- Funding for Research and Programs That Address Cancer Disparities
- Coordination of Health Disparities Research and Programs Within the Federal Government
- Policies to Support Health Disparities Research
- Policies to Promote an Inclusive Workforce
- Policies to Address Disparities in Cancer Prevention
- Policies and Regulations to Reduce the Disparate Harms of Tobacco Products
- Policies to Promote Environmental Justice
- Policies to Address Disparities in Cancer Screening and Follow-up Care
- Policies to Address Disparities in Clinical Research and Care
- Improving Representation in Clinical Trials
- Improving Access to High-quality Cancer Care
- Supporting Patient Navigators and Community Health Workers
- Leveraging AI and Digital Health to Address Disparities
Overcoming Cancer Disparities Through Science-Based Public Policy
In this section, you will learn:
- Sustained and robust investment in federal agencies and programs is fundamental to addressing cancer disparities.
- Promoting an inclusive workforce is essential for cancer research progress to benefit all populations.
- Addressing disparities in cancer screening and follow-up care is critical to reducing cancer burden and deaths.
- Encouraging broader representation in clinical research will help ensure safe and effective cancer therapeutics across populations.
Contents
Despite decades of advances in the prevention, early detection, and treatment of cancer, not all communities and populations have benefited equally from scientific progress. Disparities across the cancer care continuum and in research remain persistent challenges that disproportionately affect certain populations, driven by a complex interplay of social drivers of health (SDOH), structural inequities, environmental exposures, and biological factors. Overcoming cancer disparities and achieving health equity requires collaborative and multidirectional efforts from all stakeholders in the cancer care and research ecosystem, including government, the academic community, health care systems, insurance companies, and other organizations. From expanding access to precision prevention and screening to strengthening clinical trial diversity and addressing SDOH, science-based public policy has the power to translate innovation into measurable reductions in cancer burden for historically marginalized populations. Achieving high-quality cancer outcomes for all requires sustained investment in research to understand and reduce cancer disparities, dedicated support for inclusive data systems, and an overall commitment to implement evidence-based programs and policies that address barriers to care. This section focuses on federal initiatives and science policy solutions to reduce cancer disparities.
Funding for Research and Programs That Address Cancer Disparities
Federal funding for Department of Health and Human Services (HHS) agencies, including the National Institutes of Health (NIH), the National Cancer Institute (NCI), the Centers for Disease Control and Prevention (CDC), and the Centers for Medicare & Medicaid Services (CMS), as well as for the United States (US) Food and Drug Administration (FDA) and other agencies, is crucial for advancing our understanding of cancer disparities and developing effective mitigation strategies.
NCI, which leads the federal government’s cancer research enterprise, is strongly committed to reducing cancer disparities (1034)National Cancer Institute. NCI Center to Reduce Cancer Health Disparities (CRCHD). Accessed: March 31, 2026. . The NCI Center to Reduce Cancer Health Disparities (CRCHD) was founded in 2001 to help reduce the unequal burden of cancer among diverse populations. The center provides expert advice on policy, participates in strategic planning to strengthen cancer disparities research, leads NCI’s training efforts to increase diversity and representation in the cancer research workforce (see Disparities in the Cancer Training Pathway and Cancer Research and Care Workforce), and supports basic, clinical, translational, and population disparities research. CRCHD currently offers funding opportunities to investigate biological factors contributing to cancer disparities across racially and ethnically diverse populations and oversees programs that expand scientific partnerships between institutions serving underserved communities and NCI-designated cancer centers, provide opportunities for scientific training, and strengthen community partnerships to improve cancer screening (see Sidebar 41).
NCI also supports a wide range of other initiatives that focus on understanding and addressing cancer disparities. NCI conducts, funds, and coordinates large research studies on the biology behind disparities and the complex factors that shape unequal cancer outcomes across populations. Additionally, the National Institute on Minority Health and Health Disparities (NIMHD) within NIH helps set the federal health disparities research agenda and leads initiatives to address health disparities and improve minority health. NIMHD’s statutory mandate includes planning, reviewing, coordinating, and evaluating disparities research activities across NIH institutes and centers, as well as supporting a broad portfolio of investigator-initiated grants, centers of excellence, and workforce development programs aimed at understanding and addressing health disparities (1035)National Institute of Minority Health and Health Disparities. About. Accessed: March 31, 2026. . For example, NCI, NIMHD, and the Prostate Cancer Foundation jointly support a large study on prostate cancer called RESPOND (Research on Prostate Cancer in Men of African Ancestry: Defining the Roles of Genetics, Tumor Markers, and Social Stress), which investigates environmental and genetic factors contributing to the higher burden of aggressive prostate cancer among Black men. This multilevel study, initially funded in 2018, is also now incorporating newer technology, including artificial intelligence (AI) (1036)Keck School of Medicine of USC. Researchers to utilize $7.6M and the latest technology to better understand prostate cancer predictors. Accessed: March 31, 2026. .
Prior to 2025, federal agencies were expanding cancer disparities research programs and implementing new initiatives aimed at improving health outcomes across populations. However, since January 2025 there have been challenges in the federal funding landscape for cancer disparities and a shift in priorities, including the cancellation of many NIH-wide efforts that were focused on addressing disparities. For example, the NIH Common Fund Transformative Research to Address Health Disparities and Advance Health Equity program supported innovative and interdisciplinary projects that address SDOH and advance novel interventions; however, no new funding opportunities have been available since 2024 (1037)NIH Common Fund. Transformative Research to Address Health. Accessed: March 31, 2026. . Likewise, the NIH Community Partnerships to Advance Science for Society (ComPASS) program, launched in 2023 with a promised investment of $400 million over 10 years, was terminated in early 2025, halting many active and ongoing projects as well as archiving its website (1038)NIH Common Fund. Community Partnerships to Advance Science for Society (ComPASS). Accessed: March 31, 2026. . ComPASS was intended as a community-led research initiative to address structural factors causing health disparities and had just completed initial planning phases to support Community-led Health Equity Structural Interventions.
Coordination of Health Disparities Research and Programs Within the Federal Government
Effective coordination of health disparities research and between programs across the federal government is critical to advancing cancer health equity and reducing inequities in cancer incidence, access to care, and mortality. HHS agencies including NIH, NCI, and CDC play key roles in strategic planning for disparities research and in forming inter-agency partnerships to align policies, address barriers, and promote health equity.
At NIH, NCI primarily coordinates cancer disparities research through CRCHD, which maintains resources for cancer disparities researchers, including a directory of more than 250 NCI-supported tools and services (1039)National Cancer Institute. Resources for Cancer Disparities Researchers. Accessed: March 31, 2026. . CRCHD National Outreach Network (NON) is a program designed to reduce cancer disparities among underserved populations by adding specialized Community Health Educators to NCI-designated cancer centers to deliver culturally tailored cancer education, prevention, and screening information to local communities (1040)National Cancer Institute. National Outreach Network. Accessed: March 31, 2026. . Beyond CRCHD, the NCI Community Oncology Research Program (NCORP) is a national network designed to bring clinical research studies to individuals in their own communities. The NCORP network is composed of 7 research bases, 32 community sites, and 14 minority and underserved community sites whose patient populations include at least 30 percent racial and ethnic minority individuals or rural residents (1041)National Cancer Institute. The NCI Community Oncology Research Program (NCORP). Accessed: March 31, 2026. .
At HHS, several offices focus on health disparities policy alignment as well as serve as focal points for cross-cutting program coordination. The Office of Minority Health provides leadership, resources, and coordination to improve the health of racial and ethnic minority populations and eliminate health disparities (1042)US Department of Health and Human Services. Office of Minority Health. About the Office of Minority Health. Accessed: March 31, 2026. . The Healthy People 2030 initiative, led by the Office of Disease Prevention and Health Promotion, sets national objectives for advancing health equity and specifically prioritizes eliminating health disparities, increasing health literacy, and addressing SDOH (1043)Healthy People 2030. Social Determinants of Health. Accessed: March 31, 2026. . CDC operates many public health programs to reduce cancer disparities and improve population health. CDC’s Division of Cancer Prevention and Control (DCPC) works to reduce cancer disparities and strengthen prevention and control efforts through grants to state and local health departments and other initiatives (see Sidebar 42).
