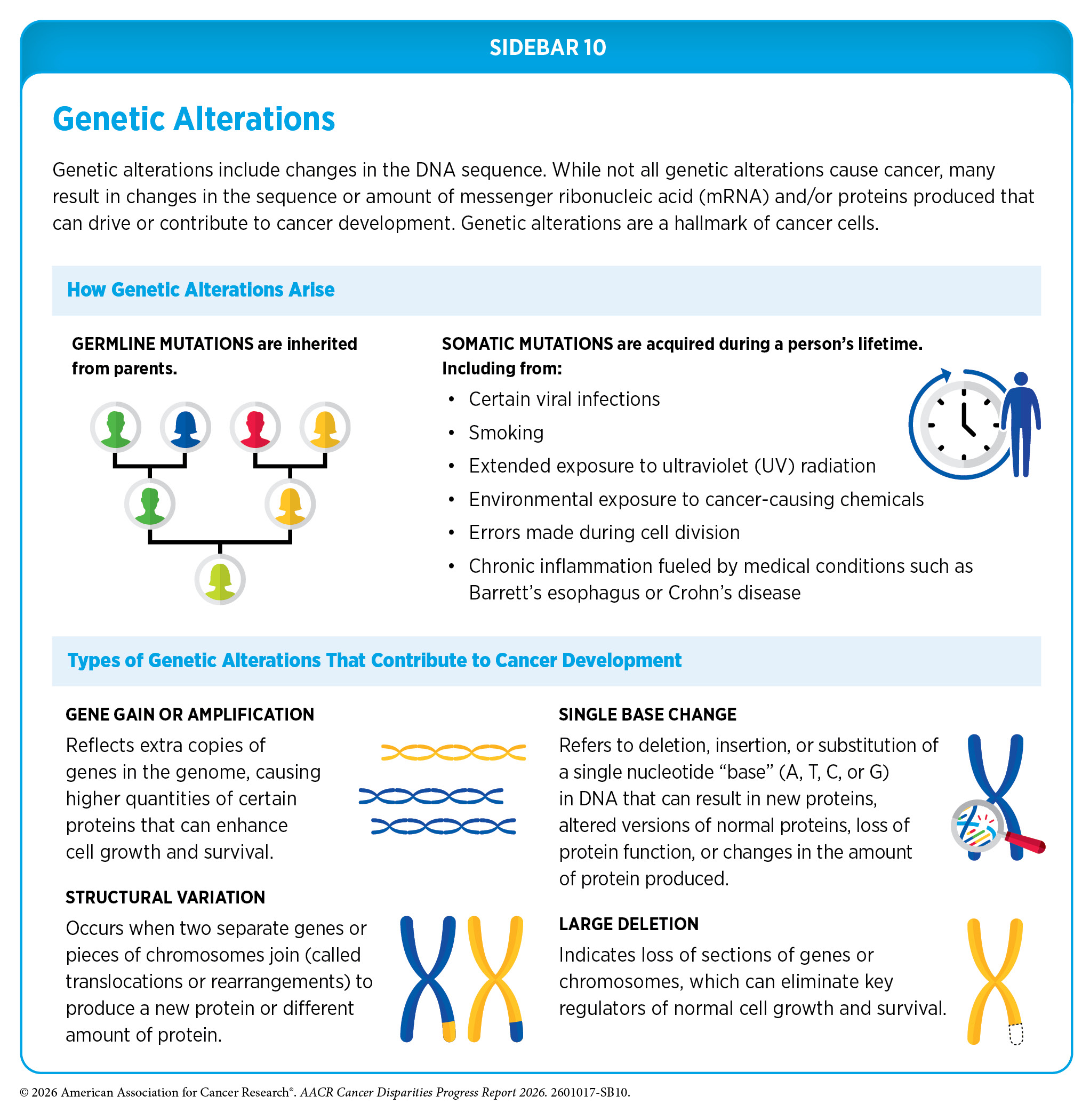
One hallmark of cancer cells is the occurrence of alterations in the DNA sequence. Also referred to as mutations, genetic alterations can change the sequence or amount of the resulting mRNA and protein, thus disrupting or modifying normal protein function and contributing to cancer development. Genetic alterations can be inherited from parents (germline mutations) or acquired throughout a person’s lifetime (somatic mutations) (see Sidebar 10).
To identify genetic alterations in cancer and other diseases, a patient’s genome is typically compared against a reference genome. The original human reference genome—the first complete sequence of the human genome generated by the Human Genome Project—has served as a foundational resource for genomic research for more than two decades. However, this reference genome lacked genetic diversity that naturally exists among different populations because it was derived from a small number of individuals that were mostly of European ancestry.
To address this limitation, researchers are developing reference pangenomes—collections of genome sequences from many individuals that together represent a broader range of human genetic diversity. The first human pangenome, assembled using 47 genetically diverse human genomes, was released in 2023 by the Human Pangenome Reference Consortium (HPRC), an initiative funded by NIH (203)Liao WW, et al. (2023) Nature, 617: 312. . In 2025, HPRC released an updated pangenome, which includes more than 200 genomes, with a near-term goal of including 350 genomes in 2026 (204)Marx V (2026) Nat Methods, 23: 487. . Ongoing efforts are focused on further expanding pangenomes representing populations that have historically been underrepresented in genomic studies (205)Logsdon GA, et al. (2025) Nature, 644: 430. (206)Nassir N, et al. (2025) Nat Med, 31: 725. (207)Gaye A, et al. (2024) Am J Hum Genet, 111: 2074. .
About 10 percent of cancer cases are caused by germline mutations. These mutations occur in the body’s reproductive cells (egg or sperm) that are passed on from parents to children and can increase their risk of developing cancer. However, not all germline mutations contribute to cancer development.
Because of limited genomic information from patients of non-European ancestry, there is often insufficient evidence to determine with confidence whether a mutation in a non-European patient is truly cancer-causing; these mutations are categorized as variants of unknown significance. Consequently, genetic counseling, which guides patients on how genetic findings may affect their cancer risk and care, becomes less precise and less informative. The need for more research is urgent to better understand variations in inherited genetic alterations in people from different ancestral backgrounds.
Thanks to technological advances in DNA sequencing and large-scale genome-wide association studies—which analyze hundreds of thousands to millions of genetic variations across the genome to identify variants associated with disease risk—researchers are gaining new insights into differences in the frequency of germline variants across populations with differing genetic ancestry associated with cancer risk and can inform early detection and interception, surveillance, and treatment decisions. Increasingly, studies are incorporating populations matched based on genetic similarity and analytical approaches to improve the relevance of findings across populations.
Inherited variants can influence cancer susceptibility through differences, both in how often they occur and which variants are present across populations. For example, in a study of women with ovarian cancer, patients of self-reported Ashkenazi Jewish ancestry had the highest rates of germline mutations in BRCA1/2 and other genes related to DNA repair that are associated with increased cancer risk (208)Aryasomayajula C, et al. (2026) Gynecol Oncol, 204: 1. . Additionally, recent studies analyzing lung cancer risk across individuals with genetically inferred African and East Asian ancestries have identified genetic variants associated with cancer susceptibility, including variants that had not previously been detected in studies largely conducted in people of European ancestry (209)Betti MJ, et al. (2025) Am J Hum Genet, 112: 2102. (210)Chen TY, et al..
