Understanding And Addressing Drivers of Cancer Disparities
In this section, you will learn:
- A long history of structural inequities and social injustices has shaped current neighborhood conditions that can influence cancer risk, access to care, and outcomes.
- Structural and social factors such as residential segregation, environmental exposures, transportation access, food environments, and neighborhood disinvestment contribute to cancer disparities by influencing access to screening and treatment, and exposure to modifiable risk factors.
- Disproportionately high exposure to stressors linked to social and environmental disadvantage among certain populations affects physiologic systems—including immune and inflammatory pathways, epigenetic regulation, and gene expression—in ways that contribute to disparities in cancer development and progression.
- Policy‑level interventions, including national and state initiatives (e.g., insurance expansion and cancer screening programs), together with community‑based programs like transportation support and food or housing assistance, have been shown to mitigate upstream social barriers to cancer prevention and care leading to reduction in cancer disparities.
Contents
Disparities in health and cancer outcomes in the United States (US) reflect the cumulative effects of racism, segregation, and ongoing structural and social challenges that have disproportionately affected marginalized populations over generations. Disparities in access to resources, opportunities, and conditions that support health and well‑being are increasingly recognized as central contributors to population‑level differences in health outcomes. In 2003, the Institute of Medicine, under mandate from the US Congress, issued the landmark report Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care (99)Institute of Medicine (US) Committee on Understanding and Eliminating Racial and Ethnic Disparities in Health Care. Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care. Smedley BD, Stith AY, Nelson AR, editors. Washington (DC): National Academies Press (US); 2003. PMID: 25032386, which systematically documented persistent racial and ethnic disparities across the health care system. The report concluded that while socioeconomic factors such as income, education, and access to care are important contributors, systemic and structural racism plays a critical role in sustaining these disparities in the United States (99)Institute of Medicine (US) Committee on Understanding and Eliminating Racial and Ethnic Disparities in Health Care. Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care. Smedley BD, Stith AY, Nelson AR, editors. Washington (DC): National Academies Press (US); 2003. PMID: 25032386.
Disparities driven by structural racism, broader societal inequities, and contemporary injustices are evident across multiple measures of health, including across the cancer continuum, and are particularly pronounced among racial and ethnic minority groups and other medically underserved populations. In this section, we describe key drivers of cancer disparities in the United States, including social drivers of health, and summarize selected initiatives and programs that seek to mitigate these disparities. Together, these efforts underscore ongoing strategies to reduce cancer disparities and advance progress toward health equity.
Drivers of Health Disparities
A range of conceptual frameworks have been developed to characterize the multiple influences on health outcomes and to explain the origins and persistence of health disparities, including disparities in cancer (100)Committee on Educating Health Professionals to Address the Social Determinants of Health; Board on Global Health; Institute of Medicine; National Academies of Sciences, Engineering, and Medicine. A Framework for Educating Health Professionals to Address the Social Determinants of Health. Washington (DC): National Academies Press (US); 2016 Oct 14. 1, Introduction. (101)Krieger N (2012) Am J Public Health, 102: 936. (102)Krieger N (1999) Int J Health Serv, 29: 295. (103)Alvidrez J, et al. (2019) Am J Public Health, 109: S16. (104)Asare M, et al. (2017) Oncol Nurs Forum, 44: 20. (105)Winkfield KM, et al. (2021) JCO Oncology Practice, 17: e278. . These frameworks consistently emphasize that health outcomes are shaped by a complex, interconnected system of factors that extend beyond clinical care. Such factors include structural factors that influence biological, psychosocial, and modifiable risk factors, as well as nonclinical influences commonly referred to as social drivers of health (SDOH) (104)Asare M, et al. (2017) Oncol Nurs Forum, 44: 20. (105)Winkfield KM, et al. (2021) JCO Oncology Practice, 17: e278. (106)Warnecke RB, et al. (2008) Am J Public Health, 98: 1608. .
