Disparities in the Cancer Training Pathway and Cancer Research and Care Workforce
In this section, you will learn:
- A cancer research and care workforce that reflects the populations it serves strengthens trust, communication, treatment adherence, research participation, and patient-centered care, while also reducing systemic bias and improving outcomes.
- Inequitable access to kindergarten through 12th grade resources, underrepresentation in science, technology, engineering, and mathematics fields and medical education, research funding disparities, and barriers at critical career transition points collectively limit entry, retention, and advancement of underrepresented individuals and drive persistent gaps in cancer training pathway and workforce.
- Long-standing federal, academic, and professional programs have helped increase workforce representation by supporting students and trainees from historically underrepresented backgrounds.
- The current environment of funding instability and policy shifts disproportionately threatens early-career and underrepresented researchers. A 2026 AACR survey of cancer disparities researchers found widespread adverse impact of the current environment on the field.
- Unequal access to federal funding, recent grant terminations, visa and immigration barriers, and declining interest in academic careers jeopardize a sustainable, innovative, and representative cancer science and medicine training pathway and workforce.
Contents
A robust cancer research and patient care workforce depends on representation across racial, ethnic, geographic, and socioeconomic backgrounds and lived experiences. Building a workforce that reflects the diversity of the populations it serves, and the geographic diversity across the United States (US), strengthens cancer research and care by broadening the talent pool, mitigating systemic biases, enhancing cultural competence, and supporting patient-centered care. Growing evidence shows that workforce diversity is associated with greater patient trust, improved communication, higher treatment adherence, and better health outcomes, in part by enabling more timely and appropriate care and fostering meaningful engagement with patients and communities (974)Gupta H, et al. (2025) JAMA Netw Open, 8: e2537667. (975)Alsan M, et al. (2025) J Health Econ, 100: 102968. (976)Fabian AJ, et al. (2026) J Racial Ethn Health Disparities, 13: 1263. (977)Frakes M, et al. (2025) Rev Econ Stud. .
Racial and ethnic concordance between patients and physicians has been linked to improved communication, greater patient trust, higher satisfaction, better treatment adherence, and improved uptake of recommended preventive and therapeutic care—mechanisms that are particularly relevant for mitigating disparities in cancer care. For example, patients with chronic myeloid leukemia have shown higher long-term treatment adherence when their providers shared similar racial and gender characteristics (681)Montano-Campos JF, et al. (2025) JAMA Netw Open, 8: e258039. . Additionally, an analysis of data from the 2010–2016 Medical Expenditure Panel Survey found emergency department use was lower among Hispanic patients with ethnically concordant clinicians. Furthermore, among Black, Asian, and Hispanic patients, those with a racially or ethnically concordant clinician had lower total health care expenditures (14 percent, 34 percent, and 20 percent lower, respectively) (978)Jetty A, et al. (2022) J Racial Ethn Health Disparities, 9: 68. .
A representative cancer research and care workforce drives greater innovation and ensures that the perspectives, priorities, and lived experiences of all communities are reflected across the research and care continuum. It also provides the role models and mentors needed to inspire and sustain the next generation of professionals from historically underrepresented backgrounds. Achieving and maintaining this representation requires coordinated investment across educational pipelines, training environments, funding structures, and leadership pathways.
Building and Sustaining the STEM Pathway to Medicine
Science, technology, engineering, and mathematics (STEM), is an umbrella term for several fields that support entry into multiple career pathways, including health care, medical research, and public health. The United States STEM workforce, which includes any individual who uses specialized training in STEM in their job, comprised 36.8 million people and constituted 24 percent of the total US workforce in 2021 according to the National Science Foundation (NSF) (979)National Science Board. Talent: U.S. and Global STEM Education and Labor Force. Accessed: March 31, 2026. .
Representation of women, certain racial and ethnic minority populations, and sexual and gender minority (SGM) groups in STEM is not commensurate with the representation of these groups within the broader US workforce. According to NSF data from 2021, the most recent year for which data are available, Black, Hispanic, and American Indian or Alaska Native (AIAN) individuals collectively accounted for 23 percent of the STEM workforce, compared to 30 percent of the overall US workforce (979)National Science Board. Talent: U.S. and Global STEM Education and Labor Force. Accessed: March 31, 2026. . Recent trends show that the proportion of underrepresented groups in the STEM workforce increased from 18 percent in 2011 to 24 percent in 2021 (980)National Science Foundation. Diversity and STEM. Women, Minorities, and Persons with Disabilities. 2023. Accessed: March 31, 2026. .
Strengthening the STEM workforce requires a robust, inclusive training pathway that begins in kindergarten through 12th grade (K–12) education and extends through postsecondary, graduate, and medical school, and postdoctoral training. Sustained investment in programs that broaden participation and support individuals from historically underrepresented groups is essential for building and maintaining a diverse, innovative, and resilient STEM workforce.
K–12 Education
A robust K–12 educational system is essential for laying the groundwork that will ensure the long-term success of individuals in the STEM workforce. Underrepresented racial and ethnic minority populations and students from rural areas and lower socioeconomic households are often served by under-resourced K–12 schools, which tend to experience shortages of qualified, well-compensated teachers, support services, classroom supplies, educational field trips, and advanced placement courses (981)Education Law Center. Making the Grade. How Fair is School Funding in Your State? Accessed: March 31, 2026. . Without a strong support and mentorship infrastructure, students in these communities lack exposure to available opportunities in STEM (982)Ruth Kaggwa AB, Emma Wester, Sandra Arango-Caro, Terry Woodford-Thomas, Kristine Callis-Duehl (2023) Journal of STEM Outreach, 6: 15. . For example, a report by the Government Accountability Office found that one district in rural Alabama had no certified math teachers to serve their 300 students in grades 7–12 during the 2023–2024 school year (983)US Government Accountability Office. Selected Federal Initiatives, Challenges, and Approaches to Supporting Rural Populations Accessed: March 31, 2026. .

Increased educational spending can improve student performance and achievement. During the COVID-19 pandemic, the federal government provided $190 billion through the Elementary and Secondary School Emergency Relief Fund, the largest amount of federal funding in K–12 education in US history and more than four times the amount provided in a typical year. This influx of funding led to a measurable increase in student performance, with the most significant impact seen in low-income areas. The Education Recovery Scorecard, which tracks learning loss due to the COVID-19 pandemic and recovery from its impact, found that for every $1,000 of federal relief spent per student, there were measurable increases in math and reading testing scores, particularly in districts where more than 70 percent of students came from low-income households (984)Standford University. Federal Pandemic Relief and Academic Recovery. Accessed: March 31, 2026. .
Within the National Cancer Institute (NCI), the R25 Youth Enjoy Science (YES) Research Education Program funds nonprofit and government research programs for high school and undergraduate students, aiming to increase cancer knowledge and awareness among students underrepresented in STEM while preparing them for careers in biomedical research. Programs funded by the YES Research Education Program have primarily focused on promoting cancer research training to underrepresented racial and ethnic minority youth populations.