While the federal government continues to invest in health disparities research and infrastructure to support disparities science, the federal landscape for coordinating health disparities research and programs has undergone substantial disruption since 2024. Widespread removal of “health equity” and “social determinants of health” language from federal government programs and policies threatens the ability to accurately measure causes of disparities, coordinate disparities research, and address the root causes of cancer disparities. For instance, CMS has proposed removing key disparity-related metrics from major programs, including the Health Equity Index reward factor in Medicare Part C and D Star Ratings (1051)McDermott+. CMS releases 2027 policy and technical changes to Medicare Advantage and Part D proposed rule. Accessed: March 31, 2026. , and dropped the previously mandatory health equity plans in the Enhancing Oncology Model (1052)Mary C (2025) Evidence-Based Oncology, 31: SP248. HHS proposals also include major department restructuring that would consolidate offices with a health disparities focus into the new Administration for a Healthy America, eliminate discretionary funding for health equity, and cut many offices, programs, and initiatives with a health equity focus (1053)US Department of Health and Human Services. Fiscal Year 2026. Budget in Brief. Accessed: March 31, 2026. .
Policies to Support Health Disparities Research
For all Americans to have the healthiest lives possible, a policy environment that extends beyond federal investment to include sustained support from state and local governments, private foundations, academic institutions, and community-based organizations is essential to ensure that all communities are adequately represented in research and treatment. Efforts that strengthen research infrastructure, promote data sharing and the return of results, and incentivize cross-sector collaboration are essential to advancing cancer disparities research. By fostering inclusive research ecosystems and supporting investigators at all career stages, these policies help generate the evidence needed to inform cancer prevention, diagnosis, and treatment strategies across populations.
Encouraging a Return of Results (ROR) Policy
An essential component of equitable cancer disparities research is the responsible and transparent return of research results (ROR) to participants. Beyond fulfilling an ethical obligation to respect participants and acknowledge their contributions to science, returning individual and aggregate findings can build trust, increase research engagement among historically underrepresented groups, and help ensure that the benefits of discovery are shared fairly across diverse populations. A growing body of evidence supports that most participants value receiving their data, and that ROR can enhance willingness to participate in future research and strengthen trust in scientific institutions (1054)Kent DA, et al. (2024) J Clin Transl Sci, 8: e126. . However, barriers to ROR include socioeconomic determinants such as digital inequity, low health literacy, and other individual characteristics (1055)Phung L, et al. (2024) HGG Adv, 5: 100346. . Recent studies underscore how ROR strategies rarely account for historically marginalized populations and their unique barriers and emphasize how policy frameworks to foster participant-centered approaches are needed to ensure equitable access and advance health equity in ROR (1056)Idnay B, et al. (2025) BMJ Open, 15: e107270. . Embedding plans for ROR into study design and funding mechanisms, informed by participant preferences and community needs, will foster transparency and partnership with minority and underserved populations as well as help reduce cancer disparities.
Collaborative Resources to Advance Disparities Research
In addition to federal investments, a growing ecosystem of collaborative resources has emerged to support cancer disparities research through diverse mechanisms, helping foster innovation, community engagement, and workforce development. Nonprofit organizations and private foundations provide grants for cancer disparities research as well as career development. For example, the Cancer Health Research Centers (CHERCs) program offers 4-year, multi-million dollar grants to create research centers that directly address cancer disparities and support collaborative research partnerships tailored to local and regional community needs (1057)American Cancer Society. RFA: Cancer Health Research Centers (CHERCs). Accessed: March 31, 2026. . In addition to these larger awards, community-focused programs and grants exist to support local projects aimed at reducing disparities in cancer prevention, screening, and early detection, including initiatives in rural and underserved populations (1058)Prevent Cancer Foundation. Cancer Prevention and Early Detection Community Grants. Accessed: March 31, 2026. . Federal support for these initiatives are supported by proposed legislation like the Mammography Access for Veterans Act, introduced by Congressman Glenn “GT” Thompson, which work to address the intersection of rural and veteran populations. Furthermore, fellowship and career support mechanisms like the AACR Cancer Disparities Research Fellowship, which provides sustained salary support for postdoctoral investigators studying cancer disparities, help early-career investigators establish career paths in the field (1059)American Association for Cancer Research. AACR Cancer Disparities Research Fellowship. Accessed: March 31, 2026. . Collectively, these resources broaden the landscape of support for cancer disparities research and interventions as well as investigators, enabling tailored, community-responsive science that sustains the field.
At the state and local level, public health departments are leveraging funding to launch and maintain programs targeting screening and navigation barriers in underserved populations to directly address disparities in access to early diagnosis and care. For example, CDC has partnered with NYC CONNECT (New York City Cancer Outreach Network in Neighborhoods for Equity and Community Translation) to increase overall screening access for community-clinical centers. This partnership works with the New York University (NYU) School of Medicine, the Food Bank for New York City, and other community-stakeholders to see how to best increase screening rates for breast, cervical, and colorectal cancers in the NYC area and, in turn, share those resources with other communities (1060)NIH RePROTER. DP21-003 NYC Cancer Outreach Network in Neighborhoods for Equity and Community Translation. Accessed: March 31, 2026. .
Policies to Promote an Inclusive Workforce
A cancer care and research workforce that reflects the diversity of all patients is key to advancing scientific and health outcomes for Americans of all racial, ethnic, socioeconomic, and geographic backgrounds (see Disparities in the Cancer Training Pathway and Cancer Research and Care Workforce). Over the past few decades, NIH has instituted a range of programs aimed at increasing diversity and inclusivity in the biomedical research workforce. In 2014, NIH established the Division of Biomedical Research Workforce (DBRW) within the Office of Extramural Research (1061)National Institutes of Health Grants & Funding. Division of Biomedical Research Workforce. Accessed: March 31, 2026. . This division was tasked with using in-depth research to guide and implement long-term policies and extramural programs focused on training and career development for a more inclusive biomedical research workforce. Additionally, the Division of Training Workforce Development and Diversity within the National Institute of General Medical Sciences is committed to guiding underrepresented trainees through a variety of programs at all career development stages (1062)National Institute of General Medical Sciences. Research Training. Accessed: March 31, 2026. .
To aid researchers from underrepresented backgrounds in transitioning to the next stages of their careers, NIH offered several programs. In 1992, all NIH institutes and centers began offering diversity supplements to support individuals from underrepresented groups or disadvantaged backgrounds to engage in research. Additionally, most institutes and centers provide K awards to help scientists from diverse backgrounds enhance their careers. Offered through partner institutions, the Institutional Research and Academic Career Development Award (IRACDA) program combines a traditional postdoctoral research experience with additional teaching and mentorship opportunities that have generally benefited women and individuals from diverse backgrounds.
However, support for these programs changed significantly when the Trump administration issued a pair of executive orders directing federal agencies to end programs and grants supporting underrepresented populations on the basis of federal anti-discrimination law. Consequently, many NIH programs created to support a more inclusive research workforce were eliminated, and their webpages deactivated, such as the National Research Mentor Network. Findings from a 2026 AACR survey suggest that grant terminations have significantly impacted investigators across all career stages.
AACR Survey of Cancer Disparities Researchers: View the ResultsAccording to a recent study, the administration terminated 181 NCI-awarded grants totaling more than $640 million, with an estimated $317 million in unspent research funds (1063)Haque W, et al. (2026) JAMA Oncol, 12: 109. . While these terminations affected early-career investigators of all backgrounds, the impact fell disproportionately on female researchers (1004)Oliveira DFM, et al. (2026) Proc Natl Acad Sci U S A, 123: e2527755123. . The disruptions also coincided with a decline of more than 2,000 doctoral enrollments in the life and biomedical sciences across the United States from fall 2024 to fall 2025. While initiatives to diversify the medical workforce and study health disparities have seen significant disruption, educational programs are now also facing drastic change. Under pressure from the Trump administration, the leading medical school accreditation body in the United States removed the requirement for schools it accredits to teach about health disparities (1064)STAT News. As political pressure mounts, medical school accreditor drops requirement to teach about health equity. Accessed: March 31, 2026. .