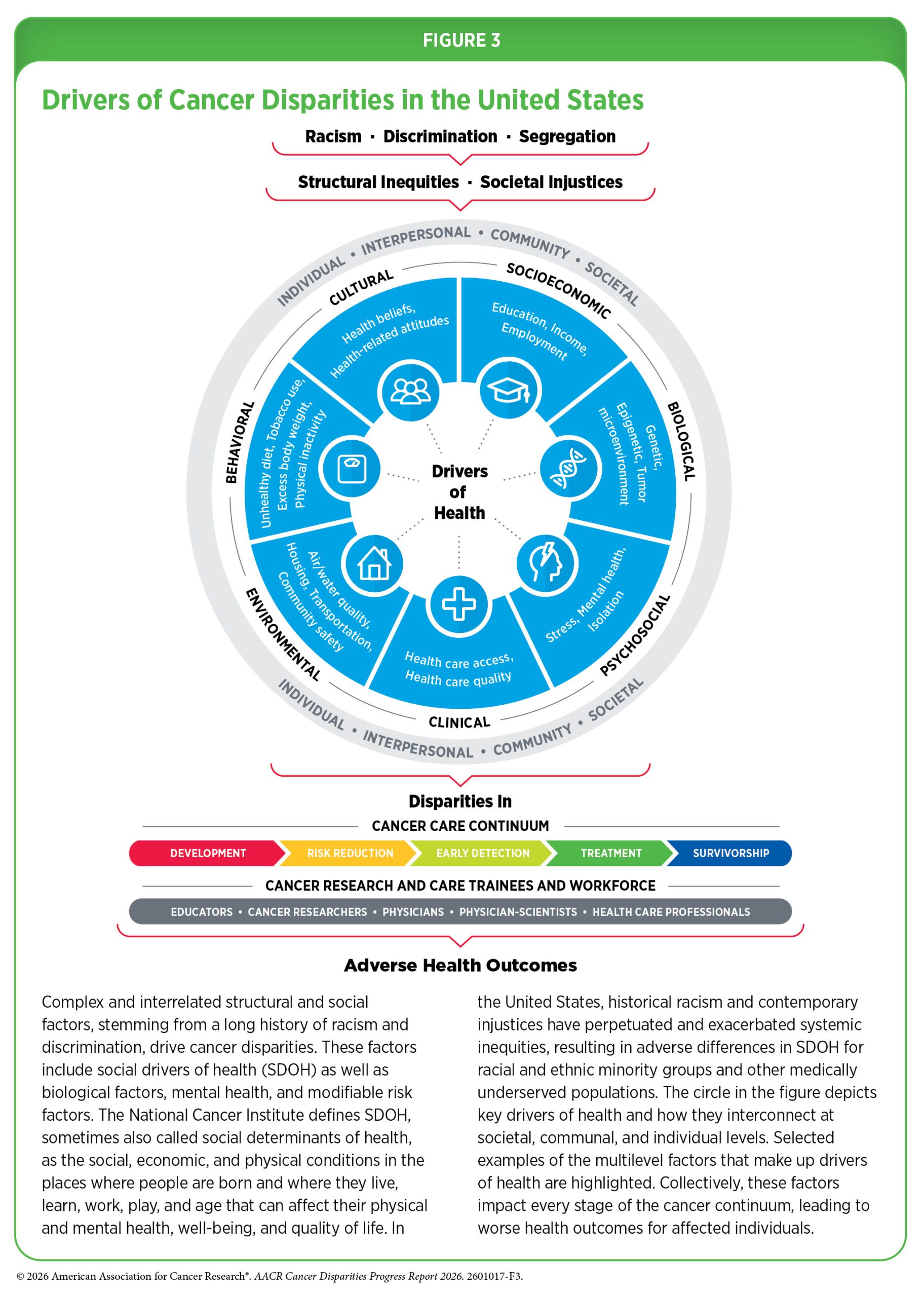
The National Cancer Institute (NCI) defines SDOH—also referred to as social determinants of health—as the social, economic, and physical conditions in the environments where individuals are born and where they live, learn, work, play, and age, all of which can influence health, well‑being, and quality of life. These drivers encompass a wide range of factors, including income, education, housing, transportation, neighborhood conditions, and access to healthy food, fresh air, clean water, and health care services. Importantly, SDOH do not operate in isolation; rather, they interact across individual, community, and societal levels and over the life course to shape lived experiences and health trajectories (see Figure 3).