Blood levels of prostate-specific antigen (PSA) are used for routine prostate cancer screening and are indicative of potential prostate cancer if above a certain threshold (see Prostate Cancer Screening). Evidence shows that germline genetic variants can also contribute to differences in PSA levels. Genetic cancer risk prediction models based on variants of the PSA gene perform poorly in patients of non-European ancestry, particularly in individuals of African ancestry who experience a higher burden of prostate cancer. Recent research has shown that including participants from underrepresented populations could improve the accuracy of genetic prediction models for PSA across genetic ancestry groups and may support more inclusive prostate cancer screening strategies (211)Hoffmann TJ, et al. (2025) Nat Genet, 57: 334..
Similarly, many breast cancer risk prediction models rely on common risk variants identified in women of European ancestry and therefore perform poorly when applied to women of African ancestry. Studies have shown that including women of African ancestry in genomic studies improves the identification of risk variants and increases the accuracy of risk prediction in this population (212)Jia G, et al. (2024) Nat Genet, 56: 819. (213)Jia G, et al. (2025) Nat Genet, 57: 80. .
Inherited genetic differences associated with disease risk and outcomes across populations defined by ancestry and other demographic factors have also been observed in childhood cancers. Research has shown that certain variants associated with an increased risk of childhood acute lymphoblastic leukemia (ALL) are observed at a higher frequency in Hispanic populations (214)Langie J, et al. (2026) Human Genetics and Genomics Advances, 7. (215)de Smith AJ, et al. (2024) Cell Genomics, 4. . Additionally, in a study of children with B-cell ALL, researchers identified that genetic alterations observed at higher frequency among children of African ancestry were associated with worse survival (216)Im C, et al. (2025) Nat Commun, 16: 8974. .
Somatic, or acquired, mutations arise during an individual’s lifetime, often because of errors during normal cell division or in response to environmental exposures, lifestyle factors, or chronic health conditions. These mutations contribute to the unique genetic landscape of individual tumors, with distinct patterns reflecting potential causes of cancer, tissue of origin, and evolving over time.
There is mounting evidence that somatic mutational profiles across many cancer types vary as a function of genetic ancestry, with potential implications for therapeutic interventions (187)Amuzu S, et al. (2025) Nat Genet, 57: 2655. . Several recent studies have identified differences in somatic mutation patterns observed among individuals from different ancestry groups that may contribute to disparities in incidence and survival in lung and head and neck cancers (218)Jain S, et al. (2024) JCO Precis Oncol, 8: e2400223. (219)Sisoudiya SD, et al. (2024) NPJ Precis Oncol, 8: 153. (220)Ndahayo M, et al. (2026) Cancer Metastasis Rev, 45: 6. .
Similarly, research in breast cancer has identified differences in both somatic and germline mutations observed among women from different ancestry groups that may influence cancer risk and treatment response, with women of African ancestry more likely to develop aggressive tumors and to be diagnosed and die at younger ages (221)Thorn GJ, et al. (2025) Nat Commun, 16: 4237. .
Differences in tumor burden and in the frequency of specific somatic mutations have also been observed across racial and ethnic population groups, which may reflect not only differences in genetic variation but also disparate influences of structural and SDOH, such as environmental exposures and lack of health care access (see Understanding and Addressing Drivers of Cancer Disparities) (222)Wen W, et al. (2025) Cancer Epidemiol Biomarkers Prev, 34: 2208. (223)Brown LM, et al. (2024) Nat Commun, 15: 8218. .
In pancreatic and prostate cancers, Black individuals experience the highest incidence and mortality rates among all population groups (see The State of US Cancer Disparities in 2026). Recent studies have identified unique somatic alterations and immune features in pancreatic and prostate tumors across patient populations, which may contribute to differences in cancer development and outcomes (224)Mandal S, et al. (2025) Cancer Res Commun, 5: 128. (225)Elbialy A, et al. (2025) Cell Insight, 4: 100238. .
The incidence of early-onset cancer—defined as cancer diagnosed in young adults ages 18 to 49 years—has been rising globally (226)Zhao J, et al. (2023) BMJ Oncol, 2: e000049. . Colorectal cancer (CRC) is now the leading cause of cancer-related death among individuals under 50 years (19)Siegel RL, et al. (2026) CA Cancer J Clin, 76: e70067. . Research has identified distinct patterns of somatic mutations in early-onset CRC that vary across patient populations defined by factors such as ancestry, geography, biological sex, and social and demographic characteristics (227)Hein DM, et al. (2022) J Natl Cancer Inst, 114: 775. (228)Li J, et al. (2025) Lancet Oncol, 26: 1055. . Several recent studies have reported differences in somatic mutation profiles in early-onset CRC between patients identified as Hispanic and White; however, these differences likely reflect a complex interplay of genetic variation, environmental exposures, and SDOH, rather than inherent differences attributable to race or ethnicity (229)Monge C, et al. (2025) Cancer Med, 14: e70791. (230)Monge C, et al. (2025) Cancers (Basel), 17. (231)Monge C, et al. (2025) Cancers (Basel), 17. .
Continuing to expand our knowledge of how distinct genetic alterations drive cancer development across diverse populations will be essential for developing equitable strategies for cancer prevention, diagnosis, and treatment.
RNA Variations
Gene expression is the process by which a cell reads the instructions in a gene to produce mRNA. Cells can regulate this process to increase or decrease mRNA production as needed to respond to internal and external signals. In cancer, these regulatory processes often go awry.
Most genes are made up of alternating segments known as exons and introns. Exons contain the instructions needed to make proteins, whereas introns do not. When a gene is transcribed into mRNA, the resulting transcript includes both exons and introns. Through a “cut and paste” process called RNA splicing, the introns are removed and the exons are joined together to produce an mRNA molecule that can then be translated into a functional protein.
If errors occur during the RNA splicing process, faulty mRNAs can produce dysfunctional proteins that can drive cancer development and even cause therapeutic resistance. Research has identified differences in RNA splicing across population groups that may contribute to biological mechanisms underlying outcome disparities in prostate and lung cancers (232)Al Abo M, et al. (2025) NPJ Precis Oncol, 9: 30. (233)Zeeshan S, et al. (2025) Oncogene, 44: 958. .
Understanding changes in gene expression and RNA processing within tumors provides vital insights into how cancer develops, evolves, and spreads. Technologies such as transcriptomics and single-cell RNA sequencing are being used to identify and understand RNA-level changes by mapping how genes are expressed within individual tumor cells and across different regions of a tumor.
Differences in mRNA expression levels have been demonstrated in cancers from different population groups. For example, a transcriptomics analysis of colon tumors from Black and White patients identified distinct gene expression patterns at localized, regional, and metastatic stages, including differences in immune-related pathways and genes linked to tumor progression (234)El Moheb M, et al. (2025) Ann Surg Oncol, 32: 736. . These findings highlight variation in tumor characteristics across patient groups and may contribute to understanding why, when compared to White patients, Black patients with colon cancer experience worse outcomes at every stage of disease. However, these differences likely reflect a complex interplay of social, environmental, and biological factors rather than inherent differences attributable to race itself.
Recent research suggests that even normal pancreatic tissue can harbor transcriptomic features associated with cancer risk. Analyses have identified distinct gene expression states in normal tissue that resemble known pancreatic cancer subtypes and found that the likelihood of these changes varied with genetic similarity, with individuals showing greater genetic similarity to populations with African ancestry more likely to exhibit these early changes than those with greater genetic similarity to populations with Indigenous American ancestry (235)Perkins CM, et al. (2026) Cancer Res Commun, 6: 165. .
In prostate cancer, researchers have shown that neighborhood disadvantage is associated with increased expression of genes linked with stress and inflammation. Because chronic stress can promote inflammatory pathways linked to prostate tumor initiation and progression, these findings suggest a potential mechanism through which social and environmental exposures may contribute to an increased risk of aggressive prostate cancer (236)Boyle J, et al. (2024) JAMA Netw Open, 7: e2421903. .
