Executive Summary
This is an extraordinary time in cancer science and medicine. Thanks to decades of research, we are witnessing unprecedented progress against the collection of diseases we call cancer. Yet, these advances have not benefited everyone equally and many segments of the United States (US) population continue to bear a disproportionate burden of cancer. Health care disparities remain among the most profound forms of inequity and injustice, underscoring the urgent need for all stakeholders to eliminate barriers to high-quality health care, the access to which is a fundamental human right.
As the first and largest professional organization in the world dedicated to preventing and curing all cancers for all populations, the American Association for Cancer Research® (AACR) is committed to accelerating research aimed at addressing disparities across the cancer continuum. AACR is also dedicated to increasing public awareness of cancer disparities, highlighting the lifesaving importance of disparities research, and advocating for sustained federal funding for the agencies that drive progress in this area, particularly the National Institutes of Health (NIH), the National Cancer Institute (NCI), and the Centers for Disease Control and Prevention (CDC).
The AACR Cancer Disparities Progress Report 2026 to Congress and the public is a cornerstone of AACR’s educational and advocacy efforts to address cancer disparities. This report highlights recent progress in reducing cancer disparities and emphasizes the continued need for transformative research and strengthened collaborations to ensure that research-driven advances benefit everyone, regardless of race, ethnicity, age, sexual orientation, gender identity, socioeconomic status, or geographic location.
The State of US Cancer Disparities in 2026
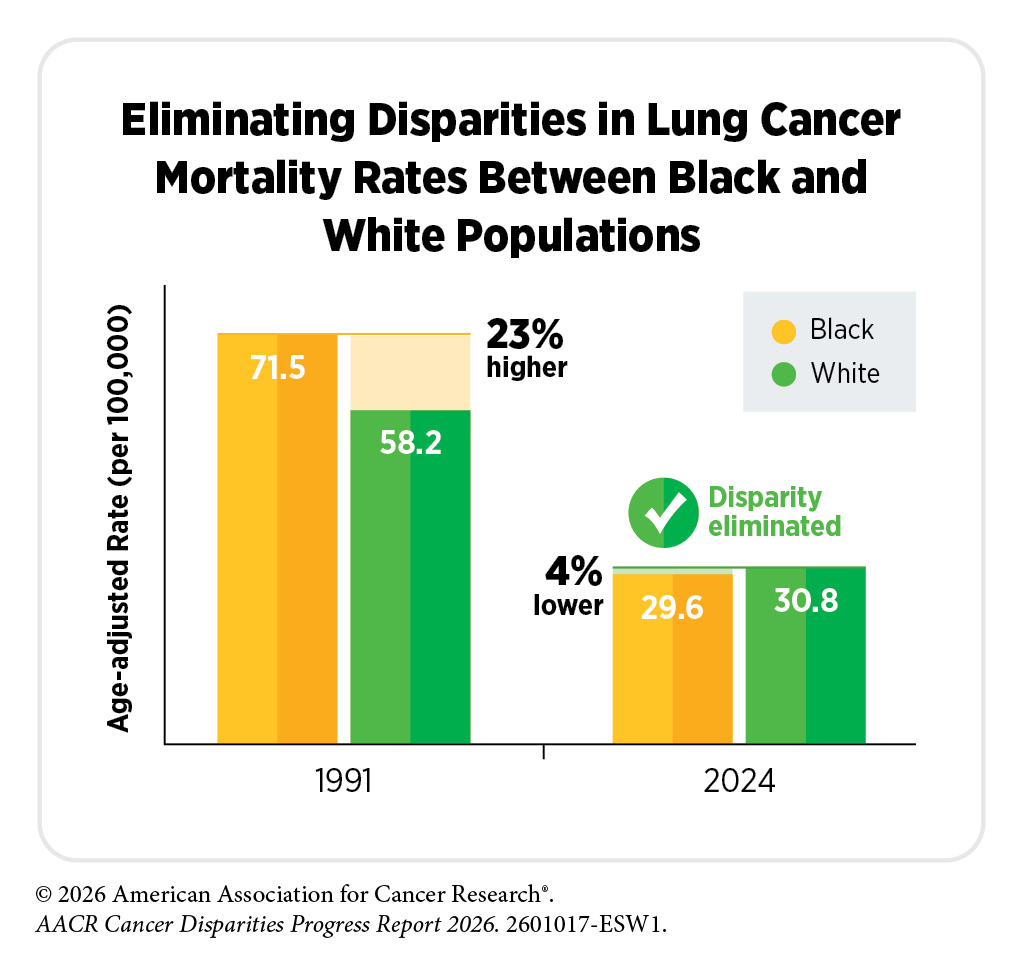
Remarkable advances in cancer prevention, early detection, and treatment have contributed to substantial progress against cancer in the United States over the past several decades. Since 1991, the overall cancer death rate has declined by 35 percent, translating to more than 4.8 million fewer cancer deaths and a growing population of cancer survivors.
Despite these advances, cancer disparities remain a pressing public health challenge. Compared to White populations, Black populations experience higher incidence and mortality rates for several cancers, including multiple myeloma and prostate cancer, while American Indian or Alaska Native (AIAN) populations have higher incidence and mortality rates for cancers of the colorectum, kidney, and cervix. Hispanic and Asian populations bear a disproportionate burden of infection-related cancers, including liver and stomach cancers. In addition, the overall cancer death rate remains higher among Black and AIAN populations, and all racial and ethnic minority populations have lower 5-year relative cancer survival compared to White populations. Other concerning trends include increasing rates of early-onset colorectal cancer among AIAN populations, as well as the rising incidence of lung cancer among Asian women who have never smoked.