Programs that aim to empower K–12 teachers with opportunities to learn more about cancer science and develop curricula to teach students are essential to bridge the educational gap in underfunded and under-resourced schools. As part of the YES Research Education Program, Teach to Beat Cancer at an NCI-designated comprehensive cancer center provides grades 6–12 teachers with opportunities to participate in cancer research to aid in building curricula around cancer (985)Case Comprehensive Cancer Center. Teach to Beat Cancer. Accessed: March 31, 2026. . The National Institutes of Health (NIH) Science Education Partnership Award supports the development and implementation of educational programs to enhance STEM education (986)National Institute of General Medical Sciences. Science Education Partnership Award (SEPA). Accessed: March 31, 2026. . One example, led by a large children’s hospital, provides mobile classroom resources for Title I middle school teachers to enhance STEM education (987)Seattle Children’s. Science Education Partnership Award Program. Accessed: March 31, 2026. .
According to a 2025 congressional report, governmental partners, including the Department of Agriculture, Department of Education, the National Aeronautics and Space Administration, and NSF, and private stakeholders have directly supported K–12 education in rural populations through recruiting and training rural STEM educators to enhance learning and career exploration activities for rural populations (983)US Government Accountability Office. Selected Federal Initiatives, Challenges, and Approaches to Supporting Rural Populations Accessed: March 31, 2026. .
Sustained investment in early education is critical to strengthening the STEM pathway, as it provides foundational skills, exposure, and support that enable students from all backgrounds to pursue advanced training and ultimately contribute to a representative and resilient workforce. Additionally, supporting K–12 teachers is just as critical as providing resources for students, because well-trained, well-supported educators are essential for delivering high-quality instruction, mentoring students, and translating educational investments into meaningful learning opportunities in STEM.
Postsecondary Education
A robust postsecondary educational network that provides flexible, inclusive, and individualized support is essential to expanding participation in STEM pathways beyond K–12. Despite decades of effort, students from certain racial and ethnic minority groups remain underrepresented in STEM degree attainment relative to their share of the US population.
In 2022, only 7.5 percent of bachelor’s degrees and 10.7 percent of associate’s degrees in STEM were awarded to Black students, despite Black individuals comprising 12.1 percent of the total US population. AIAN students represented just 0.3 percent of bachelor’s degrees in STEM awarded in 2022, despite accounting for approximately 0.7 percent of the US population (988)National Center for Education Statistics. Table 318.45. Number and percentage distribution of science, technology, engineering, and mathematics (STEM) degrees/certificates conferred by postsecondary institutions, by race/ethnicity, level of degree/certificate, and sex of student: Academic years 2012-13 through 2021-22. Accessed: March 31, 2026. .
Although Hispanic students have made gains over the past decade—rising from 10.4 percent of STEM degrees in 2013 to 15.6 percent in 2022—they remain substantially underrepresented relative to their population share (988)National Center for Education Statistics. Table 318.45. Number and percentage distribution of science, technology, engineering, and mathematics (STEM) degrees/certificates conferred by postsecondary institutions, by race/ethnicity, level of degree/certificate, and sex of student: Academic years 2012-13 through 2021-22. Accessed: March 31, 2026. . These patterns, resulting from persistent structural barriers within higher education that limit access, retention, and degree completion for underrepresented students, must be addressed to strengthen postsecondary education to better attract, support, and retain students from all backgrounds in STEM (see Sidebar 40).
The federal government has established or expanded initiatives to enhance participation in STEM education programs and create pathways for people from all backgrounds to pursue careers in STEM fields. NSF leads several programs and initiatives aimed at broadening participation, including programs in informal STEM learning, pre-K–12 science education, undergraduate and graduate training in science and engineering, and career support for early-career academic researchers. Many of these programs were created or expanded through provisions of the 2022 Creating Helpful Incentives to Produce Semiconductors (CHIPS) and Science Act, which, as of 2026, has continued to drive billions of dollars of investment in the private sector. The CHIPS and Science Act continues to support historically underserved students and communities by providing new initiatives and funding to Historically Black Colleges and Universities (HBCUs), Minority-Serving Institutions (MSIs), and other academic institutions.
Multiple programs exist to familiarize undergraduate students from underrepresented minority groups with medical and cancer research. Some examples include the Meharry Cancer Summer Undergraduate Research Program, the Synergistic Partnership for Enhancing Equity in Cancer Health’s Summer Cancer Research Institute for undergraduate students, the Continuing Umbrella of Research Experiences program, and the Diversity in Cancer Research Internship National Program. In addition, programs that provide opportunities for undergraduate students conducting laboratory research to present their work at scientific conferences, such as the AACR Undergraduate Student Caucus and Poster Competition and the AACR Undergraduate Scholar Awards, offer early exposure to the cancer research community and help foster sustained engagement in the field. These programs play a critical role in strengthening undergraduate scholars’ interest in cancer research, building foundational scientific knowledge and skills, and preparing students to pursue advanced training and long-term careers in the field (989)Al Hakani MA, et al. (2024) Biochem Mol Biol Educ, 52: 527. (990)Motley-Johnson E, et al. (2025) J Cancer Educ. (991)Zhu L, et al. (2023) PLoS One, 18: e0286279. .
Disparities in STEM education have direct and lasting consequences for the cancer workforce. Because cancer research and care depend on a steady pathway of well-trained scientists, clinicians, and allied health professionals, disparities at early educational stages carry forward into advanced training, faculty roles, clinical specialization, and leadership. Programs that strengthen and diversify this pathway are therefore critical to sustaining the scientific progress, innovation, and long-term success of the cancer research enterprise.
Basic and Translational Cancer Research Workforce Landscape
Basic and translational cancer research aims to improve our understanding of cancer biology and develop new strategies for cancer prevention, detection, diagnosis, and treatment. Basic research focuses on understanding the fundamental mechanisms that underlie cancer development (see Generating Knowledge Through Basic Research), while translational research aims to “translate” the findings into clinical applications that can benefit cancer patients.
Robust representation of all demographic groups in the basic and translational cancer research workforce strengthens cultural competence and relevance, as well as the impact of cancer science, while fostering trust among patients, clinicians, and researchers. A more representative workforce also expands the career pathways by encouraging individuals from underrepresented groups to pursue and sustain careers in STEM, supporting a resilient and innovative cancer research enterprise (992)Davis-Hall D, et al. (2023) Biomed Eng Educ, 3: 23. (993)Kricorian K, et al. (2020) International Journal of STEM Education, 7: 16. .
Laying the groundwork for a career in basic and translational biomedical and cancer research begins with graduate work (master’s or PhD) followed by postdoctoral training. Graduate students and postdoctoral fellows form the foundation of the cancer research workforce, conducting the majority of basic and translational research, and most carry out their work in academic institutions, including universities and university hospitals.
Graduate student enrollment in the biological and biomedical sciences field is robust, representing 20 percent of all doctoral students in the United States in 2022, the most recent year for which data are available (994)National Science Foundation. Table 3. Enrollment of master’s students and doctoral students in science, engineering, and health, by field: 2018–22. Accessed: March 31, 2026. . Further, biological and biomedical science programs had an increase of 1.5 percent in graduate student enrollment in 2025 compared to 2024, although this was lower than the 4.0 percent increase in enrollment seen the previous year (995)National Student Clearinghouse Research Center. Clearinghouse Enrollment Insights Series: Clearinghouse Final Fall Enrollment Trends. Accessed: March 31, 2026. . The racial and ethnic composition of these programs does not reflect that of the overall US population. Data from 2023 showed that Black (6.2 percent), Hispanic (10.5 percent), and AIAN (0.3 percent) students remained underrepresented in biological and biomedical sciences graduate programs (996)National Science Foundation. Table 4-4a. Citizenship, ethnicity, and race of graduate students, by detailed field: 2023. Accessed: March 31, 2026. .