In addition to mRNA, cells also produce non-coding RNAs (ncRNAs)—RNA molecules that do not encode proteins but play critical roles in regulating gene expression. These include microRNAs (miRNAs), long non-coding RNAs (lncRNAs), and circular RNAs, each of which can drive normal cellular processes but also influence how tumors grow, interact with their environment, and resist treatment.
Studies have reported differences in ncRNA levels and/or function across racial and ethnic population groups (237)Zhao D, et al. (2025) Wiley Interdiscip Rev RNA, 16: e70028. (238)Morgan RA, et al. (2025) Genes (Basel), 16. . A recent study found adults experiencing high levels of perceived discrimination had differences in the expression of certain lncRNAs and miRNAs involved in immune and inflammatory responses (239)Pacheco NL, et al. (2025) FASEB J, 39: e70366. . These findings may provide insight into how adverse social factors may differentially influence biological processes leading to disparities in cancer development and outcomes (see Understanding and Addressing Drivers of Cancer Disparities).
Protein Modifications
Proteins are vital for normal cellular functions. The full set of proteins expressed by the cell, known as the proteome, contains approximately 20,000 unique proteins. Proteomics is the study of the proteome, which can reveal important molecular features that are not apparent from studying the DNA or RNA alone.
In a large-scale proteomic study of patients across diverse racial and ethnic backgrounds, researchers identified both shared and population-specific proteins associated with prostate cancer risk. However, the number of proteins identified varied substantially by population group, likely reflecting differences in sample size and representation, highlighting the need for more inclusive datasets to ensure equitable risk prediction across populations (240)Zhong H, et al. (2025) Nat Commun. .
The functions of many proteins are regulated by posttranslational modifications (PTMs), which are reversible chemical changes that occur after a protein is formed and modulate its function, localization, and stability. A recent study integrating proteomics and PTMs with genomic data in lung cancer patients representing diverse ethnic backgrounds and environmental exposures identified differences in protein expression and PTMs linked to environmental carcinogens, immune responses, and clinical outcomes (241)Satpathy S, et al. (2025) Cancer Cell, 43: 1731. .
In the United States, NCI is playing a vital role in supporting research on proteomic alterations in cancer through the Clinical Proteomic Tumor Analysis Consortium (CPTAC). CPTAC researchers generate data on how alterations in protein modifications play a role in cancer and are discovering novel avenues for therapeutic intervention, and efforts are underway to increase the diversity of biospecimens from underrepresented populations in proteogenomic datasets.
Epigenetic Changes
Epigenetic modifications are chemical changes that regulate how genes are expressed without altering the underlying DNA sequence. The entirety of epigenetic changes within a cell is called the epigenome. Epigenetic changes are shaped by aging, environmental exposures (e.g., air pollution and ionizing radiation), behavior and lifestyle factors (e.g., cigarette smoking), and psychosocial stressors (e.g., systemic racism and discrimination) (see Disparities in the Burden of Modifiable Behavioral Cancer Risk Factors) and may be passed on from parent to child. Some epigenetic changes are reversible, and harnessing this discovery for therapeutic purposes is an area of intensive investigation.
One common type of epigenetic modification is DNA methylation, in which methyl groups are added to specific regions of the genome to regulate whether nearby genes are turned on or off. Research suggests that epigenetic differences in tumors observed among individuals from different ancestry groups may contribute to cancer disparities. For example, distinct DNA methylation patterns reflecting differences in tumor behavior have been identified among men of European and African ancestries who have prostate cancer and may contribute to understanding the higher prevalence of aggressive disease among men of African ancestry (243)Craddock J, et al. (2025) Mol Syst Biol, 21: 1676. (244)Chernoff M, et al. (2025) Cancer Epidemiol Biomarkers Prev, 34: 428. .
Racial disparities in outcomes have been seen in ovarian and endometrial cancers, particularly between Black and White women. Although White women have a higher incidence of ovarian cancer, Black women experience worse survival. Additionally, Black women have a higher incidence and mortality from endometrial cancer compared to White women. Recent studies comparing ovarian and endometrial tumors from Black and White women have identified differences in DNA methylation patterns related to metabolism and immune responses in tumors from Black women that may contribute to aggressive disease and poorer clinical outcomes, within a broader context shaped by interacting social, environmental, and biological factors (245)Huang H, et al. (2024) NPJ Genom Med, 9: 64. (246)Hoos E, et al. (2025) Carcinogenesis, 46. .
There is increasing evidence suggesting that social and environmental factors, such as redlining, segregation, and neighborhood deprivation (see Understanding and Addressing Drivers of Cancer Disparities), may drive cancer disparities through modulation of the tumor epigenome. For example, high neighborhood deprivation and air pollution have been linked to inflammatory changes in breast tissue and differences in DNA methylation associated with breast cancer risk (160)Harris AR, et al. (2025) JAMA Netw Open, 8: e2461334. . Additionally, living in neighborhoods with higher levels of violence, used as a marker of chronic social stress, was associated with differences in PRMT6 expression—an epigenetic regulator linked to lung cancer progression and poor outcomes (247)Kim SJ, et al. (2025) Cancer Prev Res (Phila). . These findings suggest that social and environmental conditions may influence tumor biology in ways that contribute to cancer disparities and highlight the vital need for investments in public health interventions and policy changes at the neighborhood level.
Influences Outside the Cell
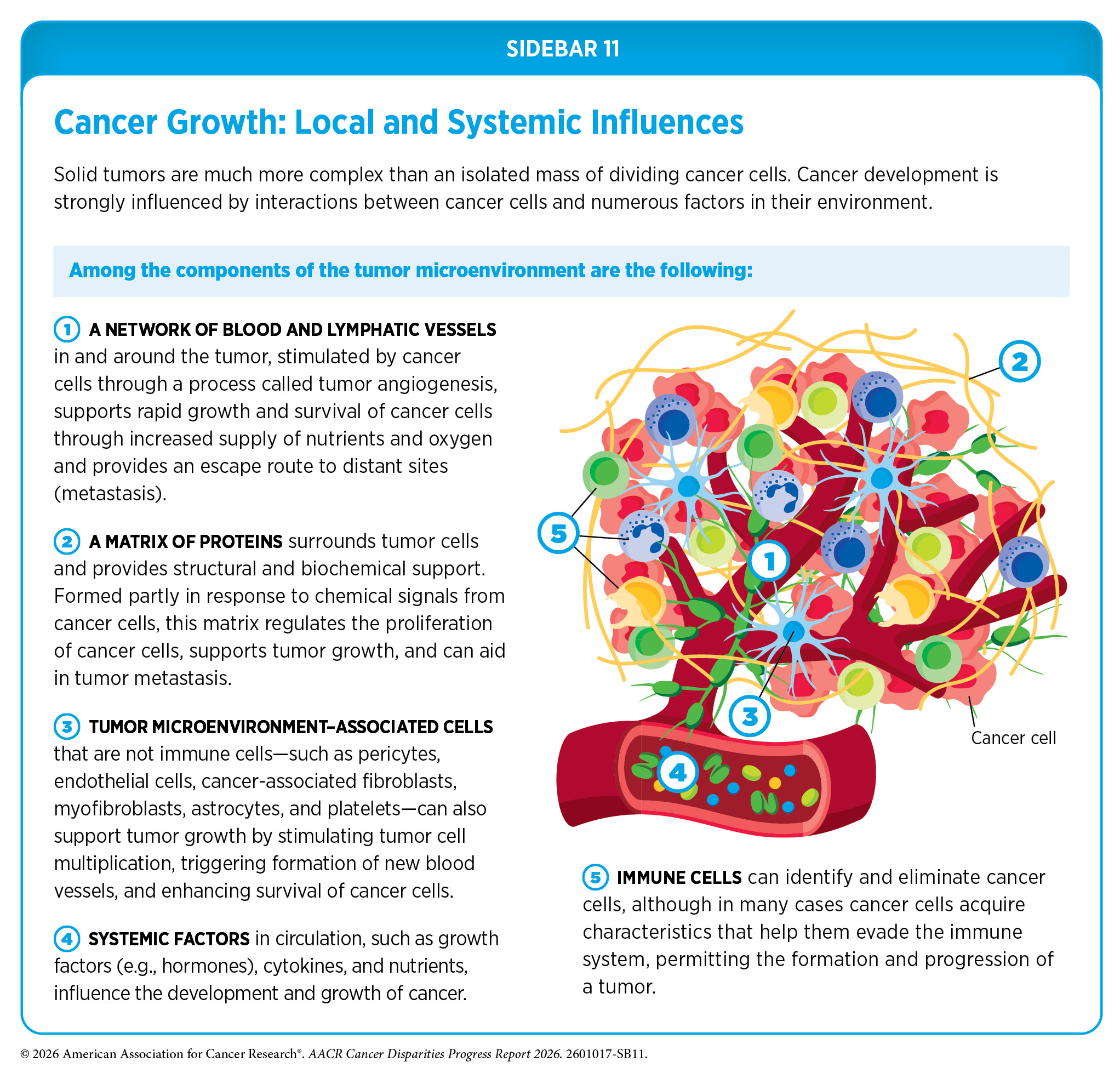
In addition to alterations inside the cell, influences outside the cell contribute to cancer initiation, progression, and response to therapy (see Sidebar 11). A hallmark of cancer is the ability of tumor cells to break away from the primary tissue and travel to other parts of the body. This process—known as metastasis—is enabled by the blood and lymphatic systems, which can provide physical routes through which cancer can spread, and the immune system, which can either suppress or support tumor progression, depending on how it is activated or suppressed.