Importantly, disparities in the burden of certain cancer types have declined for some populations in recent decades. For example, overall cancer mortality among Black men declined by more than 50 percent between 1991 and 2024—the largest reduction of any racial or ethnic group. Disparities have also narrowed for specific cancers, including cervical cancer mortality between Hispanic and White populations and stomach cancer mortality between Asian or Pacific Islander and White populations. However, persistent cancer disparities underscore the need for continued efforts to ensure that all individuals have equitable access to high-quality care and the opportunity to achieve optimal health outcomes.
It is increasingly evident that racial and ethnic population groups in the United States are highly diverse, and variations in cancer burden by country of origin, nativity, and geographic context highlight the importance of collecting disaggregated data to fully understand the extent of cancer disparities within and among these populations. For example, cancer statistics for Asian American and Native Hawaiian or Pacific Islander (NHPI) populations are often reported in aggregate, which can mask substantial disparities in cancer burden experienced by NHPI populations as well as important differences among Asian subgroups.
In addition to racial and ethnic minority groups, many segments of the US population shoulder a disproportionate burden of cancer. These include rural residents, people living in persistent-poverty areas, and individuals who belong to sexual and gender minority (SGM) populations. Declines in overall cancer death rates have been slower among rural residents compared to those living in urban counties, widening the existing disparities. Individuals living in persistent-poverty areas also experience worse outcomes across the cancer continuum than those in non–persistent-poverty areas, including higher incidence, more advanced stage at diagnosis, and higher mortality across multiple cancer types. Additionally, population-level data on cancer incidence and mortality among SGM populations remain limited, hindering efforts to fully understand and address cancer disparities in this population.
Cancer disparities not only affect patients, families, and communities, but also impose a substantial burden on the US economy. In 2018 alone, racial and ethnic health inequities were estimated to cost the US economy approximately $451 billion due to excess medical costs, lost productivity, and premature deaths, while disparities associated with lower educational attainment accounted for an additional $978 billion. Eliminating cancer disparities requires sustained, coordinated, and adequately resourced efforts across all sectors. Robust and predictable federal investment in medical and public health research to understand and address cancer disparities must be a national priority to reduce the cancer burden and improve outcomes for all populations.
Understanding and Addressing Drivers of Cancer Disparities
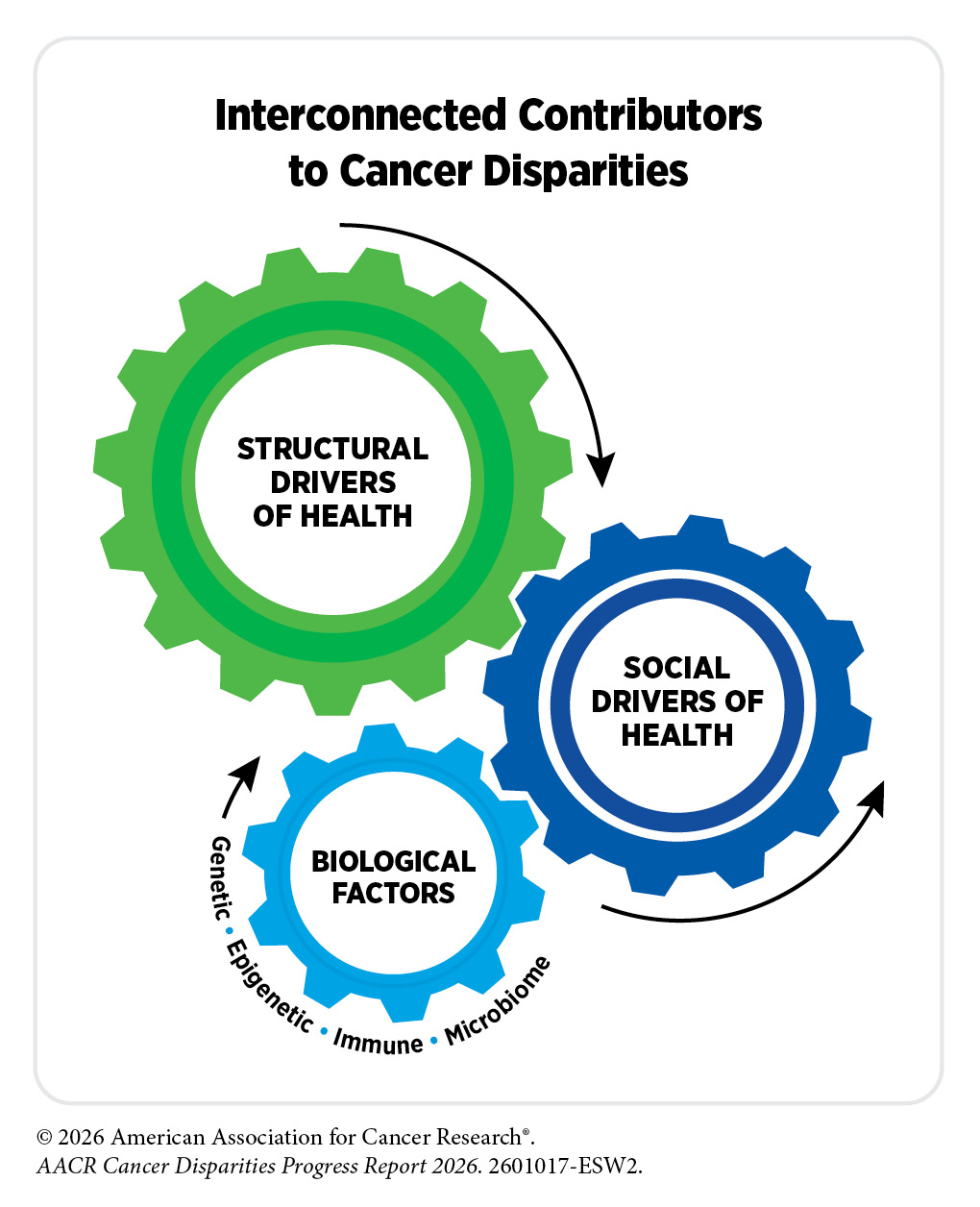
Disparities in health and cancer in the United States are shaped by a complex interplay of structural factors, biological processes, and social drivers of health (SDOH)—such as income, education, housing, and access to care—that influence health across the life course. SDOH do not operate in isolation but interact at individual, community, and societal levels to shape cancer risk, access to prevention and treatment, and outcomes. Racial and ethnic minority groups and other medically underserved populations experience a disproportionate burden of cancer driven by persistent disparities across the cancer care continuum.