International graduate students and postdoctoral fellows who come to the United States for training are foundational to biomedical research productivity. They conduct a substantial share of laboratory experiments, data analysis, and translational work in US academic research settings. In 2024, 26 percent of graduate students in the biological and biomedical sciences field were foreign nationals holding temporary visas and the majority of postdoctoral researchers in science, engineering, and health fields (58.3 percent) required a temporary visa (997)National Science Foundation. Graduate students in science, engineering, and health broad fields, by degree program, citizenship, ethnicity, and race: 2024. Accessed: March 31, 2026. (998)National Science Foundation. Citizenship of graduate students and postdoctoral appointees in science, engineering, and health: 1980–2024. Accessed: March 31, 2026. .
Several types of visas can be granted to international scholars. The H1-B visa is a nonimmigrant, employer-sponsored visa typically granted for up to 6 years and is widely used for highly skilled professionals such as postdoctoral scholars, junior faculty members, and long-term researcher positions. H1-B visa holders can also apply for permanent residency (i.e., a green card) to remain in the US workforce. On September 19, 2025, an executive order significantly increased the fee for new H1-B visa petitions to $100,000, discouraging recruitment of international trainees (999)The White House. Restriction on Entry of Certain Nonimmigrant Workers. Accessed: March 31, 2026. , with substantial adverse implications for the STEM workforce and long-term leadership of the nation in innovative and cutting-edge science.
Increasing barriers to recruiting trainees into medical research will reduce research productivity, weaken scientific competitiveness for the United States, and exacerbate existing workforce shortages. Subsequently, this will disproportionately affect researchers who are already facing funding constraints, particularly early-career cancer researchers.
Another concern is that PhD recipients in the United States are less likely to pursue postdoctoral positions in academia than they were two decades ago, decreasing the number of future researchers. Data from the National Center for Science and Engineering Statistics show a steady decline in the proportion of biomedical sciences PhD recipients entering postdoctoral training, driven in part by increased movement into industry positions. In 2024, 52 percent of PhD recipients in biological and biomedical sciences accepted jobs in industry or business—nearly double the proportion in 2004, when 28 percent pursued industry careers (1000)National Science Foundation. Definite non-postdoc employment commitments in industry or business in the United States, by trend broad field: 2004–24. Accessed: March 31, 2026. .
Persistent attrition at this career stage threatens the continuity of basic and translational academic research pipelines. While biopharmaceutical industry careers play an important and complementary role in medical innovation, the declining proportion of trainees pursuing academic research positions raises concerns for the sustainability of the academic cancer research enterprise. Academic laboratories remain uniquely positioned to pursue high-risk, long-term, and discovery-driven cancer research that may not align with short-term commercial incentives of the private sector.
Early-stage Investigators
Recruiting and retaining a robust cancer research workforce beyond the postdoctoral stage is a pivotal challenge for the biomedical research community. Prospective tenure-track investigators must rapidly transition from a mentored training environment to functioning as fully independent, self-sustaining researchers. The first 5 years of this transition are especially consequential, as early-stage investigators work to establish their independent research programs, secure laboratory infrastructure, build professional collaborations and networks, and generate the preliminary data needed for long-term success. Access to reliable and timely federal funding during this period is critical.
NIH career development and research awards play a central role in enabling this transition, with mechanisms such as the K99/R00 Pathway to Independence Award supporting the transition from postdoctoral training to independent faculty positions, and the R01 serving as the primary source of sustained research support once independence is achieved. Limited access to R01 funding can constrain laboratory growth, reduce competitiveness for promotion and tenure, and increase attrition from academic research careers.
Historically, women have been underrepresented among recipients of NIH R01 grants compared to men, reflecting long-standing gender disparities in access to sustained federal research funding. Although the proportion of R01 awards granted to women has increased over time, gaps persist across many scientific fields (1002)Chaudhary AMD, et al. (2021) Cureus, 13: e14930. . For example, one study found that only 27 percent of the nearly 1,500 R01 grants awarded in gastrointestinal oncology during the fiscal years of 2018–2021 were awarded to women, highlighting continued inequities in highly specialized areas of cancer research (1003)Khan S, et al. (2024) Journal of Clinical Oncology, 42: 763. .
In early 2025, more than 2,200 active research grants—representing $2.45 billion in funding—were prematurely terminated, with the majority of these cancellations affecting academic medical centers. Data indicate that women researchers had a larger share of active resources at the time of grant cancellation (57.9 percent vs. 48.2 percent), meaning that they experienced a greater disruption of active research and personnel support. As a result, women lost a greater portion of unrealized scientific output. Most concerning, among early-stage investigators (i.e., assistant professors), projects led by women were disproportionately more likely to be terminated than those led by their male counterparts (1004)Oliveira DFM, et al. (2026) Proc Natl Acad Sci U S A, 123: e2527755123. .
Substantial disparities persist in the receipt of NIH funding by Black scientists, with important implications for fairness, scientific innovation, and the long-term sustainability of the biomedical workforce. One study found that in 2021, a Black applicant’s odds of receiving at least one new R01 research grant was 24 percent lower compared to a White applicant (1005)Science Magazine. NIH launches grant program aimed at closing the funding rate gap between Black and white investigators. Accessed: March 31, 2026. . Both early-career (e.g., K99/R00) and independent (e.g., R01) research grants are disproportionately concentrated among researchers at high-profile, research-intensive “legacy” institutions, while comparatively few awards are made to investigators at HBCUs and other MSIs. Notably, an analysis of NIH data from 2006–2022 found no K99 awards had been granted to investigators based at HBCUs (1006)Woitowich NC, et al. (2024) Elife, 12. .
Because NIH grants are foundational to establishing and sustaining independent research programs, reduced access to these funding mechanisms for underrepresented researchers can compound disadvantages over time. Limited success in securing early-career awards reduces competitiveness for subsequent R01 funding, constrains laboratory growth, and narrows opportunities for promotion, tenure, and leadership. These funding gaps contribute to higher attrition from academic research careers and limit the diversity of perspectives shaping cancer science and medicine. Addressing disparities in NIH funding allocation is therefore critical for strengthening the cancer research enterprise by ensuring that talent, innovation, and leadership are drawn from the full breadth of the nation’s scientific workforce.
Within NCI, the Center to Reduce Cancer Health Disparities (CRCHD) is leading initiatives to train the next generation of students, researchers, and physician-scientists to ensure a robust research workforce for decades to come (see Sidebar 41). Over the past four decades, under the leadership of Sanya A. Springfield, PhD, CRCHD has offered various pathways across the academic cancer research continuum that have proven effective in addressing career development gaps through a holistic and multilevel approach.
NIH and NCI must continue to support stable, predictable funding mechanisms for early-stage investigators from all sociodemographic backgrounds, as this transition period is marked by intense competition and funding uncertainty that disproportionately affects underrepresented researchers. Targeted career development awards, sustained research support, and loan repayment programs are essential to prevent attrition and to build a diverse, resilient cancer research workforce capable of advancing innovation and equity.
Established Investigators
Transitioning into senior roles at academic institutions and medical centers is critical, as these positions confer greater influence over research priorities, institutional decision-making, mentorship, and resource allocation, thereby shaping the direction of science, clinical practice, and the training of future generations.