The influence of SDOH on cancer risk and outcomes can be observed across the cancer continuum. For example, access to balanced and nutritious diets is associated with improved overall health and reduced risk for several chronic conditions, including cancer (107)Bui LP, et al. (2024) Am J Clin Nutr, 120: 80. (108)Cai Y, et al. (2024) Am J Clin Nutr, 119: 406. (109)Fraser GE, et al. (2025) Am J Clin Nutr, 122: 535. . Conversely, limited access to affordable healthy food options increases the likelihood of adverse health outcomes and contributes to observed cancer disparities (see Disparities in the Burden of Modifiable Behavioral Cancer Risk Factors) (110)Morales-Berstein F, et al. (2024) Eur J Nutr, 63: 377. (111)Odoms-Young A, et al. (2024) The American Journal of Clinical Nutrition, 119: 850. . In such contexts, informational or educational interventions alone are often insufficient, particularly in communities that lack nearby grocery stores, experience high levels of crime or violence, or face economic barriers that limit the affordability of healthy foods.
Addressing these challenges requires coordinated, multisector approaches that extend beyond health care, involving sectors such as education, transportation, labor, housing, and justice to improve both access to and affordability of health‑promoting resources, while also supporting awareness of health benefits. Ongoing research continues to elucidate the multilevel and cumulative effects of SDOH on individuals, communities, and populations. In this section, we highlight selected examples of key health drivers, including SDOH, and examine their contributions to cancer disparities experienced by racial and ethnic minority groups and other medically underserved populations in the United States.
Structural Inequities and Social Injustices
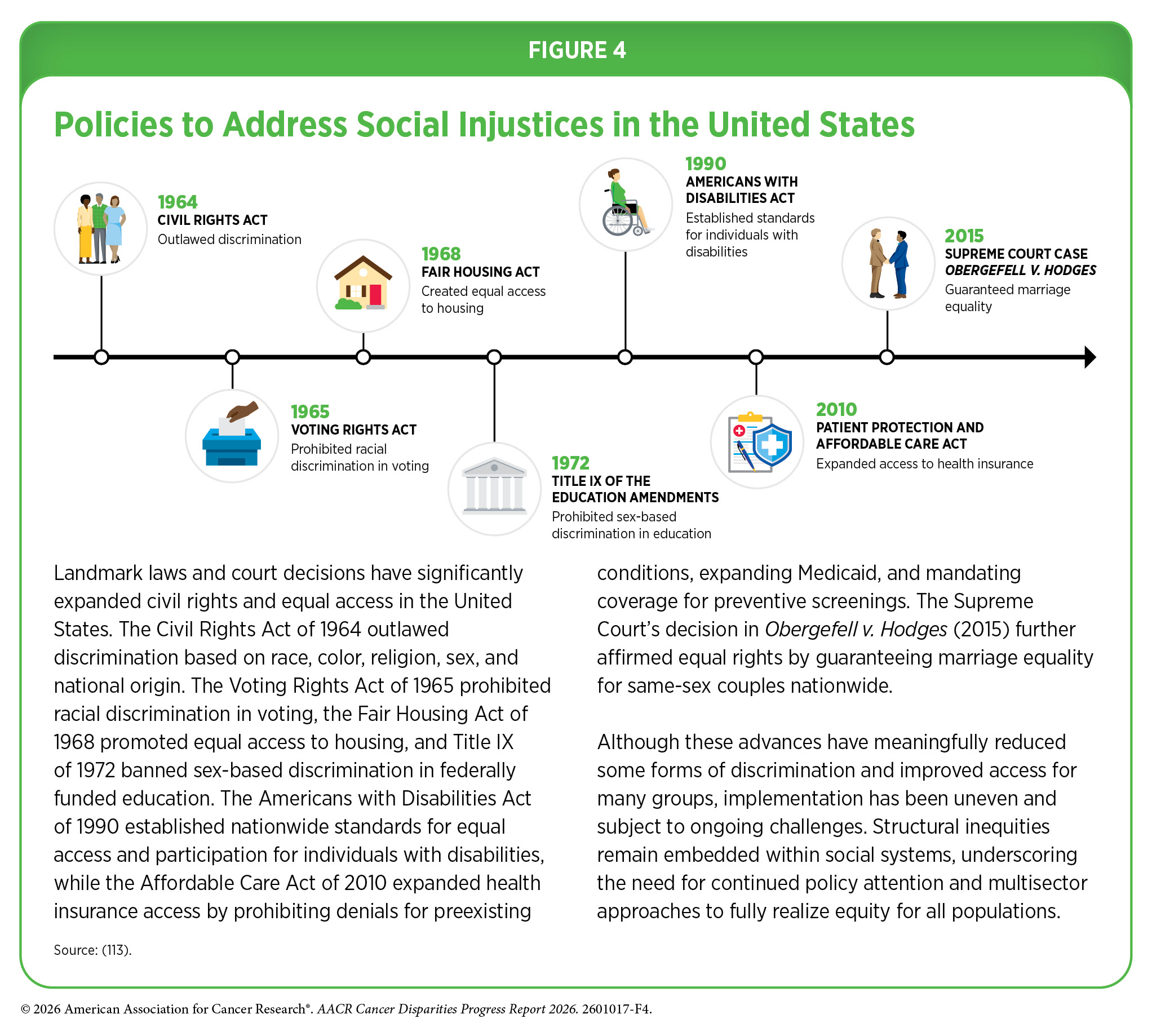
In the United States, contemporary structural inequities and social injustices are rooted in legacies that date back to European colonization. Beginning in the 16th century, a succession of laws, policies, and social practices—including chattel slavery; the displacement and forced removal of American Indian and Alaska Native peoples; denial of citizenship and land rights of Native Hawaiian or Pacific Islander