Structural inequities, such as racism, segregation, and unequal access to resources, are deeply rooted in US history. Discriminatory policies, such as redlining, have led to residential segregation and uneven distribution of resources. These structural inequities shape neighborhood environments, influencing exposure to environmental hazards, access to health-promoting resources, and opportunities for economic mobility. Evidence shows that individuals living in historically segregated neighborhoods experience higher risks of cancer incidence, later-stage diagnoses, and poorer survival. These disparities are further compounded by socioeconomic disadvantages, which are associated with reduced access to preventive services, delayed diagnoses, and higher cancer mortality.
Access to quality health care remains a critical driver of cancer disparities. Uninsured and underinsured individuals experience disparities across the cancer care continuum. Even when insurance coverage is available, barriers—such as lack of transportation, limited geographic access to care, and high health care costs—can limit care. At the same time, social and economic stressors, including financial strain, housing instability, and food insecurity, can reduce engagement with preventive services and treatment adherence.
Evidence is emerging that the adverse effects of social disadvantages on cancer can be influenced by chronic stress. Persistent exposure to stressors, such as discrimination, poverty, and environmental hazards, can lead to physiological changes, including chronic inflammation and dysregulated immune function, that may increase cancer risk and worsen outcomes. Additionally, stress may increase cancer risk by contributing to unhealthy behaviors such as smoking, alcohol use, physical inactivity, and poor diet.
Importantly, broader structural and environmental contexts often shape conditions that limit individuals’ ability to engage in healthy behaviors, contributing to cancer disparities. Addressing these inequities requires coordinated, multisector approaches, including policy reforms, health system interventions, research initiatives, and community-based programs, that target the underlying structural and social drivers of health.
Understanding Cancer Development in the Context of Cancer Disparities
Cancer is a collection of diseases in which some of the body’s cells acquire changes that enable them to grow uncontrollably, resist cell death, and spread to other parts of the body. Cancer development is a complex and multistep biological process, shaped by influences inside and outside the cell. Social and environmental exposures can modify biological processes, such as chronic inflammation, metabolism, and epigenetic regulation, contributing to differences in cancer risk, tumor biology, and outcomes across populations.
Basic research plays a central role in uncovering mechanisms that drive cancer development and provides the foundation for prevention, early detection, diagnosis, and treatment strategies. Accurately describing populations in research studies, including how sociodemographic and biological characteristics are measured and reported, is critical to ensuring that research findings are meaningful and representative across populations. Race and ethnicity categories capture important social, environmental, and structural drivers of health, but they are not biologically meaningful representations of the human genetic variation. In contrast, genetic ancestry, which is typically inferred using measures of genetic similarity, provides information about inherited patterns of genetic variation. Considering both biological and social factors together can improve the interpretation of research findings, strengthen scientific rigor, and help ensure that discoveries benefit all populations.
A major challenge in cancer research has been the lack of diversity in research models, datasets, and biorepositories, which have largely been derived from individuals of European ancestry. The limited representation of other populations in these resources limits the applicability of research findings and highlights the need for more inclusive resources to conduct cancer science.
Inside the cell, genetic alterations, RNA variations, protein modifications, and epigenetic changes can drive cancer development. Genetic alterations can be inherited from parents or acquired during an individual’s lifetime due to errors in cell division or in response to social and environmental exposures.
Studies have identified differences in the frequency and types of these alterations among individuals across populations. Differences in gene regulation and RNA processing have also been observed across population groups and may contribute to variations in tumor characteristics and cancer outcomes. Studies of proteins and protein modifications have identified both shared and population-specific biological markers associated with cancer risk. Epigenetic changes—shaped by aging, environmental exposures, behavioral and lifestyle factors, and psychosocial stressors—can provide insight into how disadvantaged neighborhoods or chronic stress may influence cancer risk and development.
Interactions between cancer cells and their environment, known as the tumor microenvironment (TME), as well as the blood, lymphatic, and immune systems, and microbiome, play essential roles in cancer development. The TME is composed of cancer cells and supportive non-cancer cells, blood vessels, signaling molecules, and structural components and reflects the combined effects of inherited genetic variation, chronic inflammation, epigenetic changes, and immune response. Research has identified components of TME that differ across patient populations that may contribute to differences in tumor behavior and treatment response. Differences in immune responses and inflammation observed across populations may affect both cancer development and response to therapies such as immunotherapy. The microbiome—shaped by environmental, socioeconomic, cultural, dietary, lifestyle, and health exposures—can further modulate inflammation, metabolism, immune responses, and cancer development.
Advances in precision medicine are transforming cancer care by tailoring prevention, diagnosis, and treatment approaches to the unique characteristics of patients and their cancer. However, disparities in access to molecular testing, emerging technologies, and precision therapies have limited the benefits of these innovations. Ensuring that precision medicine benefits all patients will require expanding the diversity of research datasets, improving access to care and technology, and integrating biological insights with social and environmental context.