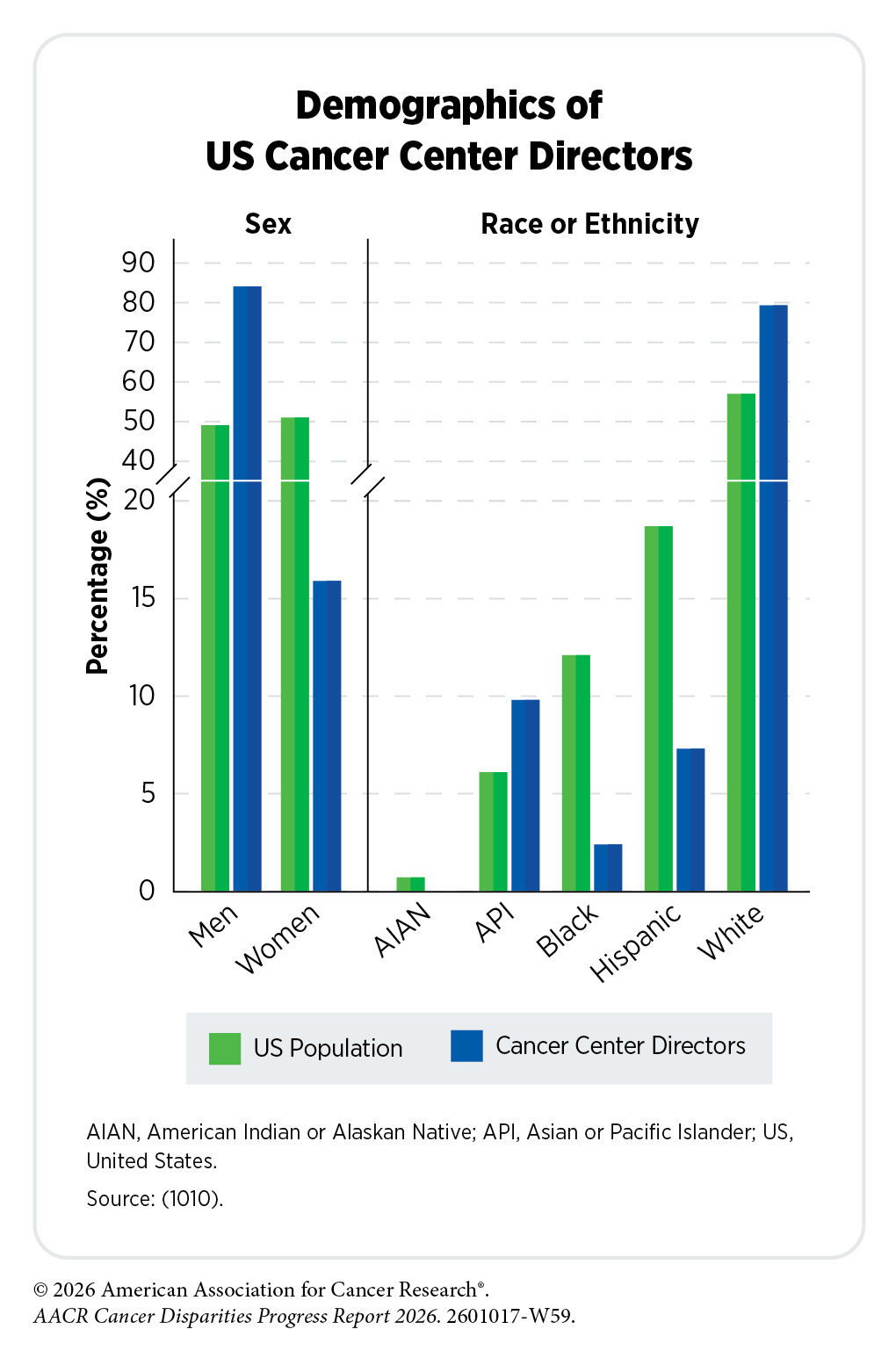
Several studies have demonstrated unequal representation of women and racial and ethnic minority populations in higher positions of academia, including in cancer science and medicine (1007)Levy MS, et al. (2025) JAMA Netw Open, 8: e252829. (1008)Krischak MK, et al. (2025) Cancer, 131: e35690. (1009)Li CI, et al. (2024) J Natl Cancer Inst, 116: 1198. (1010)Lerman C, et al. (2022) JNCI, 114: 1214. . There are also disparities in median annual salaries among tenure track professors at medical institutions. One study found that women faculty earned less than men and those belonging to groups historically underrepresented in medicine earned up to 20 percent less than White men (1011)Owda D, et al. (2025) JAMA Netw Open, 8: e259583. .
Underrepresentation at these levels perpetuates inequities across the entire workforce, limiting opportunities for diverse trainees and reinforcing systemic barriers that extend well beyond individual career trajectories. A poll conducted after funding disruptions in 2025 found that nearly 75 percent of the more than 1,600 surveyed US scientists had considered leaving the United States (1012)Witze A (2025) Nature, 640: 298. . Reflecting growing concerns about a potential research “brain drain,” several countries have since begun offering US researchers grants and institutional support to relocate and continue their work abroad (1013)Udesky L, et al. (2025) Nature. (1014)Gibney E, et al. (2026) Nature. .
Recent policy changes have further destabilized the US research environment by constraining international collaboration. In mid-2025, NIH announced restrictions on US investigators’ ability to issue international sub-awards—where a primary recipient of a grant passes a portion of the funds to a subrecipient to carry out part of a sponsored project’s programmatic work—through federally funded grants. In a survey of nearly 1,000 NIH-supported scientists, 15 percent of respondents reported their grants were terminated, 45 percent experienced delays, 34 percent had funding temporarily paused or frozen, 34 percent had their grant amounts reduced, and 32 percent reported grant programs were canceled (1015)STAT. STAT NIH-funded researcher survey. Accessed: March 31, 2026. .
Disruptions to research as a result of recent policy changes are also being reported by cancer disparities-focused researchers. A 2026 AACR survey found that 93 percent of respondents reported impacts to their research following recent diversity, equity, and inclusion (DEI)-related policy changes. Among those surveyed, 51 percent were senior investigators (i.e., professor or associate professor) and nearly 22 percent were early-stage investigators. Notably, 56 percent indicated they are considering or have already shifted their research focus away from cancer disparities.
AACR Survey of Cancer Disparities Researchers: View the ResultsRobust and sustained federal investment in research grants is essential to maintaining US scientific leadership and competitiveness in an increasingly global research landscape. Without stable funding, the United States risks losing talent, slowing innovation, and ceding its long-standing role as the world’s leading engine of scientific discovery and medical advances.