While increased funding for extramural grants would provide more opportunities for early-stage investigators—and, by extension, more researchers from underrepresented backgrounds—it is not a substitute for the programs and initiatives specifically focused on creating a more inclusive biomedical research workforce. Congress should therefore consider ways to statutorily protect existing programs with tangible, evidence-based benefits for the biomedical research workforce. For example, CRCHD’s Intramural Continuing Umbrella of Research Experiences (iCURE) program has supported more than 3,000 scholars across the United States since its founding, providing mentored research training at every career stage from undergraduate through early-stage faculty (1065)National Cancer Institute. Increasing Diversity in the Biomedical Workforce. Accessed: March 31, 2026. . Additionally, the NCI Diversity Supplement Program awarded 429 diversity supplements between 2005 and 2020. Codifying key programs like these in statute would ensure their long-term stability and protect them from possible elimination in the future. Congress should also consider legislative action to restore programs eliminated by the administration in 2025.
Given that disruptions to early-career investigators fell disproportionately on researchers from underrepresented backgrounds, Congress should also direct NIH to restore its early-career grant award rates to their 2024 levels, as well as establish bridge funding mechanisms to ensure continuity of research in the event of future administrative disruption. Similar approaches have been adopted by scientific societies, which have expanded bridge funding programs in response to the 2025 NIH funding disruptions (1066)American Society of Hematology. ASH Significantly Expands Bridge Grant Eligibility. Accessed: March 31, 2026. .
Policies to Address Disparities in Cancer Prevention
Cancer disparities, including those related to cancer incidence, are driven by a complex set of interrelated causes, including SDOH (1043)Healthy People 2030. Social Determinants of Health. Accessed: March 31, 2026. . Effective cancer prevention depends not only on scientific advances but also on public policies that ensure those advances reach all communities equitably. Policies that expand access to evidence-based prevention services, reduce environmental and behavioral risk factors, and address SDOH play a critical role in narrowing disparities in cancer incidence. Aligning prevention strategies with the needs of populations that experience disproportionate cancer burdens will help ensure all individuals benefit from progress in cancer prevention.
Policies and Regulations to Reduce the Disparate Harms of Tobacco Products
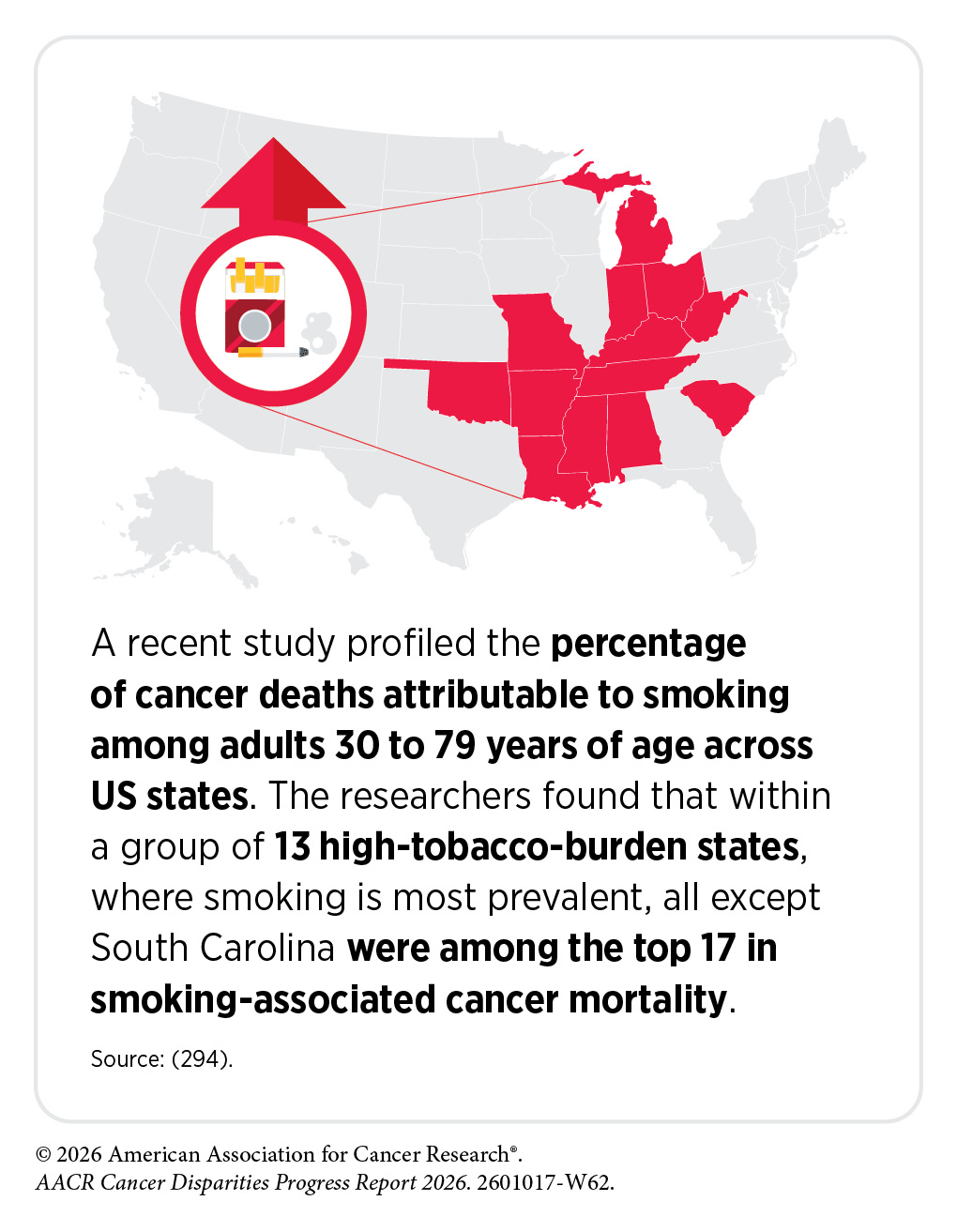
Evidence continues to demonstrate that tobacco smoking causes at least 18 different types of cancer, is the leading cause of premature mortality, accounting for 30 percent of all cancer deaths, and is the top modifiable risk factor for cancer-related deaths (see Disparities in the Burden of Modifiable Behavioral Cancer Risk Factors). Reducing tobacco use is therefore pivotal for improving overall health outcomes. Fortunately, smoking prevalence among adults in the United States has declined to an all-time low at 9.9 percent, thanks to policies such as smoke-free laws, tobacco taxes, advertising restrictions, evidence-based smoking cessation programs, and awareness campaigns (293)Agaku I, NEJM Evidence, 0: EVIDpha2500339. .
Unfortunately, decreases in smoking prevalence have not been equal across all populations, with disparities continuing to exist based on race, ethnicity, socioeconomic status, education, sexual orientation, gender identity, occupation, geography, behavioral health status, and disability status. In November 2024, the US Surgeon General released a report titled Eliminating Tobacco-Related Disease and Death: Addressing Disparities, which took stock of these issues and identified paths toward eliminating the burden of death and disease caused by tobacco use for all (1067)US Department of Human and Health Services. Eliminating Tobacco-Related Disease and Death: Addressing Disparities—A Report of the Surgeon General. Accessed: March 31, 2026. . While many of the national-level solutions outlined in the Surgeon General’s report, including continued funding for the CDC National and State Tobacco Control Program and the federally funded Tips From Former Smokers awareness campaigns, have recently faced increased instability or been cut entirely, it is encouraging to see that many efforts to track and reduce smoking and other tobacco-related disparities remain active.