Disparities in the Burden of Modifiable Behavioral Cancer Risk Factors
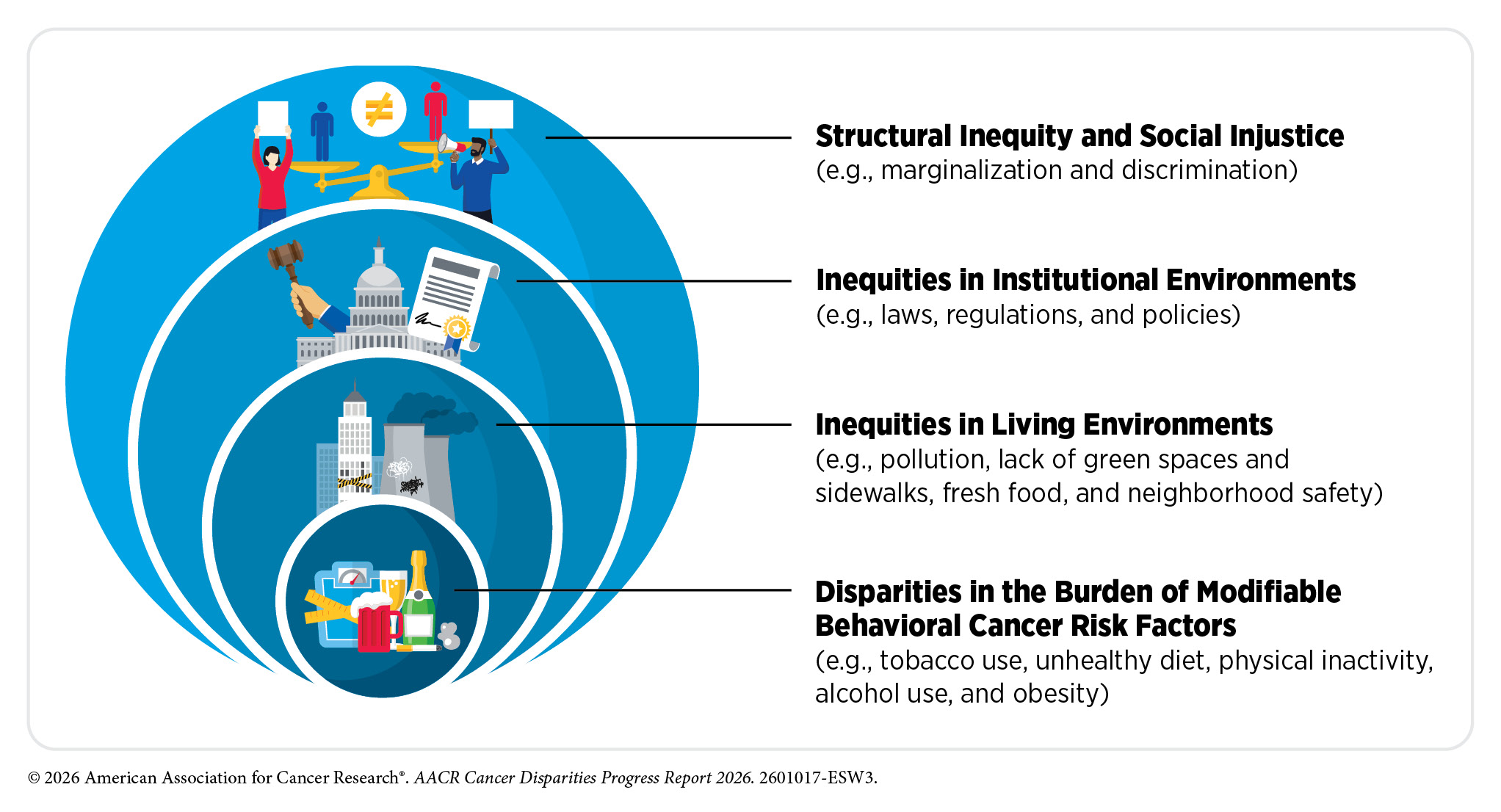
Research across basic, translational, and population sciences has identified a wide range of modifiable factors that increase cancer risk. Behavioral and lifestyle factors—including tobacco use, unhealthy diet, physical inactivity, alcohol consumption, ultraviolet (UV) exposure, obesity, and infectious agents—are estimated to contribute to approximately 40 percent of all cancers. Although individuals can reduce their cancer risk by modifying these behaviors, distribution of these risk factors varies widely across the US population. These differences reflect broader structural and social conditions that shape opportunities for healthy behaviors, underscoring that cancer risk is not only influenced by individual choices but also shaped by the environments in which people live.
Historical and structural inequities have played a major role in shaping these environments. Discriminatory housing policies, such as redlining, have resulted in neighborhoods with higher poverty, greater environmental hazards, and limited access to health-promoting resources. These conditions are associated with increased exposure to cancer risk factors—such as higher densities of tobacco and alcohol retailers and reduced access to high-quality food stores—making healthier behaviors more difficult to adopt. Addressing these systemic inequities is therefore essential to reducing disparities in cancer risk and improving population health.
Commercial tobacco use is the leading modifiable cause of cancer, contributing to at least 18 cancer types. Although cigarette smoking in adults has declined significantly over the past several decades, disparities persist across socioeconomic, racial, and geographic groups. Smoking rates are also substantially higher among individuals with lower educational attainment, those belonging to SGM populations, and residents of certain Southern and Midwestern states. Often referred to as “Tobacco Nation,” these states are characterized by weaker tobacco control policies, lower taxes on tobacco products, and limited access to cessation programs, which contributes to higher cancer burdens. Targeted marketing strategies, particularly for menthol cigarettes among Black populations, have further exacerbated disparities. Further, the use of electronic cigarettes and other tobacco products, especially among youth and young adults, presents additional challenges and raises major concerns about long-term health effects.