The microbiome—comprising diverse microorganisms residing on and in the body—can influence cancer development by modulating inflammation, immune responses, and systemic metabolism. The tumor microenvironment encompasses the cellular and structural context in which a tumor exists and shapes how cancer evolves and responds to treatment.
The following sections describe the differences in influences outside the cell that may contribute to disparities in cancer development and treatment response across populations.
Blood, Lymphatic, and Immune Systems
The blood, lymphatic, and immune systems influence how tumors grow, spread, and interact with their surrounding environment, shaping both disease course and therapeutic outcomes.
The blood and lymphatic systems are composed of interconnected networks of vessels, circulating cells, signaling molecules, and lymph nodes, as well as several organs, including spleen, thymus, tonsils, and adenoids. Together, these networks deliver oxygen and nutrients throughout the body, remove cellular waste from tissues, and support the immune system.
One hallmark of cancer cells is the ability to promote angiogenesis—the formation of new blood vessels—toward and within a tumor, increasing tumor vascularization to meet the high demand of oxygen and nutrients needed to fuel tumor growth. Cancer cells can produce and release high levels of vascular endothelial growth factors (VEGF), a family of signaling proteins that stimulate angiogenesis. Tumors can also increase the formation of new lymphatic vessels—a process known as lymphangiogenesis—that increase opportunities for cancer cells to access and spread through the lymphatic system, particularly to nearby lymph nodes.
The degree to which tumors become vascularized can be an indicator of tumor aggressiveness and patient outcomes. A recent study showed that higher levels of genes and proteins that are associated with VEGF and regulate angiogenesis and lymphangiogenesis were observed in breast tumors from women of African ancestry compared to those from women of European ancestry (248)Han YJ, et al. (2024) Clin Cancer Res, 30: 2609. . These findings may contribute to understanding the prevalence of more aggressive tumors and poorer survival among women of African ancestry with breast cancer.
The immune system is composed of a variety of organs, tissues, cells, and molecules that work together to defend the body against pathogens (e.g., viruses and bacteria) and diseases (e.g., cancer). How the immune system responds to threats depends on many factors, including hereditary factors and the types of exposures individuals encounter in their lifetime.
Recent research has identified germline variants in genes regulating immune system functions that differ in frequency across populations. In an analysis of individuals representing 26 populations across Africa, East Asia, Europe, South Asia, and the Americas, researchers found variants in immune-related genes that may contribute to variation in tumor immunity, inflammation, and response to immunotherapy among individuals from different ancestry groups (249)Hu X, et al. (2026) Cell Rep, 45: 116882. .
Emerging research has shown that levels of certain immune molecules in circulation and within the tumor microenvironment differ across socially defined racial groups, including biomarkers associated with immune response and inflammation among patients with breast, lung, and pancreatic cancers, likely reflecting complex interactions between biological processes, environmental exposures, and social context rather than inherent biological differences attributable to race itself (250)Zhu Q, et al. (2025) Nat Commun, 16: 6584. (251)Trendowski MR, et al. (2024) Cancer Epidemiol Biomarkers Prev, 33: 1220. (252)Gao Z, et al. (2025) J Surg Res, 307: 21. .
Further, evidence shows chronic stress and structural disadvantages, such as discrimination and neighborhood deprivation, can adversely affect the immune system and contribute to differences in cancer aggressiveness and disparities in outcomes in socially vulnerable populations (146)Harris AR, et al. (2025) JAMA Netw Open, 8: e2459754. . A conceptual framework has been proposed to study how SDOH, environmental exposures, and stress contribute to epigenetic and immune dysregulation, and how these factors jointly drive breast cancer mortality and cancer disparities (253)Falcone M, et al. (2024) Cancer Research, 84: 3924. .
Research has shown that the ability of the immune system to recognize and eliminate cancer cells varies depending on the molecular characteristics of a tumor. Insights into the interplay between the immune system and cancer form the basis for developing immunotherapies, which leverage the natural ability of the immune system to fight cancer. The US Food and Drug Administration (FDA) has approved immunotherapies for many different types of solid tumors and blood cancers that have been highly successful (see Treatment With Molecularly Targeted Therapy and Immunotherapy). Despite this success, the development of immunotherapies has been primarily based on clinical samples from individuals of European ancestry, with limited data from populations of non-European ancestries. This is troubling because studies have reported variation in immune function across populations with different ancestries, which likely reflects a complex interplay of genetic variation, environmental exposures, and social context, indicating that there cannot be a “one-size-fits-all” approach. Comprehensive analysis of the immune system of cancer patients from diverse racial, ethnic, and ancestral backgrounds is vital to develop interventions that are effective in these populations.
Glioblastoma multiforme (GBM) is an aggressive type of brain cancer for which immunotherapies have historically failed. Recently, researchers found that distinct GBM molecular subtypes could be identified among patients of East Asian ancestry, including a subtype enriched in this group that shows improved response to immunotherapy (254)Zhong S, et al. (2025) Cell Rep Med, 6: 102217. . Similarly, immune checkpoint inhibitors (ICIs), a class of immunotherapeutics that activate cancer-eliminating immune cells by blocking proteins that would otherwise restrain them, have shown limited efficacy in prostate cancer. However, research has indicated that prostate cancer patients of African ancestry exhibit immune features associated with improved responses to ICIs compared to patients of European ancestry (188)Luo M, et al. (2025) Cancer Discov, 15: 511. .
Notably, patients of African ancestry are underrepresented in clinical trials of ICI therapy, which may contribute to the limited efficacy reported (see Challenges in Cancer Clinical Trials). These findings highlight the importance of understanding how immune features observed among individuals from different population groups influence response to immunotherapy and underscore the need for diverse clinical trial representation to ensure these potential benefits reach all patients.