Cancer Care Training and Workforce Landscape
Physicians
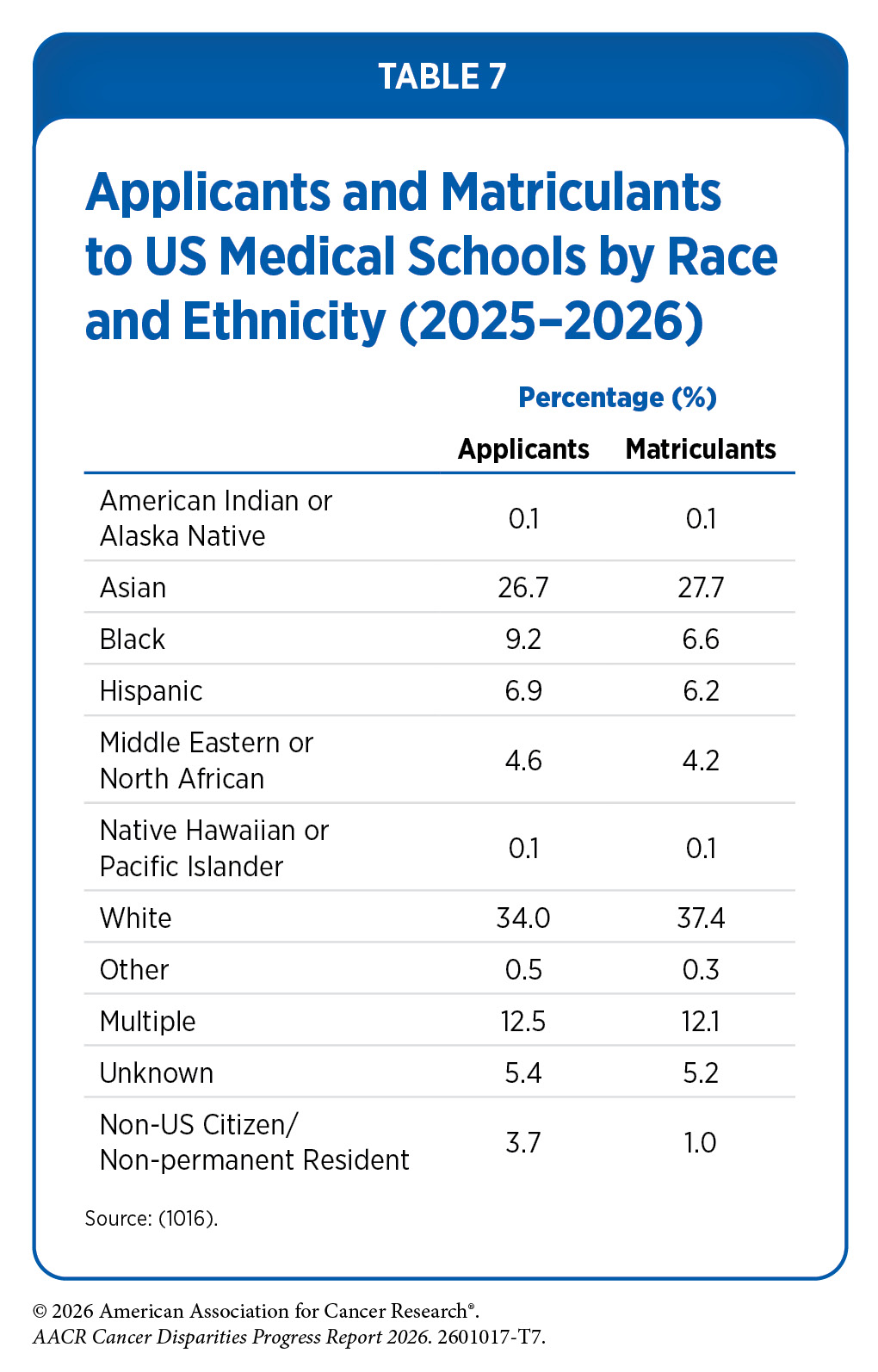
Disparities in the physician workforce are attributable to disparities earlier on in the medical education pathway. Despite comprising a substantial share of the US population, several racial and ethnic groups remain underrepresented among medical school applicants and matriculants (i.e., those who became enrolled in medical school), reflecting persistent inequities in the medical education pipeline. In 2020, Black individuals made up 12.1 percent of the total US population, but only 9.2 percent of medical school applicants and 6.6 percent of medical school matriculants in 2025 identified as Black (see Table 7). Similarly, Hispanic individuals made up 18.7 percent of the total population in 2020, but only 6.9 percent of medical school applicants and 6.2 percent of medical school matriculants in 2025 identified as Hispanic. AIAN individuals made up 0.7 percent of the total population in 2020, but only 0.1 percent of medical school applicants and matriculants in 2025 identified as AIAN.
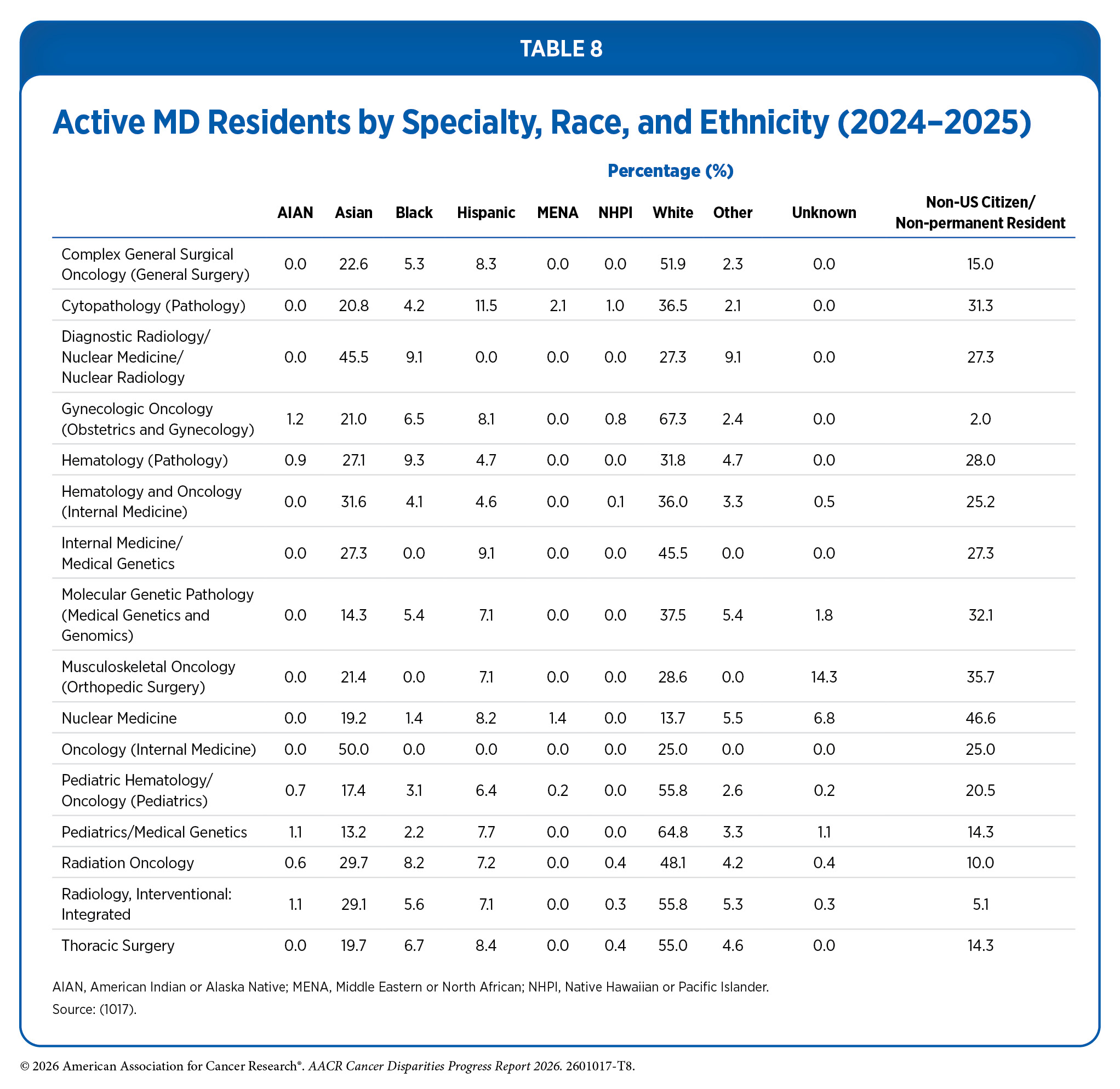
Despite many diversity initiatives over the past 10 years, underrepresentation of racial and ethnic minority populations, SGM groups, and individuals from low socioeconomic status continues in the oncology training pathway and workforce. Between 2024 and 2025, on average, just 4.4 percent, 6.6 percent, 0.4 percent, and 0.2 percent of medical residents were Black, Hispanic, AIAN, and Native Hawaiian or Pacific Islander (NHPI), respectively (see Table 8).