Obesity, unhealthy diet, and physical inactivity are major contributors to cancer risk, accounting for a substantial proportion of new cancer cases and deaths. Obesity is linked to at least 13 cancer types. The rise of obesity in the United States in recent decades has disproportionately affected racial and ethnic minority groups and other medically underserved populations. Diets high in ultra-processed foods and low in fruits and vegetables can elevate cancer risk, with food insecurity and limited access to nutritious foods contributing to disparities. Physical inactivity also increases cancer risk through mechanisms such as weight gain and chronic inflammation. It is driven in part by environmental and socioeconomic conditions, including unsafe neighborhoods, inadequate availability of recreational facilities, and constrained time and resources, all of which contribute to disparities in cancer risk.
Alcohol consumption is another important risk factor, contributing to at least 7 different types of cancer. However, public awareness of the role of alcohol in cancer remains low. Alcohol consumption varies across demographic groups, influenced by social norms, stress, and structural factors, with some populations experiencing higher rates of heavy or binge drinking.
UV exposure contributes to cancer risk, particularly skin cancers, with disparities observed in both UV exposure and cancer outcomes. While the incidence of melanoma, the deadliest form of skin cancer, is highest among White individuals, racial and ethnic minority populations often experience later-stage diagnoses and poorer survival due to differences in awareness, prevention, and access to care.
Infectious agents, including human papillomavirus (HPV), hepatitis B and hepatitis C viruses, and Helicobacter pylori, are responsible for a significant proportion of cancers. Preventive measures, such as vaccination, can dramatically reduce the risk of certain infection-related cancers; however, disparities in access and uptake persist. For example, HPV vaccination rates remain lower in rural areas and among certain racial and ethnic groups. Similarly, hepatitis infections disproportionately affect racial and ethnic minority populations, contributing to higher rates of liver cancer.
Advances in research are deepening our understanding of how environmental and occupational exposures contribute to cancer risk. Exposure to pollutants, carcinogenic chemicals, endocrine-disrupting substances, and ionizing radiation is often higher in communities affected by socioeconomic disadvantages or located near industrial or hazardous sites. Climate change can further amplify these risks by increasing the likelihood of environmental hazards, such as wildfire smoke. Similarly, certain occupations—such as firefighting, construction, and industrial work—are associated with higher exposure to cancer-causing agents, with disparities reflecting broader patterns of economic inequality.
Cancer risk is shaped by a complex interaction of behavioral, environmental, biological, and social factors. Reducing the burden of cancer requires addressing the structural and systemic drivers to help alleviate unequal exposure of certain population groups to risk factors and promote healthy behaviors at the individual level.
Disparities in Cancer Screening for Early Detection
Screening for early detection means finding precancers or cancer at the earliest stage possible when it is more likely to be curable. Cancer screening is a continuum that involves eligible individuals receiving screening tests at routine intervals based on evidence-based guidelines. If results from the initial test indicate abnormality, follow-up diagnostic testing is essential to rule out or confirm these findings.
In the United States, screening guidelines are developed by expert panels, most notably the US Preventive Services Task Force (USPSTF), which evaluates evidence on the benefits and harms of screening and issues recommendations. USPSTF currently recommends routine screening for breast, cervical, colorectal, and prostate cancers for individuals at average risk, and for lung cancer for those at higher risk (e.g., people who smoke). A recent analysis estimated that screening and prevention strategies for these five cancer types together accounted for nearly 4.75 million cancer deaths averted in the United States between 1975 and 2020, indicating that routine cancer screening is one of the most effective tools to reduce cancer mortality.
Unfortunately, cancer screening uptake remains uneven across population groups for many cancer types. The suboptimal uptake of routine screening is attributable to differences in insurance status, income, education, immigration status, and geography. Persistent gaps in who gets screened, and who receives timely follow-up after an abnormal result, continue to drive disparate cancer outcomes in medically underserved populations.
Insurance status is one of the key drivers of screening disparities, with uninsured individuals less than half as likely to be screened as those with private insurance across most cancer types. Suboptimal screening eligibility criteria can also perpetuate disparities. For example, current smoking-based thresholds for lung cancer screening, the uptake of which is only 19 percent, systematically exclude a disproportionate share of Black individuals who develop lung cancer at lower levels of tobacco exposure than White individuals. Furthermore, screening disparities extend to differences in follow-up care.
Gaps in availability and insurance coverage of new screening technologies, such as multi-cancer early detection tests, which can screen for multiple cancers simultaneously, raise the prospect that uneven access to these tools may further widen disparities based on socioeconomic status. Disparities in access to hereditary cancer surveillance—which is risk-based monitoring for individuals with inherited cancer syndromes—follow similar patterns, with non-White populations underrepresented in surveillance programs despite the willingness to participate once enrolled, emphasizing the role of system-level barriers in risk identification and referrals.
Evidence-based interventions to increase screening uptake and follow-up diagnostic testing among medically underserved populations demonstrate that screening disparities can be avoided. Patient navigation, mailed outreach, culturally tailored community engagement strategies, and improved health systems have all shown meaningful impact. An analysis of 42 randomized clinical trials found that patient navigation increased breast cancer screening by 50 percent and cervical cancer screening by 62 percent, with the strongest effects in medically underserved populations. Additionally, policy changes, such as Medicaid expansion, have produced measurable increases in screening uptake among previously uninsured populations. Integrating genetic risk assessment into primary care has the potential to eliminate referral-based disparities in genetic counseling for inherited cancer syndromes.