Microbiome
The microbiome is made up of all the microbes—bacteria, fungi, viruses, and other microorganisms—that live on and in the skin, mouth, gut, and other sites in the body. Studies have shown that microbiomes play essential roles in digestion, metabolism, immune system regulation, and protection against pathogens. SDOH can affect the composition and diversity of the microbiome within an individual and between individuals through environmental, socioeconomic, cultural, dietary, lifestyle, and health care exposures (255)Byrd D, et al. (2024) Nat Rev Cancer, 24: 89. . In a recent study, researchers found that dietary changes of populations in South Africa to Western diets—characterized by increased consumption of fat and animal protein—were linked to reduced microbiome diversity and altered microbiome composition in the gut, changes that are associated with increased CRC risk (256)Ramaboli MC, et al. (2024) Nat Commun, 15: 3379. .
Microorganisms residing in the gut can influence the immune system, metabolism, and the production of metabolites such as short-chain fatty acids (SCFAs). SCFAs are small molecules produced when gut bacteria break down dietary fiber and help support the immune system and maintain a healthy gut environment. Research exploring differences in gut microbiome and SCFA composition in populations classified by race and ethnicity across different cancers has found that lower SCFA levels in some groups may contribute to increased inflammation, reduced tumor suppression, and altered epigenetic regulation (257)Miya TV, et al. (2023) Cancers (Basel), 15. .
The interplay between the vaginal microbiome and human papillomavirus in cervical precancers and cancer development is also an area of ongoing research. Emerging data suggest that the risk of cervical cancer associated with the vaginal microbiome may vary across populations classified by race or ethnicity (258)Laniewski P, et al. (2024) Cancer Prev Res (Phila), 17: 525. . Future studies will determine whether early detection and modulation of specific microbes may aid in cancer prevention or interception efforts.
The oral microbiome is influenced by diet and exposures to carcinogens. Use of chewing tobacco and betel nut—which is particularly prevalent among Asian and Native Hawaiian or Pacific Islander populations (see Commercial Tobacco Use)—has been implicated in carcinogenesis within the oral and oropharyngeal cavities. These exposures can induce microbiome imbalance, leading to chronic inflammation, immune evasion, and activation of tumor-promoting pathways (259)Xu K, et al. (2025) Discover Oncology, 17: 59. (260)Menghani SV (2025) The American Journal of the Medical Sciences, 369: 556. .
Targeting the microbiome may offer opportunities to improve health outcomes for patients with cancer. However, a better understanding of interactions between patients and their microbiome in the context of cancer disparities is needed. Preclinical and clinical studies evaluating the microbiome as a driver of cancer and cancer disparities must recruit participants across diverse populations and consider SDOH alongside biological data to accurately ascertain the contributions of the microbiome to cancer risk.
Tumor Microenvironment
The tumor microenvironment (TME)—composed of cancer cells and supportive non-cancer cells, blood vessels, signaling molecules, and structural components (see Sidebar 11)—is a dynamic biological system that influences cancer development. Cancer cells shape the TME by releasing molecules that secure nutrients and structural support essential for their growth. Proteins and molecules released by cancer cells can also affect the behavior of nearby healthy cells and influence distant tissues to support tumor progression.
Differences in the TME may result from factors associated with inherited genetic variation, increased levels of chronic inflammation, epigenetic changes from social and environmental exposures, variation in immune response, or a combination of these (252)Gao Z, et al. (2025) J Surg Res, 307: 21. (262)Abubakar M, et al. (2025) Cancer Epidemiol Biomarkers Prev, 34: 462. . Research has identified components of the TME that differ across patient populations classified by race and ethnicity (252)Gao Z, et al. (2025) J Surg Res, 307: 21. (263)Parmar P, et al. (2026) NPJ Breast Cancer, 12: 3. (264)Cobbs Ct, et al. (2025) Cancer Med, 14: e70979. . As one example, a recent study found that breast tumors in Black and White women differed in certain aspects of collagen structure—the scaffolding that surrounds tumor cells (265)Elias TM, et al. (2025) Biophotonics Discov, 2. .
Within the TME, the tumor immune microenvironment (TIME) refers to the network of immune cells and immune-modulating factors that interact with the tumor. Recent advances in single-cell and spatial transcriptomic technologies (see RNA Variations) have revealed that the TIME plays an important role in cancer progression and response to therapy, and a deeper understanding of the processes within this environment is essential for developing effective immunotherapies. In a recent study, researchers using single-cell and spatial transcriptomic technologies uncovered distinct tumor-promoting and immunosuppressive microenvironments in tumors from Black and White women with triple-negative breast cancer, a particularly aggressive form of breast cancer, which may contribute to disparities in clinical outcomes (250)Zhu Q, et al. (2025) Nat Commun, 16: 6584. .
Collectively, the examples discussed here show how factors shaping cancer development, including social and environmental exposures, can influence biology at multiple levels, from genetic alterations to the TME. These interconnected influences may contribute to differences in cancer risk, tumor behavior, and treatment response across populations. Continued research is needed to better understand how SDOH interact with cancer biology and to inform strategies that reduce disparities in cancer outcomes.
Integrating Knowledge to Accelerate Cancer Disparities Research and Advance Precision Medicine
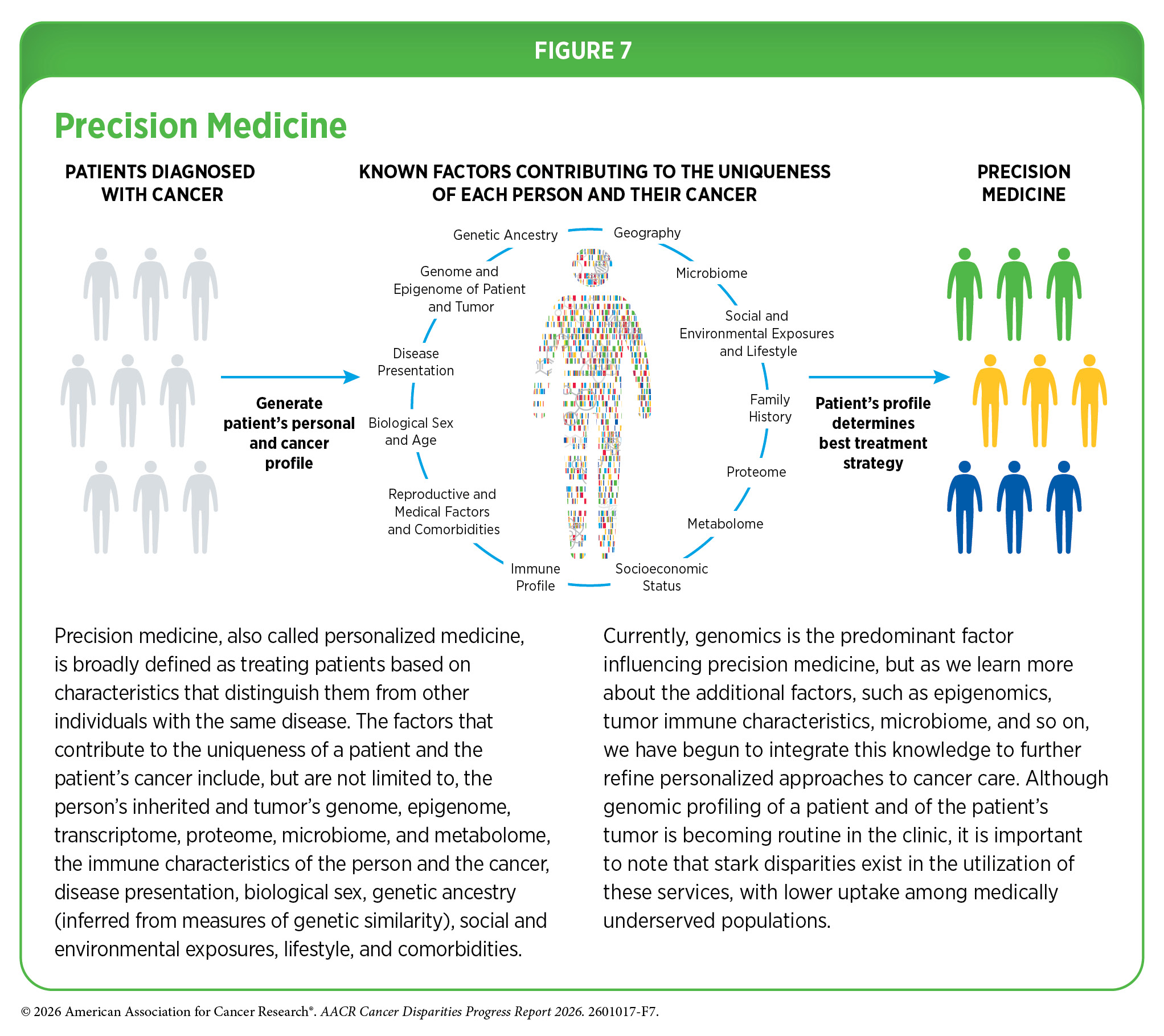
One of the most important insights gleaned from our current knowledge of the complexities underpinning cancer development is that each patient’s cancer is unique, shaped by a distinct combination of biological, lifestyle, environmental, and ancestral influences. In fact, in the past two decades there has been a shift from a “one-size-fits-all” approach to cancer prevention, screening, and treatment to a more personalized approach called precision medicine (see Figure 7). While genomics is the predominant factor influencing current precision cancer medicine efforts, researchers are rapidly accumulating data on additional cancer-associated measures, including epigenetic, transcriptomic, immune, metabolic, microbial, and protein profiles, to better understand and tackle cancer.