The Association of American Medical Colleges reports that the proportion of applications from Hispanic and AIAN individuals has grown from 11.9 percent to 12.3 percent and 11.3 to 11.7 percent, respectively, between academic years 2023–2024 and 2024–2025, while the proportion of applications from AIAN individuals decreased from 1.1 percent in academic year 2023–2024 to 1.0 percent in academic year 2024–2025. Of concern, the proportion of matriculants from AIAN, Black, and Hispanic individuals declined from academic years 2023–2024 to 2024–2025 (1018)Association of American Medical Colleges. 2025 Fall Applicant, Matriculant, and Enrollment Data Tables. Accessed: March 31, 2026. .
Exacerbating these declines are decisions by the US Supreme Court in June 2023 that curtailed the use of race-based considerations in admissions and led to the elimination or restructuring of DEI programs in medical schools.
In response, many medical schools have paused, scaled back, or re-evaluated outreach, pipeline, and scholarship programs while seeking legal clarity and new compliance frameworks. This period of uncertainty has disrupted institutional efforts and has, in part, contributed to the declines in matriculation among Black and Hispanic individuals, as noted above.
Despite these declines, medical school enrollment is more diverse now than a decade ago. Furthermore, women made up 56.8 percent of applicants, 55.1 percent of matriculants, and 54.9 percent of the total enrollment in medical schools in the 2024–2025 academic year (1019)Association of American Medical Colleges. New AAMC Data on Medical School Applicants and Enrollment in 2024. Accessed: March 31, 2026. .
Because oncology training consists of a long, highly specialized pathway, declines in medical school matriculation among underrepresented groups today will adversely impact the oncology workforce a decade or more into the future. Fewer students entering medical school from diverse backgrounds ultimately translate into fewer residents, fellows, and attending oncologists, with disproportionate effects on communities already facing barriers to cancer care. These trends underscore the importance of maintaining legally sustainable pathways that preserve access, opportunity, and diversity within medical education.
The geographic distribution of the oncology workforce further compounds disparities in access to care, particularly for individuals living in rural areas. A recent study found that by 2037, nonmetropolitan areas are projected to meet only 29 percent of their demand for oncologists, compared to 102 percent in metropolitan areas. Early-career oncologists are also less likely to practice in nonmetropolitan areas, suggesting that these geographic gaps may widen over time (596)Kirkwood MK, et al. (2025) JCO Oncol Pract, 21: 1775. .
A growing body of evidence shows that racial concordance between patients and clinicians—defined as a shared racial or ethnic identity with the patient–provider relationship—is associated with improved communication, greater patient trust, increased treatment adherence, and better survival-related outcomes (659)Loeb S, et al. (2023) JAMA Netw Open, 6: e2324395. (1020)Fang P, et al. (2018) Adv Radiat Oncol, 3: 221. (1021)Ku L, et al. (2023) J Gen Intern Med, 38: 727. (1022)Shen MJ, et al. (2018) J Racial Ethn Health Disparities, 5: 117. . These effects are particularly pronounced for Black patients, among whom racial concordance has been linked to reduced disparities in health outcomes, including lower all-cause mortality rates.
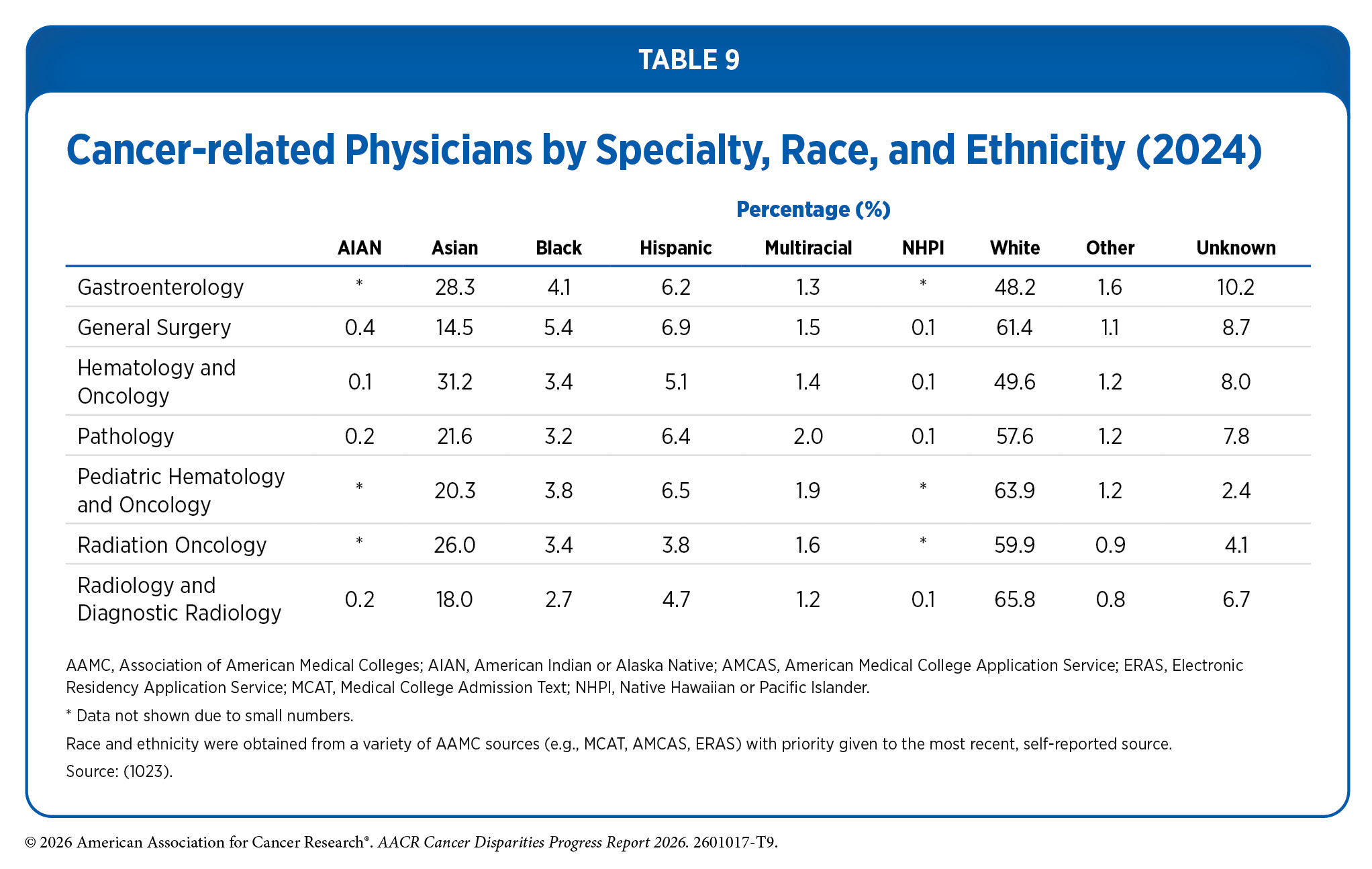
However, Black physicians remain chronically underrepresented in oncology, comprising between 2.6 percent and 5.4 percent of the oncology workforce (see Table 9). Increasing the number of Black oncologists will require medical schools to recognize and address the structural barriers that shape educational and professional pathways for Black students—barriers that are persistent, cumulative, and rooted in generations of systemic inequity. Strengthening and sustaining these pathways will require early and intentional investment, including partnerships with undergraduate institutions, particularly HBCUs, to identify, support, and mentor promising Black students who may pursue careers in medicine and oncology.