Realizing the full potential of cancer screening to reduce mortality across all populations requires partnerships and collaborations across health systems, researchers, and policymakers for targeted and sustained efforts to eliminate the barriers that limit access.
Disparities in Clinical Research and Cancer Treatment
The steady decline in the overall US cancer mortality and improvements in survival rates are attributable, in part, to rapid advances in cancer treatment driven by breakthroughs in medical research. Clinical trials are a vital part of medical research because they establish whether or not new cancer treatments are safe and effective for the patients who need them. Despite significant advances in clinical research design and conduct, low participation and lack of diversity in adult cancer clinical trials restrict the ability to ensure that research findings reflect and benefit all patient populations.
Patients from racial and ethnic minority groups and other medically underserved populations experience multilevel barriers to participating in clinical trials. Most of these barriers operate at the systemic level, including in the way that trials are designed and implemented. Additionally, adult and pediatric participants from medically underserved populations may experience worse survival even in a controlled clinical trial setting, indicating that structural and social drivers of health, as well as other biologic predictors of toxicities or recurrence, may continue to influence outcomes. Addressing unmet socioeconomic needs of patients through community outreach and engagement and navigation can help overcome many of the challenges in clinical trials. It is vital that all stakeholders in the medical research community work together to identify and implement interventions that ensure equitable clinical trial participation and outcomes.
Despite unprecedented progress in cancer treatment over the past two decades, including major breakthroughs in precision medicine, patients from racial and ethnic minority groups and other medically underserved populations remain less likely to receive the recommended standard of care for their cancer, leading to worse outcomes. Notably, research shows that disparities in survival rates for many cancers can be drastically reduced when all patients have access to high-quality, guideline-adherent treatments, including diagnostic testing and precision medicine. Evidence from integrated health care systems, such as the Veterans Health Administration, demonstrates that when access is comparable, outcomes across racial, ethnic, and socioeconomic groups are often similar and, in some cases, better for underserved populations.
Multilevel interventions that include patient navigation and community outreach and engagement are critical to improving access to cancer care, treatment initiation, adherence and completion, and genomic testing. Additionally, policies such as Medicaid expansion may enhance insurance coverage, leading to earlier diagnosis and improved patient survival. However, persistent treatment disparities highlight the continued influence of structural and clinical factors, as well as ongoing geographic barriers, on the receipt of evidence-based cancer care. These findings underscore the need for comprehensive strategies that combine equitable access to care, community-informed interventions, and supportive policies to improve outcomes for all populations.
Disparities in Cancer Survivorship
According to NCI, a person is considered a cancer survivor from the time of cancer diagnosis through the balance of the person’s life. Advances in cancer prevention, early detection, and treatment have contributed to substantial improvements in survival, resulting in a growing population of cancer survivors in the United States. As of January 1, 2025, more than 18.6 million adults and children with a history of cancer were living in the United States, and this number is projected to exceed 22 million by 2035. However, survivors from racial and ethnic minority groups, rural communities, SGM populations, and other medically underserved groups often experience greater barriers to high-quality survivorship care and supportive services. As the US population ages and becomes more diverse, the number of survivors from medically underserved populations will continue to grow. Understanding the challenges faced by these populations can help inform survivorship care strategies and supportive interventions tailored to their unique needs, ultimately improving long-term health outcomes and quality of life.
Cancer survivors experience a wide range of physical, psychosocial, and financial challenges related to their cancer and/or cancer treatment. These challenges can emerge during treatment or long after its completion, requiring ongoing care and support. Evidence shows that medically underserved populations experience a higher burden of adverse physical and psychosocial effects, greater financial hardship, and increased barriers to mental health services, supportive care, and long-term follow-up. These disparities are driven, in part, by broader structural and social drivers of health, including poverty, housing instability, medical mistrust, discrimination, and limited access to health care services.
A diagnosis of cancer also impacts friends, family members, and other caregivers, who often serve as the primary support network of cancer survivors. Caregivers from medically underserved populations frequently face additional financial, emotional, and logistical burdens that can compound the challenges of survivorship. As a result, survivorship research, support, and care must extend beyond the cancer patient and survivor to include individuals who comprise the broader support network.
A growing body of evidence suggests that disparities in survivorship outcomes can be reduced through coordinated, patient-centered approaches that integrate supportive care, mental health services, lifestyle interventions, survivorship care planning, and caregiver support into routine cancer care. Strategies such as patient navigation, telehealth-based interventions, and community-partnered programs have shown promise in improving access to survivorship services and reducing barriers to care among medically underserved populations. Culturally tailored interventions and approaches that address structural and social drivers of health may help improve long-term health outcomes and quality of life among medically underserved populations.
Persistent disparities in survivorship experiences are driven by fragmented and variable survivorship care delivery across health systems. To address these challenges, NCI and the US Department of Veterans Affairs have developed the first National Standards for Cancer Survivorship Care to guide health systems in delivering high-quality survivorship services. These standards provide a comprehensive framework for organizing survivorship services and evaluating their impact, offering health systems a roadmap to strengthen care delivery, expand access to supportive services, and ensure that all survivors—regardless of race, ethnicity, sexual orientation, gender identity, socioeconomic status, or geographic location—receive coordinated, patient-centered care across the cancer continuum.
Disparities in the Cancer Training Pathway and Cancer Research and Care Workforce
A robust cancer research and care workforce depends on the representation of individuals across racial, ethnic, geographic, and socioeconomic backgrounds and lived experiences. Building a workforce that reflects diverse populations strengthens cancer research and care by broadening the talent pool, mitigating systemic biases, enhancing cultural competence, and supporting patient-centered care. Evidence shows that workforce diversity is associated with greater patient trust, improved communication, higher treatment adherence, and better health outcomes.