Diversifying Data
As precision oncology advances, it is essential to ensure that its benefits are accessible to all patients. All constituents invested in public health must come together to ensure that institutions serving historically underserved populations and under-resourced communities have the infrastructure, including access to advanced technologies such as the latest DNA and RNA sequencing techniques, that is needed for proper implementation of precision medicine.
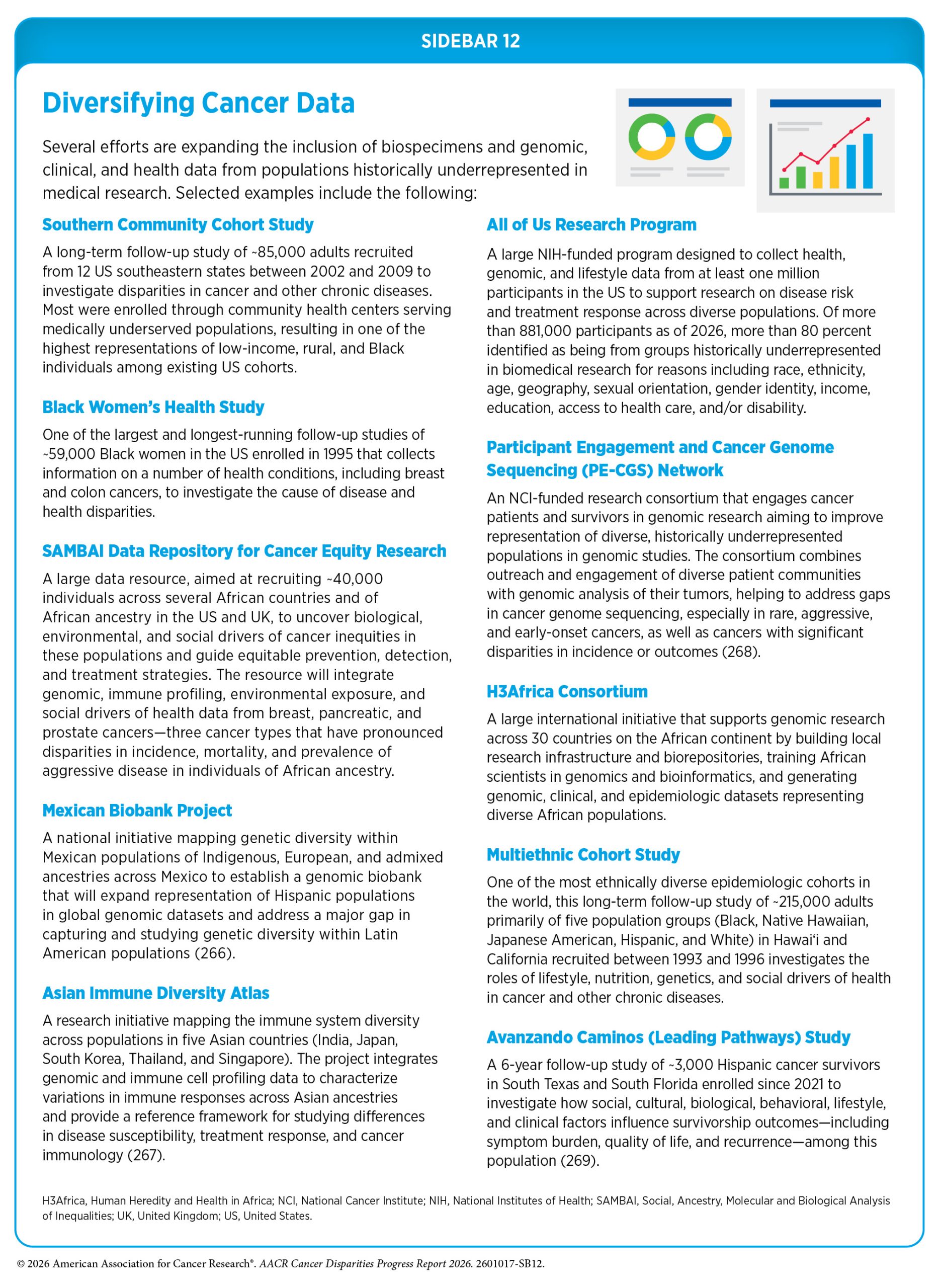
Unfortunately, much of the current information fueling advances in precision medicine is derived from individuals of European ancestry. The underrepresentation in cancer clinical studies of individuals from diverse population groups, with varied sociodemographic backgrounds, and who are medically underserved undermines the broad impact of precision medicine. Integrating insights into how genetic differences arise and vary across populations, together with more comprehensive references of human genetic variation generated through pangenomes (see Genetic Alterations) and diverse global biobanks, is essential to addressing long-standing biases in cancer genomics and ensuring that precision medicine benefits all populations. Several ongoing initiatives are aimed at diversifying cancer-related datasets and incorporate racial, ethnic, ancestral, and social and environmental variables in both research and clinical implementation (see Sidebar 12).
As one example, the AACR Project GENIE® (Genomics Evidence Neoplasia Information Exchange) has sequenced tumors from over 227,000 patients across 20 leading cancer centers in the United States, Canada, Europe, and Asia, 11 percent of whom are from underrepresented racial and ethnic groups (270)American Association for Cancer Research. AACR Project GENIE®. Accessed: March 31, 2026. . Researchers are already using this database to address gaps in knowledge about cancer biology and the genetic changes observed in these underrepresented and underserved populations (218)Jain S, et al. (2024) JCO Precis Oncol, 8: e2400223. (222)Wen W, et al. (2025) Cancer Epidemiol Biomarkers Prev, 34: 2208. .