Due in part to historical predatory marketing (1068)American Heart Association. Report: Tobacco industry continuing decades-long targeting of Black communities, women, youth with menthol products. Accessed: March 31, 2026. , Black communities experience higher rates of tobacco use when compared to other racial and ethnic groups and die from smoking-related diseases at a higher rate than Hispanic and White populations (1069)Centers for Disease Control and Prevention. African American Communities Experience a Health Burden From Commercial Tobacco. Accessed: March 31, 2026. . In particular, the tobacco industry has aggressively targeted Black communities with menthol cigarette advertising and this has resulted in long-standing disproportionately high use among this population, with CDC reporting in 2024 that 73 percent of Black adults who smoke used menthol cigarettes (1070)Wickham RJ (2020) Nicotine Tob Res, 22: 1676. (1071)VanFrank B, et al. (2024) MMWR Morb Mortal Wkly Rep, 73: 633. . Other populations, including lesbian, gay, bisexual, transgender, queer or questioning, and other (LGBTQ+) individuals, experience similar disproportionate targeting through advertisements and have higher menthol cigarette use (297)Bandi P, et al. (2025) Tob Control. . This is particularly troubling, as menthol cigarettes are known to be more addictive than traditional tobacco flavored cigarettes, with significantly more individuals who smoke menthol cigarettes wanting to quit than those who smoke non-mentholated cigarettes (1070)Wickham RJ (2020) Nicotine Tob Res, 22: 1676. (1071)VanFrank B, et al. (2024) MMWR Morb Mortal Wkly Rep, 73: 633. . Further, a recent large study of nearly one million individuals found that among people who were able to quit smoking, those who smoked menthol cigarettes experience higher all-cause mortality because of increased risks of heart disease (297)Bandi P, et al. (2025) Tob Control. .
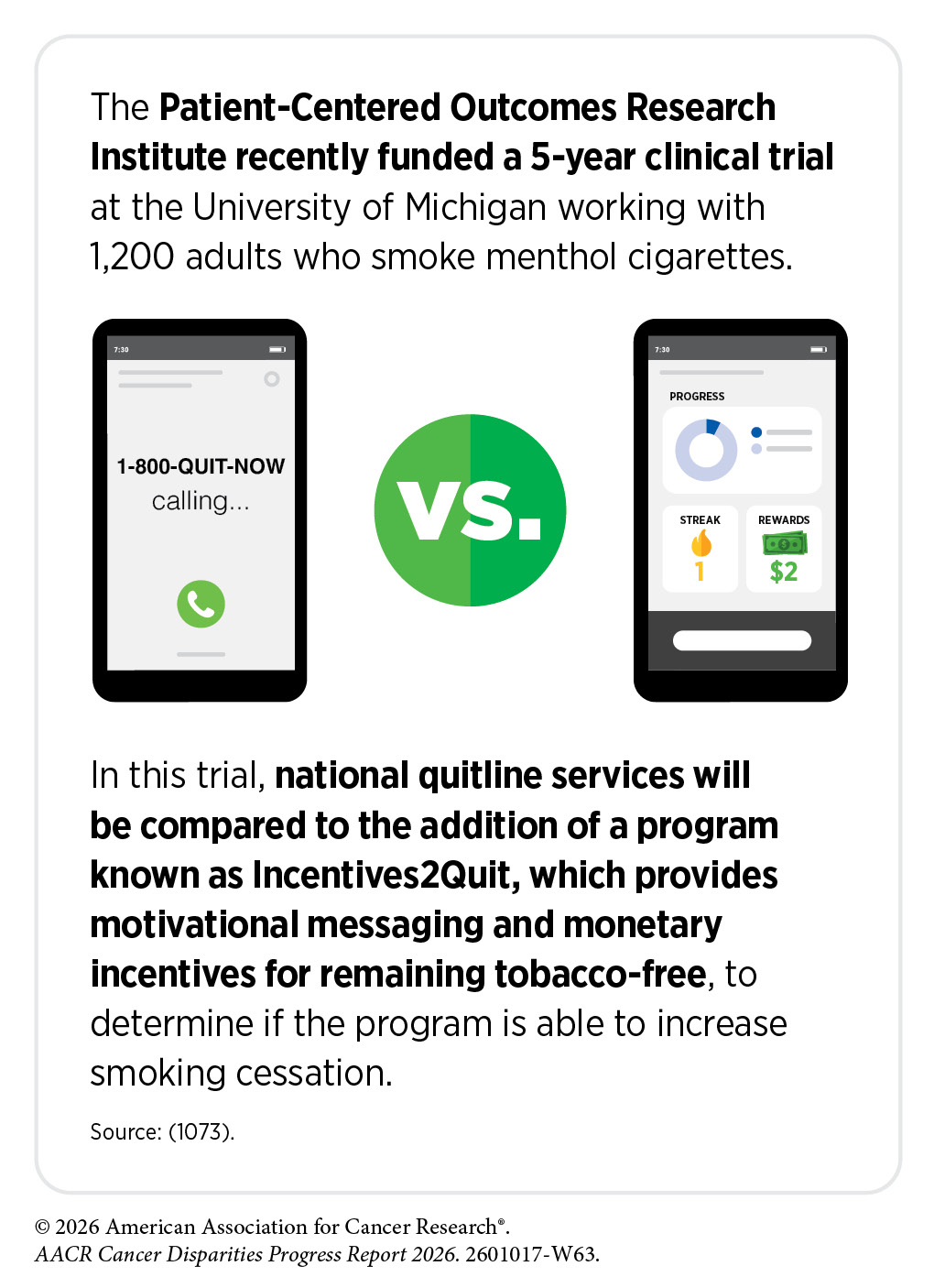
While other cigarette flavors were banned in 2009 as part of the Tobacco Control Act, FDA’s 2022 proposed ban on menthol as a characterizing flavor in cigarettes was withdrawn in 2025. However, organizations such as the Patient-Centered Outcomes Research Institute (PCORI), a US-based nonprofit that funds comparative clinical effectiveness research to help patients, caregivers, and clinicians make better-informed health care decisions, continue to fund studies specifically aimed at determining how to best aid those who smoke menthol cigarettes in quitting. In addition, in communities experiencing high levels of poverty, residential segregation, and chronic stress, individual-level cessation strategies alone have often been insufficient. To address these concerns on a community level, CDC has partnered with Cicatelli Associates, Inc., to find practical ways to empower tobacco cessation in rural areas like Jackson, Mississippi (1072)NIH RePORTER. Reducing Cancer Disparities within the Black community in Jackson, MS through Community-Led Tobacco-Related Social Norm Change. Accessed: March 31, 2026. . This partnership aims to expand access to cessation resources at the community level, including tobacco-free environments and anti-tobacco social media campaigns.
Novel tobacco products, including flavored e-cigarettes and nicotine pouches, also pose health disparity concerns. Both of these product classes can cause significant health risks, including issues with cardiovascular, lung, and oral health. While a causal link between these products and cancer is not yet clear, some research indicates that dual use of e-cigarettes and traditional cigarettes increases the risk of lung cancer by four-fold compared to only smoking traditional cigarettes (302)Bittoni MA, et al. (2024) J Oncol Res Ther, 9. . Given the proliferation of these products, especially among young people, tracking factors that contribute to their use is imperative to stemming further uptake. Notably, rural youth report higher lifetime use of both nicotine pouches and e-cigarettes, and nicotine pouch sales per capita have been shown to be higher in rural areas compared to urban areas (1074)Han DH, et al. (2025) JAMA Netw Open, 8: e256739. (1075)Xu L, et al. (2026) Int J Drug Policy, 150: 105178. . These trends hold for those with indicators of lower socioeconomic status, such as neighborhood safety and college attendance plan status (1074)Han DH, et al. (2025) JAMA Netw Open, 8: e256739. (1076)Mattingly DT, et al. (2026) Drug Alcohol Depend, 283: 113118. . Addressing these disparities, likely driven in part by differences in exposure to targeted advertising and misinformation, will be key to preventing future youth from experiencing further tobacco-related harms.
While some national-level tobacco programs have been disrupted, state and local programs are making significant progress against tobacco and tobacco-related disparities. For example, a law banning the sale of flavored tobacco products in Denver, Colorado, including e-cigarettes, menthol-flavored cigarettes, and flavored cigars, took effect on January 1, 2026 (1077)Tobacco Free Kids. Denver Voters Uphold Law Ending Flavored Tobacco Sales in Big Win for Kids Over the Tobacco Industry. Accessed: March 31, 2026. . California also continues to lead on these issues at the state and local levels, with policies being implemented in the bay area townships of Tiburon and Ross, where the sale of all tobacco products was recently prohibited with no exemptions (1078)American Lung Association. State of Tobacco Control 2026. Accessed: March 31, 2026. . Greater implementation and continued enforcement of similar policies across all levels of government would reduce disparities in tobacco use and facilitate a transition toward a tobacco-free future.