Disparities in access to education and training opportunities, research funding, and barriers at critical career transition points continue to limit entry, retention, and advancement of individuals from historically underrepresented groups across the cancer workforce. A strong foundation in science, technology, engineering, and mathematics (STEM) is essential for entry into careers in cancer research and care. Unfortunately, students from underrepresented racial and ethnic groups, rural areas, and lower socioeconomic households are more likely to attend under-resourced kindergarten through 12th grade schools with limited access to qualified teachers, advanced coursework, and mentorship opportunities.
At the graduate and postdoctoral levels, such disparities in representation are evident. While biological and biomedical sciences programs enroll large numbers of trainees, certain racial and ethnic minority groups remain underrepresented relative to their proportion of the US population. International trainees also play a critical role in sustaining research productivity, yet recent policy changes and increased barriers to immigration threaten this pipeline. At the same time, fewer PhD recipients are pursuing academic research careers, with many shifting to roles in the private sector. This trend raises concerns about the long-term sustainability of academic cancer research.
The transition from training to independent research is a particularly vulnerable point in the basic and translational research career pathway. Early-stage investigators face intense competition for limited federal funding as they establish laboratories and research programs. Unequal access to funding disproportionately affects women and researchers from underrepresented racial and ethnic groups. These disparities limit opportunities for career advancement and contribute to higher attrition rates. Recent funding instability, including grant terminations and shifting policy environments, has further exacerbated these challenges, unequally affecting early-career researchers.
Despite many efforts over the past decade, underrepresentation of certain racial and ethnic minority populations, SGM groups, and individuals from low socioeconomic status continues in the oncology training pathway and workforce. Black, Hispanic, and AIAN individuals are underrepresented among medical school applicants, matriculants (i.e., those who became enrolled in medical school), and trainees. Recent policy changes affecting admissions and diversity initiatives threaten to further narrow pathways to training future oncologists. Fewer students entering medical school from diverse backgrounds ultimately translate into fewer residents, fellows, and attending oncologists, with disproportionate effects on communities already facing barriers to cancer care.
Disparities are also evident within leadership positions in the cancer research enterprise. Women and individuals from underrepresented groups remain less likely to attain senior academic and leadership positions, limiting their influence on research priorities, mentorship, and institutional decision-making.
The unequal geographic distribution of the oncology workforce further compounds disparities in access to care, particularly for individuals living in rural areas.
Beyond physician-scientists and clinicians, other health care professionals, including physician assistants, nurse practitioners, and community health workers, play a critical role in delivering comprehensive cancer care. Yet the workforce within many of these professions also does not reflect the populations they serve. Ensuring a diverse and well-supported cancer care workforce is essential for improving patient experiences, strengthening trust, and addressing barriers to care.
Disparities across the cancer training pathway and workforce highlight the need for sustained funding, education, mentorship, and policy solutions to build a diverse, resilient, and innovative workforce capable of advancing high-quality care for all patients.
Overcoming Cancer Disparities Through Science-based Public Policy
Implementation of science-based public policy is essential to ensure that advances in cancer prevention, detection, treatment, and survivorship benefit all communities equitably. Coordinated policy action and federal investment across the cancer research and care continuum can help translate scientific innovation into measurable reductions in cancer disparities. Furthermore, partnerships and community-based programs can support disparities research and interventions that are tailored to the needs of the communities they are meant to serve.
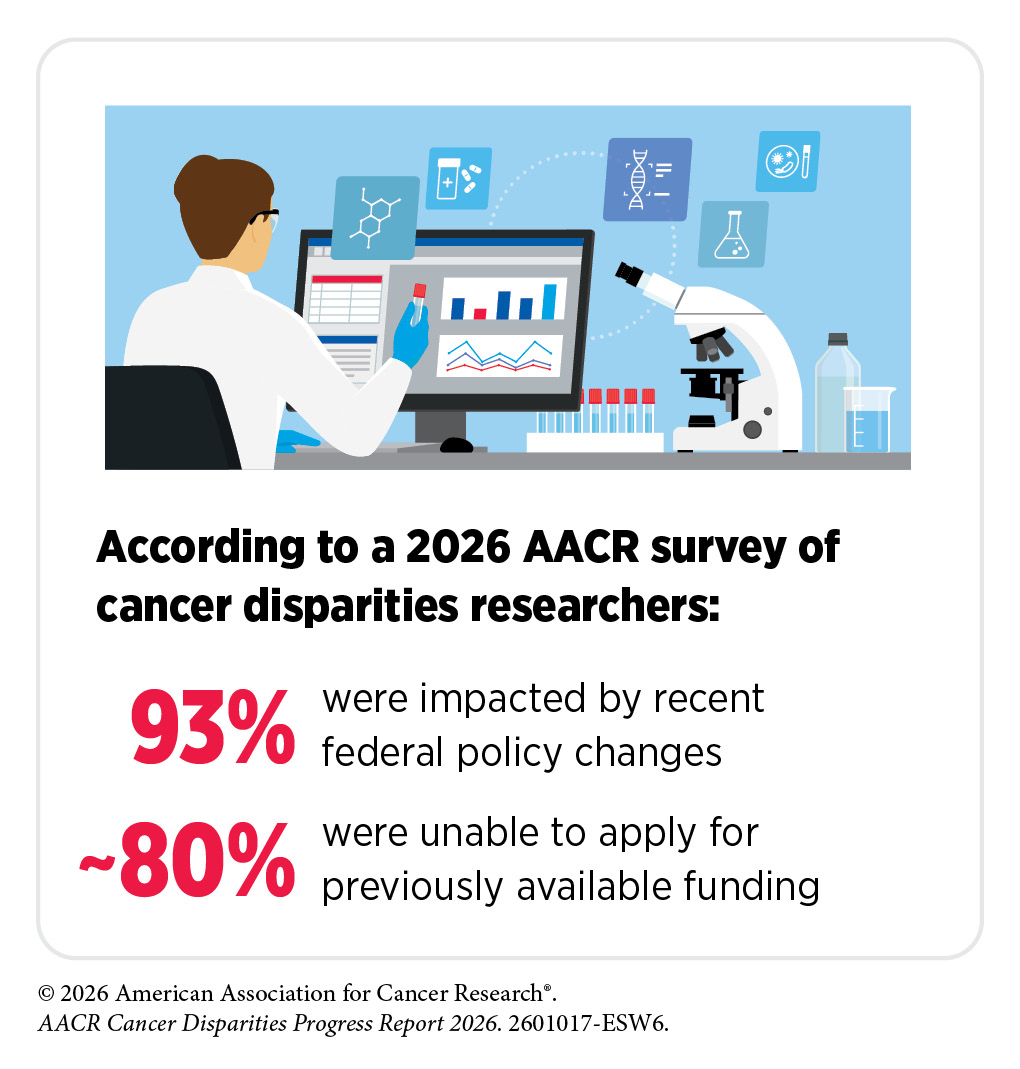
Sustained and robust funding for key federal agencies is foundational to advancing cancer disparities research and implementing programs that expand access to care. Federal programs and initiatives have demonstrated that targeted investment can narrow gaps in screening, clinical trial participation, and cancer outcomes. Interagency collaborations have further strengthened these efforts by aligning research, prevention, and care delivery strategies to address disparities. However, recent funding disruptions and termination of disparities-focused initiatives threaten the infrastructure that supports this progress and weaken the federal government’s capacity to address cancer disparities. In addition, recent proposals to remove disparity-focused metrics, restructure agencies, and eliminate health equity–related programs risk undermining the ability to measure and address disparities in cancer outcomes.