To advance the science of cancer disparities, researchers must integrate biological data with information on structural and SDOH that influence cancer development and outcomes. Several research initiatives are helping address this by examining how inherited genetics, tumor biology, and social and environmental exposures interact in populations historically underrepresented in medical research. The RESPOND (Research on Prostate Cancer in Men of African Ancestry: Defining the Roles of Genetics, Tumor Markers and Social Stress) study evaluates how exposure to stress over a lifetime, inherited susceptibility, and tumor characteristics contribute to the disproportionately high burden of prostate cancer among men of African ancestry.

Similarly, the ENLACE study, which is a part of the Participant Engagement and Cancer Genome Sequencing Network (see Sidebar 12), is focused on understanding the genetic and environmental factors influencing CRC risk in Hispanic individuals, including in patients such as Alejandro (Alex) Valdez. This study integrates genetic testing—including evaluation of hereditary cancer syndromes such as Lynch syndrome—with characterization of tumor mutations and epidemiologic and clinical data to better understand cancer risk and outcomes in this population.
In pediatric oncology, new opportunities are also emerging to better understand disparities in outcomes through the integration of biological and social data collected within clinical trials. Several Children’s Oncology Group trials have integrated biospecimen collection alongside detailed parent- or caregiver-reported information on demographic, social, behavioral, and environmental factors. This integration creates an unprecedented data resource, enabling researchers to link biological characteristics with SDOH and examine how biological, clinical, and social factors interact to influence outcomes and drive disparities in pediatric cancer (271)Jones E, et al. (2026) JAMA Netw Open, 9: e260419. .
Leveraging Technology
Technological advances are also transforming how researchers generate and interpret cancer data, creating new opportunities to address gaps in knowledge about cancer disparities. Advances in DNA and RNA sequencing technologies are enabling comprehensive genomic profiling of tumors and expanding the identification of actionable diagnostic and therapeutic targets. However, because these tools are largely developed and validated using datasets derived from individuals of European ancestry, the interpretation of genomic findings can be less accurate for individuals from other ancestral backgrounds. To address this gap, researchers are evaluating approaches to improve the performance and clinical interpretation of genomic profiling tools across more diverse populations (272)Lee JY, et al. (2025) NPJ Precis Oncol, 9: 347. (273)Clavell-Revelles P, et al. (2025) Nat Commun, 16: 10194. .
Researchers are also using innovative research models and powerful gene editing tools to better understand factors influencing cancer development and identify novel treatments. Two such approaches include functional genetic screening, which can use gene editing tools to systematically identify genes that drive cancer development or influence response to therapy, and patient-derived tumor organoids—three-dimensional models grown from a patient’s tumor cells (see Sidebar 9). Researchers have recently combined gene editing technology with organoids derived from women of African ancestry with breast cancer to identify potential targets for combination therapy that may be more effective in this population (196)Madorsky Rowdo FP, et al. (2025) Cancer Res, 85: 551. . This highlights progress in diversifying cancer research models and leveraging functional genomic approaches to accelerate discoveries that may improve outcomes for patients historically underrepresented in cancer research.
Emerging technologies, such as liquid biopsy and artificial intelligence (AI), have the potential to transform cancer research and patient care across the cancer care continuum. Liquid biopsy—a minimally invasive technique that analyzes cancer-derived material in blood or other body fluids—offers real-time insight into a patient’s tumor, enabling early cancer detection, treatment selection and response monitoring,
and prediction of disease progression or recurrence (274)American Association for Cancer Research. AACR Cancer Progress Report 2025. Accessed: March 31, 2026. . If implemented equitably, liquid biopsy approaches may expand access to molecular testing and precision oncology by reducing accessibility barriers, as these methods are less invasive and more flexible than traditional tissue biopsy (275)Phillip G. Febbo et al. (2024) JCO Precis Oncol 8, e2300382. .
Advances in AI are accelerating basic research discoveries, improving early detection, enhancing diagnostics, streamlining drug development, supporting clinical decision-making, and increasingly aiding cancer disparities research. For example, studies have shown AI-driven analyses can uncover underlying differences in biological features in tumors from Black and White women with breast and endometrial cancers that may influence disease progression, leading to disparities in outcomes (276)Abdilleh K, et al. (2025) Clin Breast Cancer, 25: e301. (277)Azarianpour S, et al. (2025) NPJ Precis Oncol, 9: 203. .
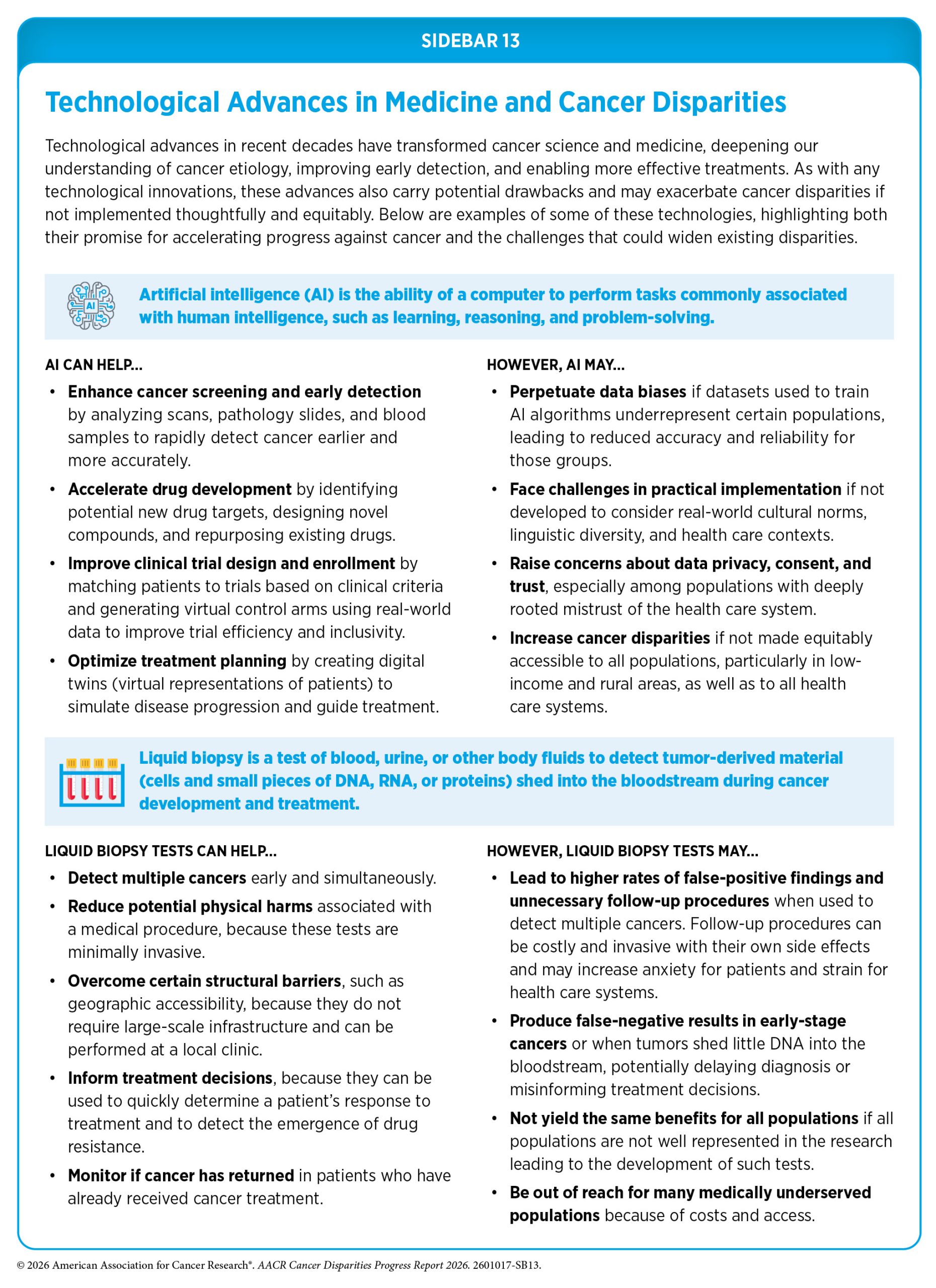
However, if not carefully developed and implemented, these emerging technologies may not benefit all populations equally. Biases in the datasets used to train AI models, limited representation of diverse populations in studies validating liquid biopsy assays, and unequal access to these technologies may unintentionally worsen cancer disparities (see Sidebar 13). It is vital that all stakeholders remain mindful of the potential drawbacks of emerging technologies and take deliberate steps to ensure that they are implemented equitably and accessible for all populations.