Policies to Promote Environmental Justice
The term environmental justice refers to efforts that advance the just treatment of all people by ensuring they are protected from disproportionate environmental health risks and can live in a healthy, sustainable environment (1079)US Environmental Protection Agency. Learn About Environmental Justice. Accessed: March 31, 2026. . Racial and ethnic minority populations and other marginalized groups are disproportionately harmed by exposures to environmental carcinogens, including radon, petrochemicals, per- and poly-fluoroalkyl substances (PFAS), and pesticides (118)Kraus NT, et al. (2024) Public Health Nurs, 41: 287. (1080)Lee EK, et al. (2022) Soc Sci Med, 294: 114696. (1081)Egede LE, et al. (2023) Diabetes Care, 46: 667. . In turn, these exposures lead to higher cancer incidence and mortality rates (1082)Zhang L, et al. (2023) JAMA Oncology, 9: 122. . These outcomes are the result of discriminatory policies, including redlining and the construction of polluting industrial facilities and waste disposal sites in marginalized communities (118)Kraus NT, et al. (2024) Public Health Nurs, 41: 287. (1080)Lee EK, et al. (2022) Soc Sci Med, 294: 114696. (1081)Egede LE, et al. (2023) Diabetes Care, 46: 667. .
Historically, the Environmental Protection Agency (EPA) was tasked with implementing initiatives and policies that pursue environmental justice. These initiatives include the National Radon Action Plan (NRAP), a public-private partnership to identify and combat preventable radon exposures (1083)RADONLEADERS.ORG. National Radon Action Plan. Accessed: March 31, 2026. . However, on March 12, 2025, in accordance with the Presidential Action “Ending Radical and Wasteful Government DEI Programs and Preferencing” (1084)The White House. Ending Radical And Wasteful Government DEI Programs And Preferencing. Accessed: March 31, 2026. , the EPA has ceased their environmental justice operations (1085)US Environmental Protection Agency. EPA Terminates Biden’s Environmental Justice, DEI Arms of Agency. Accessed: March 31, 2026. . The agency remains dedicated to reductions of environmental carcinogens, particularly lead exposure in water, which has been classified as a likely human carcinogen (1086)US Environmental Protection Agency. Learn About Lead. Accessed: March 31, 2026. . In October 2025, the EPA issued a final rule that requires lead pipes across the country be replaced with copper pipes over a 10-year time frame (1087)US Environmental Protection Agency. Lead and Copper Rule Improvements. Accessed: March 31, 2026. . While this is a notable step in promoting health equity, rescissions of environmental justice policies are concerning.
Policies to Address Disparities in Cancer Screening and Follow-up Care
Expanding access to and uptake of effective cancer screening is one of the most impactful policy solutions to reduce cancer burden and deaths. Using US population data from 1975 to 2020, NCI estimated that nearly six million cancer deaths were averted, with prevention and screening accounting for roughly 80 percent of the deaths averted across five of the most common cancers (313)Goddard KAB, et al. (2025) JAMA Oncol, 11: 162. . However, even for cancers with effective screening tools, millions of eligible individuals remain unscreened (see Disparities in Cancer Screening for Early Detection). Additionally, despite efforts to increase screening rates, structural and socioeconomic factors continue to drive gaps in access and strongly correlate with persistently low screening rates among disadvantaged populations (1088)Pradhan P, et al. (2025) JAMA Netw Open, 8: e2537905. . These persistent disparities in cancer screening and follow-up care undermine progress in reducing cancer mortality and exacerbate inequities in outcomes for racial, ethnic, and socioeconomically disadvantaged populations as well as rural and frontier populations. Limited access to affordable health care, low health literacy, inadequate patient–provider communication, transportation challenges, and geographic maldistribution of screening facilities and providers are among the barriers that reduce opportunities for timely screening in these populations (521)Gudina AT, et al. (2025) Cancer Epidemiol Biomarkers Prev, 34: 35. (1089)Potter AL, et al. (2024) J Thorac Cardiovasc Surg, 168: 248. . Importantly, delays or failures in follow-up after abnormal screening results are disproportionately concentrated in the same underserved populations, further exacerbating inequities in cancer outcomes (1090)Lepe M (2024) Cancer Cytopathol, 132: 205. (1091)Agenor M, et al. (2024) BMC Womens Health, 24: 362. .
Therefore, policy solutions to reduce disparities in cancer screening and follow-up care must consider structural, socioeconomic, and access-related barriers while also modernizing screening delivery methods. Revising screening eligibility criteria and clinical guidelines to better capture high-risk and underserved populations would dramatically reduce disparities. For example, recent research has highlighted how restrictive eligibility thresholds, particularly for lung cancer screening, exclude certain racial and ethnic minority groups as well as individuals with elevated risk due to socioeconomic factors (1092)Mahmoud MA, et al. (2025) JAMA Netw Open, 8: e2525216. (1093)Li CC, et al. (2024) J Natl Med Assoc, 116: 180. (1094)Young CD, et al. (2025) JAMA Netw Open, 8: e252172. . These findings underscore the need for risk-adapted criteria that incorporate racial, social, and environmental determinants for cancer screening eligibility. In addition, community-based interventions, including mobile screening programs, partnerships with trusted local organizations, and culturally tailored outreach, have demonstrated effectiveness in increasing screening uptake and improving follow-up adherence in underserved populations (1095)Kobrin S, et al. (2026) Health Educ Behav, 53: 44. (1096)Ferrari A, et al. (2025) Public Health Rev, 46: 1607873. . Policies that support implementation of patient navigation programs, which provide individualized support to address logistical and language barriers, are also increasingly recognized as essential tools to ensure equitable access to follow-up care after abnormal screening results.
Addressing financial barriers is another key policy lever to improve screening access and uptake. Expanding insurance coverage for screening and follow-up services, eliminating cost-sharing, and funding population-based outreach programs have been shown to significantly increase screening participation, particularly among disadvantaged populations (1097)Taylor CD, et al. (2024) JAMA Health Forum, 5: e242814. (1098)May FP, et al. (2024) Contemp Clin Trials, 145: 107639. . The Patient Protection and Affordable Care Act (ACA) was a landmark piece of legislation that expanded access to cancer screening through several key provisions, most notably by requiring private insurance plans and Medicaid expansion programs to cover US Preventive Services Task Force (USPSTF)–recommended screening services without patient cost-sharing. This policy change has been associated with measurable increases in screening uptake, particularly for breast and colorectal cancers, and reductions in out-of-pocket costs, with more recent analyses continuing to show sustained gains in early detection and narrowing of some screening disparities (1099)Preston MA, et al. (2024) Cancer Med, 13: e7054. (1100)Maceyko M, et al. (2026) JAMA Network Open, 9: e2554483. . Enactment of the ACA greatly reduced some financial barriers to cancer screenings; however, cost remains a major factor for underserved populations and additional policy-level interventions are needed (163)Hussain MR, et al. (2025) Cancers (Basel), 17. . Medicaid expansion under the ACA has been specifically credited for driving improvements in early detection and survival across populations for many cancers (783)Lyons JM, et al. (2025) Cancers (Basel), 17. (1101)Zhao J, et al. (2026) J Clin Oncol: Jco2501892. (1102)Bergstein A, et al. (2024) Gynecol Oncol, 189: 49. . Importantly, passage of the One Big Beautiful Bill Act of 2025 (H.R.1) rolled back ACA Medicaid expansion and introduced Federal Medicaid eligibility restrictions. One analysis found that these restrictions would cause millions of Medicaid enrollees to lose coverage over a 2-year period and result in hundreds of thousands of missed screenings across breast, colorectal, and lung cancers, likely disproportionately impacting populations already experiencing barriers to care (1103)Shubeck SP, et al. (2026) JAMA Oncol, 12: 319. .