A diverse and inclusive medical research workforce is central to achieving health equity. Long-standing NIH and NCI programs that provide training, mentorship, and career development for investigators from underrepresented populations have strengthened the cancer research enterprise and improved its ability to address disparities. Recent eliminations of workforce diversity programs and disruptions to early-career funding compromise this progress. Codifying and restoring these programs, protecting early-career and early-stage investigators, and supporting bridge funding mechanisms are critical policy steps to maintain a workforce that reflects and effectively serves the nation’s diverse populations.
Evidence-based public policies are powerful tools for reducing cancer disparities. Tobacco control programs, environmental health protections, and efforts to limit exposure to carcinogens have lowered cancer risk in disproportionately affected communities and continue to demonstrate how effective policy implementation can drive progress. Expanding equitable access to cancer screening and follow-up care is one of the most impactful strategies to reduce cancer mortality. Patient-centric approaches, such as at-home testing, mobile screening programs, risk-adapted eligibility criteria, and patient navigation, are improving early detection across diverse populations and reducing barriers to preventive care.
Ensuring equitable representation in clinical trials and access to high-quality cancer care is essential to translating scientific advances into better outcomes for all populations. Regulatory guidance promoting representative enrollment, more accessible trial designs, sustainable reimbursement, and patient navigation services is helping close gaps in care delivery, particularly in rural and underserved areas. Emerging tools such as artificial intelligence and digital health technologies offer additional opportunities to reduce disparities when guided by policies that emphasize equity-by-design, transparency, incorporation of diverse data, and broad access to innovation.
Together, evidence-based federal policies and legislative actions, sustained investment, inclusive workforce development, equitable prevention strategies, modernized screening policies, access to guideline-based treatments, representative clinical research, and responsible technology governance can ensure that cancer disparities research translates into equitable outcomes for all populations.
AACR Call to Action

The evidence highlighted throughout this report demonstrates that cancer disparities are neither inevitable nor insurmountable. Federal investments through NIH, NCI, CDC, and other agencies, alongside national screening and research programs, have measurably reduced cancer mortality and expanded access to care for populations disproportionately affected by cancer. However, recent funding cuts and disruptions to disparities-focused programs seriously threaten the research infrastructure and community-based initiatives that made the progress to date possible, placing the greatest burden on individuals from racial and ethnic minority groups, rural and frontier communities, persistent-poverty areas, and other medically underserved populations at increased cancer risk.
Significantly reducing cancer disparities in the United States, with a longer-term goal of completely eliminating them, is an achievable goal, provided that our nation’s policymakers prioritize the research and policy proposals that are necessary to ensuring that every patient has a fair opportunity to benefit from advances in cancer science and medicine. Future progress will depend on renewed federal and legislative actions commensurate with the scale and urgency of the challenge.
By taking the following actions outlined below, AACR is confident that we will not only significantly reduce cancer disparities, but we will eliminate them altogether:
- Sustain and strengthen federal investments in cancer disparities research.
- Support data collection initiatives to reduce cancer disparities.
- Ensure every cancer therapy is evaluated in the populations in which it is meant to be utilized.
- Ensure equitable cancer prevention, screening, genetic testing, and follow-up care.
- Implement policies to ensure equitable patient access to lifesaving therapies.
- Build a cancer research and patient care workforce that reflects the nation it serves.
By advancing these actions, and with sustained commitment and investment, Congress and federal agencies can accelerate scientific discovery, meaningfully reduce the cancer burden for all communities and populations, and save lives while strengthening the nation’s health, economy, and scientific enterprise.
Next Section: A Snapshot of US Cancer Disparities and Progress Toward Equity Previous Section: Message from AACR