Similarly, oncologists who identify as Hispanic remain highly underrepresented in the workforce. While the Hispanic population is the largest minority group in the United States, constituting approximately 18.7 percent of the total population, only 6.2 percent of matriculating medical school students self-identify as Hispanic (see Table 7), and between 3.7 percent and 6.6 percent of cancer-related physicians in the United States in 2023 self-identify as Hispanic (see Table 9).
Mentoring and training future physicians from diverse backgrounds is key to addressing cancer health disparities. Efforts led by professional societies represent an important avenue for advancing initiatives to diversify the health care workforce. In 2019, the American Medical Association (AMA) established the Center for Health Equity, which continues to lead initiatives focused on diversifying the cancer workforce and promoting health equity. These initiatives include toolkits, resources, educational centers, and video series that provide information about social drivers of health, health equity, and racial justice, as well as legislative efforts to advocate for health equity policies. In their 2024–2025 strategic plan, the AMA reaffirmed their commitment to advocate for equity and racial justice in health care.
Physician-scientists
Physician-scientists occupy a unique and critical niche in cancer research, working across the full continuum from basic discovery to clinical translation and real-world implementation. Their training typically spans medical school, residency, and fellowship, and often includes advanced research training, either through a formal research degree (e.g., a PhD) or substantial mentored research experience. With this extensive and interdisciplinary preparation, physician-scientists are uniquely positioned to translate discoveries from the bench to the bedside, bridging a long-standing and essential gap between laboratory research and patient care.
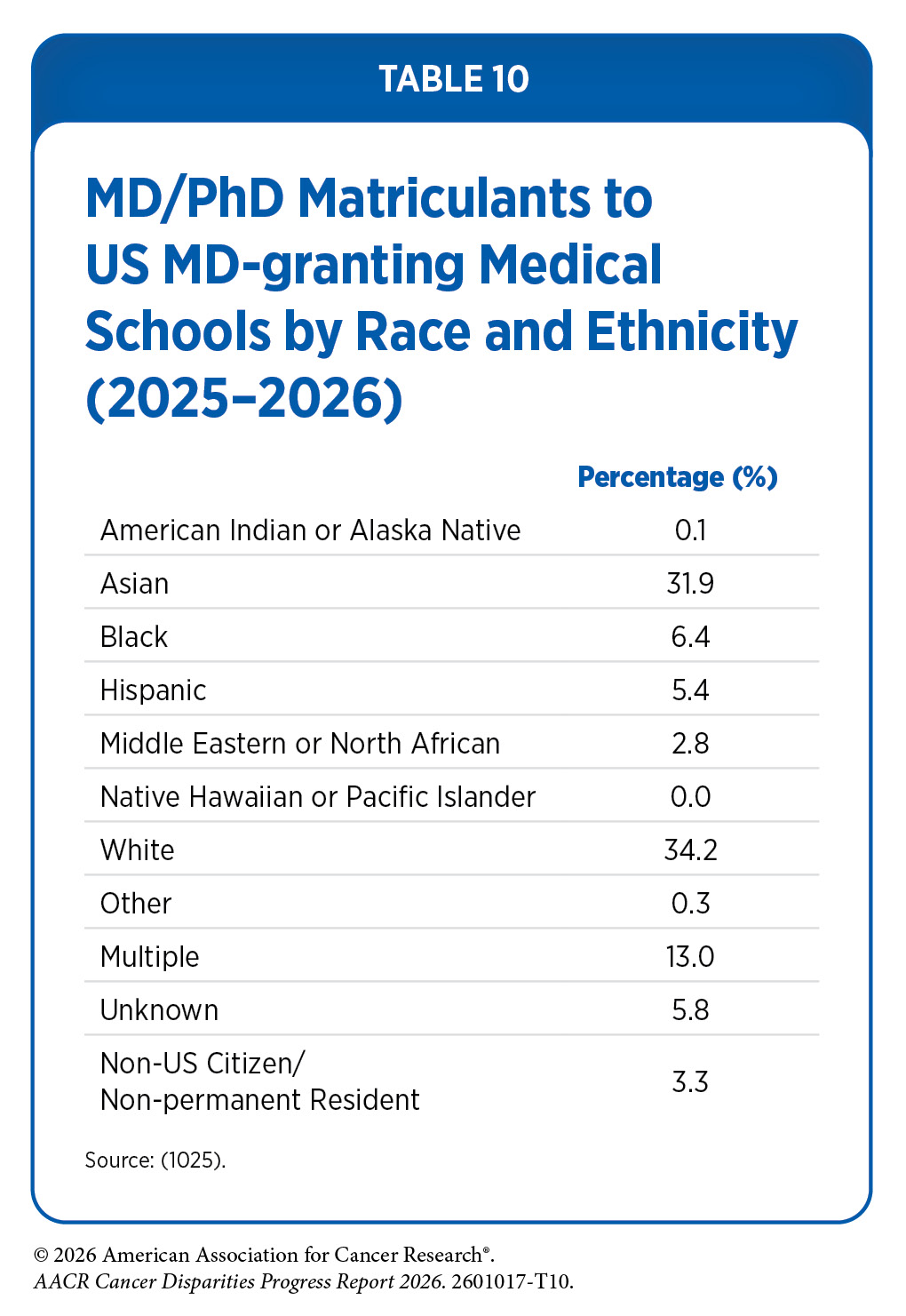
One pathway to becoming a physician-scientist is through enrollment in an MD/PhD program, which combines graduate and medical school into programs typically lasting 7–8 years. Despite making up 12.1 percent of the US population, only 6.4 percent of matriculants to US MD/PhD programs were Black (see Table 10). These gaps also exist for Hispanic individuals, who represent 18.7 percent of the population but only 5.4 percent of matriculants to MD/PhD programs. Additionally, there were no NHPI matriculants to MD/PhD programs in 2025.