In the past few years, there have been notable successful US policy efforts to address disparities in cancer screening and follow-up care. Integrating self-collection of samples for human papillomavirus (HPV) testing into primary care has been shown as a feasible and potentially transformative strategy to reduce cervical cancer screening disparities (1104)Pratt R, et al. (2024) Prev Med Rep, 38: 102599. (1105)Fokom Domgue J, et al. (2026) JAMA Netw Open, 9: e2558841. . FDA’s approval of an at-home HPV test in 2025 has introduced more accessible screening options that can be completed outside of traditional clinical settings (1106)The ASCO Post. FDA Approves At-Home Self-Collection Device for Cervical Cancer Screening. Accessed: March 31, 2026. . Updated guidelines from the Health Resources and Services Administration (HRSA) designated primary HPV testing, including self-collected samples, as a preferred screening strategy and will require most insurance plans to cover the full continuum of screening without cost-sharing, thereby directly addressing financial and logistical barriers (1107)Health Resources and Services Administration. New Cervical Cancer Screening Guidelines Strengthen Women’s Preventive Health. Accessed: March 31, 2026. . In addition, adoption of the December 2024 draft recommendations from USPSTF to incorporate self-collection methods would further improve screening adherence among populations less likely to engage in clinic-based care (1108)United States Preventive Services Taskforce. Draft Recommendation: Cervical Cancer: Screening. Accessed: March 31, 2026. . Similarly, wider implementation of at-home colorectal cancer screening tests for underserved populations has the potential to reduce disparities and improve access to screening (1109)Brodney S, et al. (2024) Cancer Med, 13: e70040. . Furthermore, effective January 1, 2025, CMS began covering computed tomography colonography (CTC) to screen individuals age 45 or older at average risk for colorectal cancer (1110)Healthcare Administrative Partners. CT Colonography Receives National Coverage. Accessed: . Research indicates that CTC is a cost-effective colorectal cancer screening strategy that enhances screening adherence among Black adults and reduces colorectal cancer disparities (1111)Kao SZ, et al. (2025) Cancer Med, 14: e71290. . Together, these policy approaches represent key strategies to reduce disparities in cancer screening and ensure more timely follow-up care.
Additional federal government and legislative actions have also supported efforts to improve access to cancer screening and follow-up care. USPSTF released updated guidelines in April 2024, recommending that women begin breast cancer screening at age 40 instead of 50, which expands access to no-cost screening for millions to address the rising incidence in younger populations and reduce disparities (1112)United States Preventive Services Taskforce. Recommendation: Breast Cancer: Screening. Accessed: March 31, 2026. . However, USPSTF, which is critical to shaping preventive care and addressing screening disparities, has not met since March 2025 (1113)CNN. The task force that shapes Americans’ preventive care has not met in a year. Doctors now worry it’s being ‘abandoned’ by HHS. Accessed: March 31, 2026. . The Nancy Gardner Sewell Medicare Multi-Cancer Early Detection (MCED) Screening Coverage Act, passed as part of fiscal year 2026 appropriations, will help reduce disparities by allowing Medicare to quickly cover new multi-cancer blood tests and make early cancer screening more affordable and accessible to medically underserved groups who often face barriers to traditional screenings (1114)US Congresswoman Terri Sewell. Rep. Sewell Celebrates House Passage of the Nancy Gardner Sewell Medicare Multi-Cancer Early Detection Screening Coverage Act. Accessed: March 31, 2026. . Proposed legislation includes the Screening for Communities to Receive Early and Equitable Needed Services (SCREENS) for Cancer Act of 2025 (S.1866/ H.R.2381), which would reauthorize and increase funding to $235 million per year for fiscal years 2026–2030 for the National Breast and Cervical Cancer Early Detection Program as well as enhance patient navigation services, outreach to underserved populations, and implementation of evidence-based strategies to increase breast and cervical cancer screening rates. Passage of this bipartisan bill would be instrumental in improving screening access for underserved communities and reducing disparities through improved patient navigation and outreach (1115)Congress.gov. Text – S.1866 – 119th Congress (2025-2026): SCREENS for Cancer Act of 2025. Accessed: Aprill 29, 2026. . Introduced by Congressman Gabe Evans (R-CO) and Congressman Raul Ruiz (D-CA), the Mobile Cancer Screening Act (H.R.4417) is a bill with bipartisan support that would increase the availability of cancer detection services in rural and underserved communities through establishment of a federal grant program to help rural hospitals and health care centers purchase mobile screening units (1116)Congress.gov. H.R.4417 – Mobile Cancer Screening Act. Accessed: March 31, 2026. .
Policy-oriented disparities research continues to reinforce that while access to screening services is necessary, systems of care also require structural interventions that strengthen follow-up procedures, reduce financial barriers, support navigation, and embed metrics to evaluate disparities into screening programs. Legislative and federal policy actions can significantly reduce disparities in cancer screening and follow-up care by evaluating and addressing these factors.
Policies to Address Disparities in Screening for Hereditary Cancer Syndromes
Genetic testing has increasingly been incorporated into clinical practice to identify patients in need of additional screening, stratify risk for developing cancer, and allow for earlier diagnosis and intervention for high-risk tumors. Over 50 hereditary cancer syndromes are known, but genetic testing and screening remain underutilized for cancer prevention and treatment (1117)National Cancer Institute. Division of Cancer Control and Population Sciences. Inherited Cancer Syndromes. Accessed: March 31, 2026. . Importantly, significant disparities persist in adequately identifying at-risk individuals across diverse populations and in optimizing surveillance strategies, as well as access to genetic testing and preventive care for common cancers with known hereditary drivers, such as colorectal and breast cancers (1118)Maria-Alexia P, et al. (2026) Cancer Genet, 302-303: 166. (1119)Duyar-Ayerdi S, et al. (2024) Obstet Gynecol Surv, 79: 673. . Policies to address disparities in screening for hereditary cancer syndromes must prioritize access to genetic testing, genetic counseling, and risk-adapted follow-up care. The Reducing Hereditary Cancer Act (RHCA) (H.R.4752/S.2760) seeks to expand Medicare coverage to cover genetic testing, counseling, and high-risk cancer screenings for individuals with family histories or known hereditary mutations (1120)Congress.gov. Text – H.R.4752 – 119th Congress (2025-2026): Reducing Hereditary Cancer Act. Accessed: March 31, 2026. . Currently, Medicare largely limits coverage of genetic testing to individuals already diagnosed with cancer, creating a critical gap in preventive care that disproportionately affects older adults and exacerbates disparities in early detection. RHCA would help remove financial barriers that currently prevent those with hereditary cancer syndromes from accessing preventive services, particularly in underserved populations. In addition, policy-oriented research has identified implementation models to overcome barriers and employ strategies to engage disadvantaged groups in genetic testing (1121)Leader AE, et al. (2024) BMC Public Health, 24: 2533. . However, additional approaches are needed to embed hereditary cancer screening into broader public health and health system reforms to increase access to genetic testing and follow-up care (1122)Rao ND, et al. (2024) Front Health Serv, 4: 1455365. (1123)Rodriguez NJ, et al. (2023) Clin Gastroenterol Hepatol, 21: 3. These emerging policy efforts highlight a shift toward prevention-focused, risk-stratified screening frameworks that can reduce disparities in hereditary cancer detection if implemented with explicit attention to affordability, access, and delivery.
Policies to Address Disparities in Clinical Research and Care
Improving Representation in Clinical Trials
Improving representation in clinical trials is essential to ensure that advances in cancer therapeutics are safe and effective across populations (see Disparities in Clinical Research and Cancer Treatment). Adequate representation strengthens trust in clinical research, maximizes the generalizability of treatment outcomes, and helps identify potential differences in treatment response across population subgroups, thereby supporting efforts to reduce cancer disparities (1124)National Academies of Sciences, Engineering, and Medicine; Policy and Global Affairs; Committee on Women in Science, Engineering, and Medicine; Committee on Improving the Representation of Women and Underrepresented Minorities in Clinical Trials and Research; Bibbins-Domingo K, Helman A, editors. Improving Representation in Clinical Trials and Research: Building Research Equity for Women and Underrepresented Groups. Washington (DC): National Academies Press (US); 2022 May 17. 2, Why Diverse Representation in Clinical Research Matters and the Current State of Representation within the Clinical Research Ecosystem. . In recent years, policymakers and regulators have advanced efforts to improve representation in clinical research and address long-standing barriers to participation.