AI models can exhibit performance disparities across demographic groups, raising concerns about fairness. In this context, unfairness or bias refers to differences in AI model performance or outcomes across population groups. A recent study found that pathology interpretation models show performance disparities across patient groups classified by race, gender, and age, but these disparities could be mitigated by deliberate algorithm design and fairness-aware training that can help ensure AI-based cancer diagnostics perform equitably across diverse populations (278)Lin SY, et al. (2025) Cell Rep Med, 6: 102527. .
Researchers are also working to diversify the genomic data that underpin many AI-driven precision medicine tools which currently overrepresent individuals of European ancestry, thus limiting the reliability of these tools for populations with different genetic ancestries. To address this, initiatives across Latin America and the Caribbean are developing more inclusive, AI-ready datasets that better capture the genetic and cellular diversity of populations historically underrepresented in biomedical research. This effort aims to ensure that emerging computational tools—such as virtual cells, digital twins, and AI-driven drug discovery models—can more accurately predict disease biology and treatment responses across populations (279)Maracaja-Coutinho V, et al. (2026) Nat Rev Mol Cell Biol, 27: 1. .
AI is also being leveraged to address structural barriers that contribute to inequities in cancer care. For example, researchers have designed a community-oriented, patient-empowering, cloud-based digital health platform supported by AI that brings together medical institutions, religious and spiritual leaders, Black and Indigenous communities, and educators with the goal of expanding access to cancer prevention, diagnosis, and treatment services for underserved communities. This platform integrates telehealth services, AI-assisted decision support tools, community-based health hubs, and mobile health applications to overcome geographic, socioeconomic, and technological barriers that often limit access to care (280)Ngwa W, et al. (2024) Nat Med, 30: 2388. .
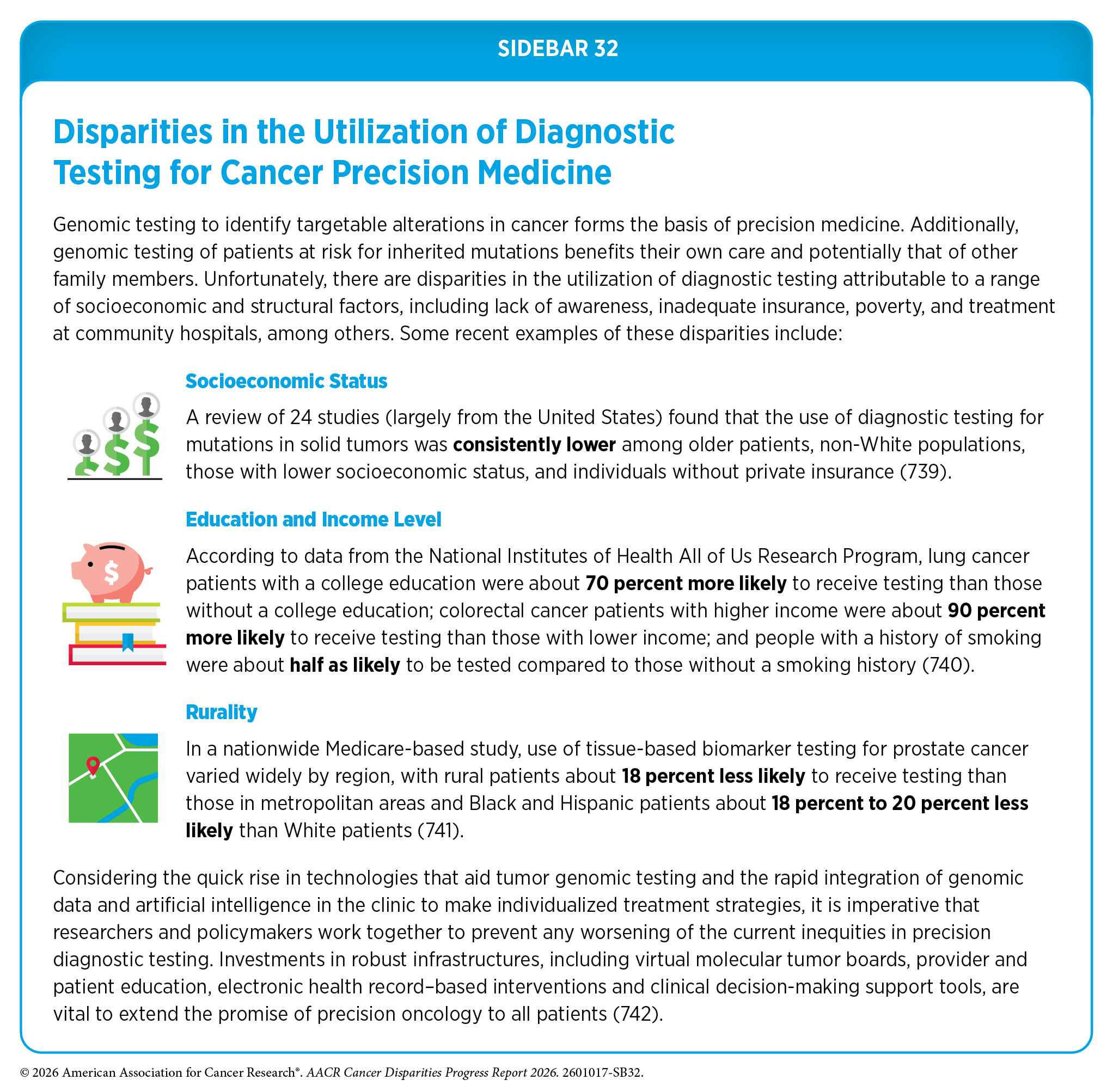
Precision medicine holds great promise to improve cancer outcomes, but key questions remain about the cost effectiveness of molecular profiling and its benefits for individuals across diverse populations (281)van Schaik LF, et al. (2025) JAMA Netw Open, 8: e2548538. (282)Arora K, et al. (2025) JAMA Oncol, 11: 310. (283)Davis MB, et al. (2025) Cancer Cell, 43: 619. . Additionally, disparities in the access and utilization of these services, with lower uptake among underrepresented racial and ethnic groups and underserved populations, further limit its impact (see Sidebar 32). Ensuring that diverse populations are proportionally represented in the development of emerging technologies, are included in clinical studies, and have access to molecular testing and new therapies is essential to realizing the full potential of precision medicine for all populations.
Next Section: Disparities in the Burden of Modifiable Behavioral Cancer Risk Factors Previous Section: Understanding And Addressing Drivers of Cancer Disparities