Beyond limited entrance in MD/PhD programs, one study found that Black MD/PhD matriculants are more likely to leave medical school or to complete their training without earning the PhD component of the degree compared to White individuals who enter a MD/PhD program (1026)Nguyen M, et al. (2023) JAMA Intern Med, 183: 1021. . Black physician-scientists were also less likely to be awarded NIH grants, have lower rates of conversion from training K awards (e.g., K08) to R awards (e.g., R01), and were more likely to have entered nonacademic clinical practice, compared to White physician-scientists (1027)Akabas MH, et al. (2024) JCI Insight, 9. .
Closing disparities in the physician-scientist pipeline strengthens the translation of biomedical discoveries into clinical care, expands the range of research questions addressed, and ensures that cancer research and innovation reflect and serve the full diversity of patients and communities.
Other Health Care Professionals
While physicians and physician-scientists play central roles in cancer research and care, the effectiveness of the cancer care continuum depends equally on a diverse range of other health professionals who support disease diagnosis, treatment adherence, symptom management, and survivorship care. Comprehensive cancer care teams—including physician assistants, nurse practitioners, registered nurses, dieticians, pharmacists, community health workers, patient navigators, and other care partners—are essential to care coordination and patient trust. As cancer increasingly becomes a chronic condition requiring long-term management, sustained access to representative and well-trained care teams is critical to improving outcomes and ensuring equitable, patient-centered cancer care.
Nurses and nurse navigators are crucial to symptom management and improving outcomes and treatment adherence for patients (see Vital Role of Patient Navigation and Community Engagement). Furthermore, improved outcomes are seen for patients when patient navigators have similar racial or ethnic backgrounds or speak the same language as the patients they serve (1028)Jang J, et al. (2025) J Gen Intern Med, 40: 2358. (1029)Mazor M, et al. (2025) Cancer, 131: e35745. (1030)Tom A, et al. (2025) J Health Equity, 2. .
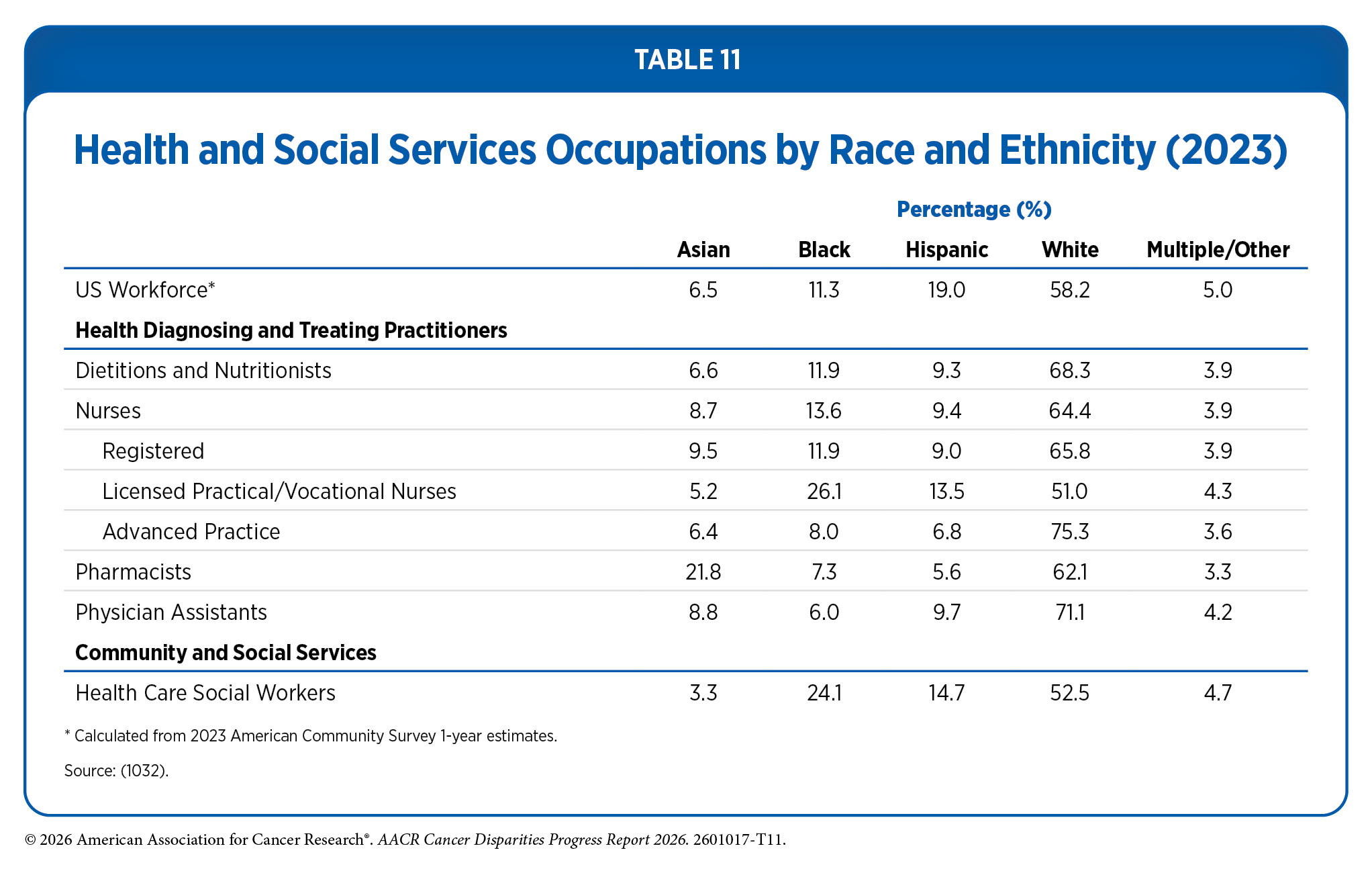
However, the cancer care workforce often does not reflect the patient populations it serves (see Table 11). In a study of 574 hospitals in the United States, Black nurses comprised only 5.3 percent of the workforce, compared to 11.2 percent of hospitalized patients identifying as Black. This disparity was most pronounced at certain hospitals serving a high proportion of Black patients, where the gap between the proportions of Black nurses and Black patients reached nearly 17 percentage points (1031)Lake ET, et al. (2025) Nurs Res, 74: 405. .
A significant portion of personnel in health care settings are noncitizen immigrants. One study found that noncitizen immigrants accounted for approximately 4 percent of personnel in hospitals and outpatient settings, 7 percent of nursing home workers, and at least 10 percent of workers in home care agencies; however, these are estimates and are likely on the low end, as these workers are either undocumented or filling temporary roles (1033)Azaroff LS, et al. (2025) JAMA, 333: 2018. . Recent immigration policy changes—including increased immigration enforcement, expedited removal, denaturalization efforts, pauses on visas, and travel bans—pose a severe threat to these essential workers in the health care workforce. Because these policies are recent, their effect on cancer care is not yet known; however, because these supportive services are already chronically short staffed, loss of personnel could have severe long-term repercussions.
Across research, training, and care delivery, workforce diversity is inseparable from the nation’s ability to advance cancer science and deliver equitable, high-quality care. Strengthening educational pipelines, stabilizing early-career funding, expanding leadership representation, and protecting the roles of the full cancer care team are mutually reinforcing strategies essential to building a cancer workforce that is innovative, resilient, and capable of meeting the needs of an increasingly diverse population.
Next Section: Overcoming Cancer Disparities Through Science-Based Public Policy Previous Section: Disparities in Cancer Survivorship