Policy and regulatory efforts have emphasized the importance of practical and intentional approaches to improving representation in clinical trials. Over the past few years, FDA has published several guidance documents aimed at improving representation in clinical trials (1125)US Food & Drug Administration. Diversity Action Plans Summary FY 2023 and FY 2024. Accessed: March 31, 2026. . Most recently, the agency issued updated draft guidance that encouraged sponsors of certain clinical studies to prospectively plan for representative enrollment and implement strategies to improve participation in clinical research (591)US Food & Drug Administration. Diversity Action Plans to Improve Enrollment of Participants from Underrepresented Populations in Clinical Studies. Accessed: March 31, 2026. , however this guidance has now been removed due to a change in federal policy. In this June 2024 guidance, FDA recommended sponsors submit plans outlining enrollment goals and strategies to achieve representative participation in clinical studies. Plans were to include enrollment targets across key demographic characteristics, such as age and sex; considerations for socioeconomic status and disability; descriptions and rationale for enrollment goals; strategies for recruiting and retaining patients; and approaches to support broader representation among clinical investigators and study staff.
At the same time, key interested parties across the cancer clinical research enterprise continue to implement strategies to improve representation, including increasing the number of trial sites in community-based oncology settings, adopting decentralized and hybrid trial models, and strengthening partnerships with local communities (1126)Ebrahimi H, et al. (2025) Am Soc Clin Oncol Educ Book, 45: e100052. . FDA has further bolstered these efforts by finalizing a guidance in 2025 that directs sponsors in making trials more representative through broadening eligibility criteria and advancing more accessible study designs to increase enrollment and retention of individuals regardless of background (1127)US Food & Drug Administration. Enhancing Participation in Clinical Trials — Eligibility Criteria, Enrollment Practices, and Trial Designs Guidance for Industry. Accessed: March 31, 2026. . Collectively, these endeavors are helping to reform clinical trial design to better support participation across populations affected by cancer.
In addition, it is also important that clinical research policy frameworks explicitly support the examination of differences in toxicity, relapse, and survival outcomes across diverse populations enrolled in clinical trials. Policies that require or incentivize the collection and stratified analysis of treatment response data can generate actionable evidence on how and why outcomes may differ across groups. This could include supporting the integration of mechanistic and real-world correlates of toxicity and disease progression into trial design, as well as strengthening post-trial analyses that can identify biological, environmental, and system-level contributors to outcome disparities. One analysis found that few oncology clinical trials had curated post-treatment sex comparisons despite clear differences in treatment toxicity and outcomes, demonstrating the importance of evaluating differential therapeutic effects across diverse cohorts (1128)Kammula AV, et al. (2024) Nat Commun, 15: 2608. . Embedding these requirements into funding criteria, regulatory guidance, and trial reporting standards would help ensure that clinical research generates the evidence needed not only to improve representation, but also to advance equitable treatment effectiveness and survival outcomes across all populations.
Improving Access to High-quality Cancer Care
Access to high-quality cancer care plays a key role in shaping cancer outcomes. However, health disparities remain across certain geographic, socioeconomic, and demographic groups. Rural and frontier populations, individuals with limited or no health insurance, and those facing financial barriers are more likely to experience delays in diagnosis, inadequate access to guideline-driven treatment, and suboptimal cancer outcomes (1129)Franks JA, et al. (2023) J Natl Cancer Inst, 115: 530. . Ensuring timely access to comprehensive, high-quality cancer care remains an essential component to reducing cancer disparities.
Geographic disparities remain a considerable barrier to accessing high-quality cancer care, particularly for individuals living in rural and medically underserved areas. These populations often face limited availability of oncology specialists, reduced access to comprehensive diagnostic and treatment services, and longer travel distances to cancer centers. In fact, studies show that individuals with cancer living in rural and frontier areas are nearly four times more likely to cross state lines for chemotherapy services compared to individuals living in urban areas (661)Moen EL, et al. (2025) JAMA Netw Open, 8: e2461021. . Policy solutions aimed at addressing these challenges include expanding telehealth services and ensuring sustained reimbursement for virtual oncology care, aligning cross-state licensure and coverage policies to support remote care delivery, and investing in broadband infrastructure to enable telehealth utilization (1130)Doshi SD, et al. (2024) Cancer J, 30: 8. .
Health insurance coverage is another key determinant of access to quality cancer care. The Social Security Act of 1935 helped establish a system of employment-based health insurance that has contributed to disparities in coverage due to unequal access to job opportunities (4)Wagle NS, et al. (2025) CA Cancer J Clin, 75: 308. . Policy approaches to improve access to health insurance include expanding Medicaid eligibility, strengthening marketplace coverage options, and implementing protections for continuous coverage. Efforts to improve benefit design and reduce out-of-pocket costs, as well as reforms to streamline prior authorization requirements, may further enhance access to quality care (1131)Office of the Assistant Secretary for Planning and Evaluation. Improving Access to Affordable and Equitable Health Coverage: A Review from 2010 to 2024. Accessed: March 31, 2026. . In addition, stable and adequate reimbursement policies are essential to ensuring the financial stability of oncology practices and maintaining continuous access to care, particularly in community-based settings where recent payment changes have introduced new challenges to care delivery.
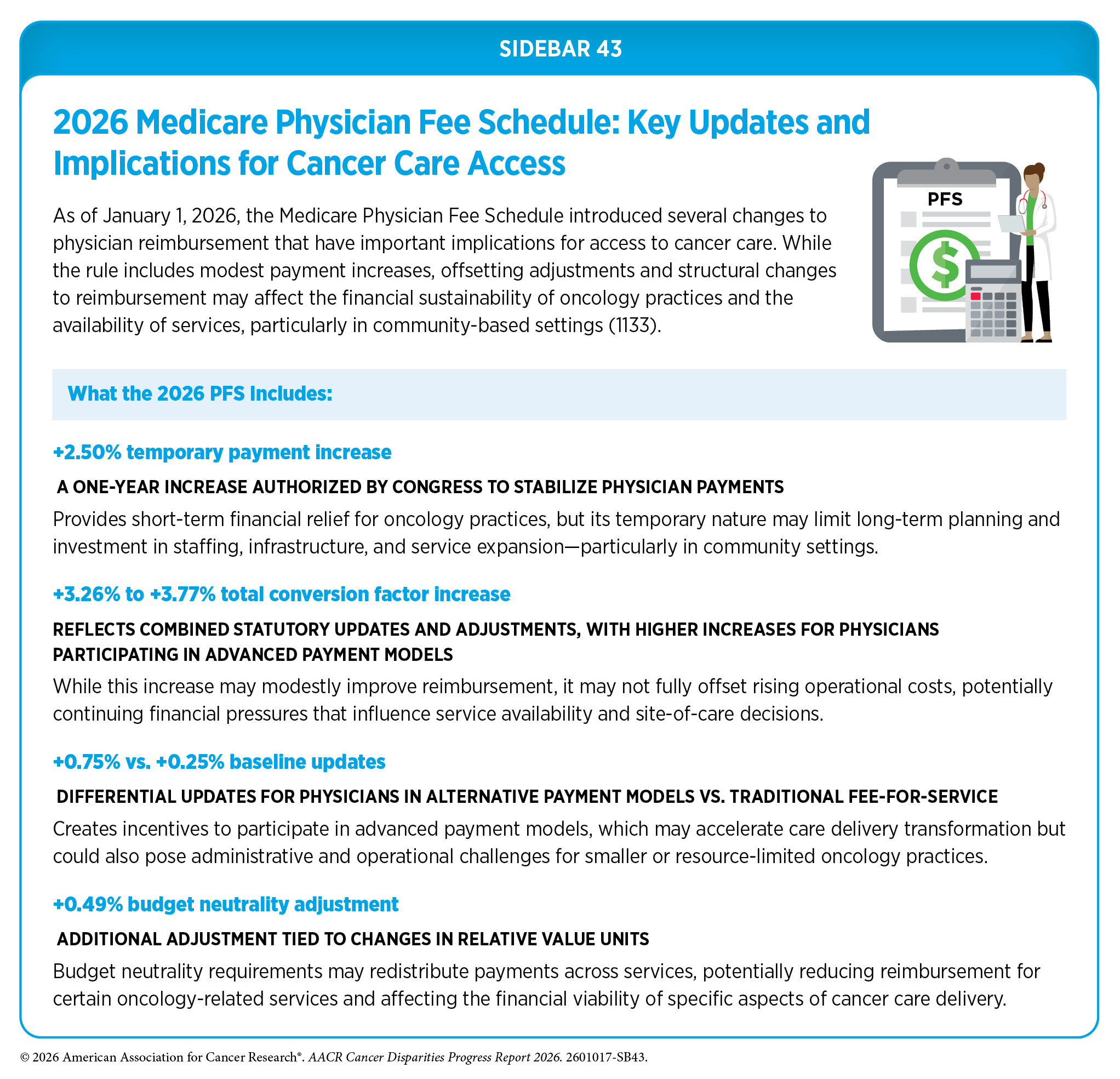
Recent updates to the 2026 Medicare Physician Fee Schedule (PFS) highlight the role of federal payment policy in shaping access to cancer care (1132)American Medical Association. What to expect from the 2026 Medicare Physician Fee Schedule. Accessed: March 31, 2026. . Although the 2026 Medicare PFS includes modest payment increases, offsetting adjustments may result in reduced reimbursement for some providers, which could affect the capacity of practices to deliver timely cancer care, particularly in community settings (see Sidebar 43).
Supporting Patient Navigators and Community Health Workers
Patient navigation and community health worker (CHW) programs are crucial for improving access to quality cancer care (see Sidebar 39). These programs enable individualized support, including care coordination, patient education, and assistance in addressing social and logistical challenges to enhance access to quality care (1134)Lieberman DA, et al. (2025) Clin Gastroenterol Hepatol, 23: 1868. . Research shows that patient navigation and CHW interventions are associated with improved access to care, enhanced patient experience, and better clinical outcomes, particularly among underserved populations (540)Nelson HD, et al. (2025) JAMA Intern Med, 185: 976. (1135)Freeman HP (2006) J Urban Health, 83: 139. (1136)Dwyer AJ, et al. (2022) Cancer, 128 Suppl 13: 2561. .
Recent policy developments have increasingly focused on supporting the sustainability and integration of patient navigation services into routine cancer care. In 2024, CMS established reimbursement pathways for patient navigation through the introduction of Principal Illness Navigation, which continue, under the 2026 Medicare PFS (1137)Centers for Medicare & Medicaid Services. Calendar Year (CY) 2024 Medicare Physician Fee Schedule Final Rule. Accessed: March 31, 2026. (1138)Federal Register. Medicare and Medicaid Programs; CY 2026 Payment Policies Under the Physician Fee Schedule and Other Changes to Part B Payment and Coverage Policies; Medicare Shared Savings Program Requirements; and Medicare Prescription Drug Inflation Rebate Program. Accessed: March 31, 2026. . These services allow for payment for navigation services that address health-related social needs, care coordination, and patient support for individuals with serious conditions, including cancer. The availability of reimbursement represents a significant step toward integrating navigation services into standard oncology care delivery; however, adoption of these billing codes remains variable across health systems.
Efforts to strengthen the oncology navigation workforce have also expanded in recent years. National organizations have developed standardized training and credentialing programs to support competency-based navigation services and align with CMS requirements. For example, the American Cancer Society’s Leadership in Oncology Navigation program provides no-cost training and credentialing to support workforce development and expand access to high-quality navigation services (1139)American Cancer Society. Leadership in Oncology Navigation (LION™). Accessed: March 31, 2026. . Updated training programs in 2025 emphasized core competencies such as care coordination, patient communication, and addressing SDOH, reflecting the evolving role of navigators in oncology care.
Despite these advances, gaps remain in the availability and consistent implementation of navigation and CHW services across care settings. Sustained policy efforts to support reimbursement, workforce development, and integration of navigation into care delivery models will be essential to ensuring that patients can access timely, coordinated, and high-quality cancer care.
Leveraging AI and Digital Health to Address Disparities
AI and digital health tools have the potential to both mitigate and exacerbate cancer disparities, depending on how they are designed, validated, regulated, and governed. Leveraging AI and digital health approaches to reduce disparities requires thoughtful and responsible policies that ensure access to these technologies and fair implementation. Recent studies highlight that AI-enabled tools, such as risk prediction algorithms, imaging diagnostics, and clinical decision support systems, can improve early detection and care coordination, particularly in under-resourced settings, but may also perpetuate disparities if trained on non-representative datasets or deployed without safeguards (1140)Dankwa-Mullan I, et al. (2025) Curr Oncol Rep, 27: 95. (1141)Srivastav AK, et al. (2025) Cancers (Basel), 17. . Frameworks that incorporate “equity-by-design” approaches, including requirements for diverse training data, algorithmic auditing, and transparency in model development, can help ensure that AI systems perform adequately across populations (1142)Roadevin C, et al. (2025) J Med Ethics. . In addition, digital health interventions, such as AI-powered patient navigation, telehealth platforms, and mobile health applications, have shown promise in improving screening uptake and follow-up care among underserved populations, particularly when combined with community-based implementation strategies (1142)Roadevin C, et al. (2025) J Med Ethics. (1143)Kim S, et al. (2025) PLOS Digit Health, 4: e0001028. . Furthermore, mobile health tools that are patient-centric and incorporate tailored and personalized interventions can bridge broader disparities in health care access and engagement (1144)Yang S, et al. (2025) J Med Internet Res, 27: e71349. . Crucially, the cost and equipment required for high-quality AI systems could prevent under-resourced institutions from accessing these technologies, furthering disparities based on socioeconomic factors. While rural and frontier areas could benefit from these systems, they frequently have lower capital to invest in these tools (1145)Hwang Y-M, et al. (2026) NEJM AI, 3: AIp2600103. .
Policy efforts have increasingly focused on establishing guardrails to ensure that AI deployment advances health equity. The 2025 White House “AI Action Plan” and subsequent federal initiatives prioritize responsible AI use in health care, explicitly calling for safeguards against bias, improved data governance, and expanded public–private collaboration to support equitable innovation (1146)The White House. Winning the Race America’s AI Action Plan. Accessed: March 31, 2026. . Complementing this, HHS released a department-wide AI strategy to integrate AI across public health and care delivery while improving patient outcomes and system efficiency (1147)US Department of Human and Health Services. HHS Unveils AI Strategy to Transform Agency Operations. Accessed: 2026, . Regulatory efforts have also advanced health information technology policy, including the HTI-1 Final Rule, which introduces requirements for transparency and evaluation of clinical algorithms to ensure fairness, validity, and safety in real-world use (1148)Office of the National Coordinator for Health Information Technology. HTI-1 Final Rule. Accessed: March 31, 2026. . At the legislative level, proposals such as the Healthcare Enhancement And Learning Through Harnessing Artificial Intelligence (HEALTH AI) Act of 2026 (H.R.5045) seek to fund research and infrastructure for responsible AI deployment in health systems (1149)Congress.gov. H.R.5045 – 119th Congress (2025-2026): HEALTH AI Act. Accessed: March 31, 2026. . Concurrently, policy discussions have increasingly centered on the ethical and equity implications of AI in medicine. National organizations and advocacy groups have called for “equity-first” standards, emphasizing the need to prevent algorithmic bias, ensure clinician oversight, and strengthen privacy protections, particularly for historically marginalized populations (1150)National Association for the Advancement of Colored People. Building a Healthier Future: Designing for AI Health Equity. Accessed: March 31, 2026. . Broader federal actions, including executive efforts to harmonize AI regulation across states, reflect an ongoing shift toward a coordinated national framework. Together, these policy developments emphasize that while AI offers transformative opportunities to reduce cancer disparities through improved access, early detection, and personalized care, achieving this potential will require sustained policy attention to equity, accountability, and inclusive implementation.
Next Section: AACR Call to Action Previous Section: Disparities in the Cancer Training Pathway and Cancer Research and Care Workforce