individuals; the systematic suppression of women’s rights; Jim Crow segregation; periods of nativist legislations against and mass deportations of Hispanic immigrants; eugenics movements; the internment of Japanese American individuals during World War II; anti‑Chinese immigration policies; and the criminalization of same‑sex relationships—profoundly shaped social hierarchies and patterns of exclusion. Collectively, these actions established and reinforced inequities that continue to influence social, economic, and health outcomes across generations. Although many policies have been enacted over the past 60 years to mitigate the effects of historic inequities (see Figure 4), the legacy of discriminatory practices remains embedded in present‑day social structures, influencing SDOH and population‑level outcomes.
Structural inequities and social injustices shape SDOH through historical and contemporary policies that unevenly distribute social and economic resources across populations. Structural inequities refer to entrenched, system‑level patterns that advantage some social groups while systematically disadvantaging others within the same society. These inequities are embedded across multiple domains, including policies, laws, governance structures, and cultural norms, and operate along dimensions such as race, ethnicity, socioeconomic position, sexual orientation, gender identity, and other social identities. Structural inequities produce persistent and patterned disadvantages that shape unequal exposures to SDOH and, in turn, contribute to differences in health outcomes across populations (113)National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Board on Population Health and Public Health Practice; Committee on Community-Based Solutions to Promote Health Equity in the United States. Communities in Action: Pathways to Health Equity. Baciu A, Negussie Y, Geller A, Weinstein JN, editors. Washington (DC): National Academies Press (US); 2017 Jan 11. PMID: 28418632(114)Schaefer A, et al. (2025) Current Epidemiology Reports, 12: 7. . More work is needed to better characterize these pathways that drive health, improve their measurement, and develop effective interventions to mitigate their impact on health inequities.
Social and Built Environments
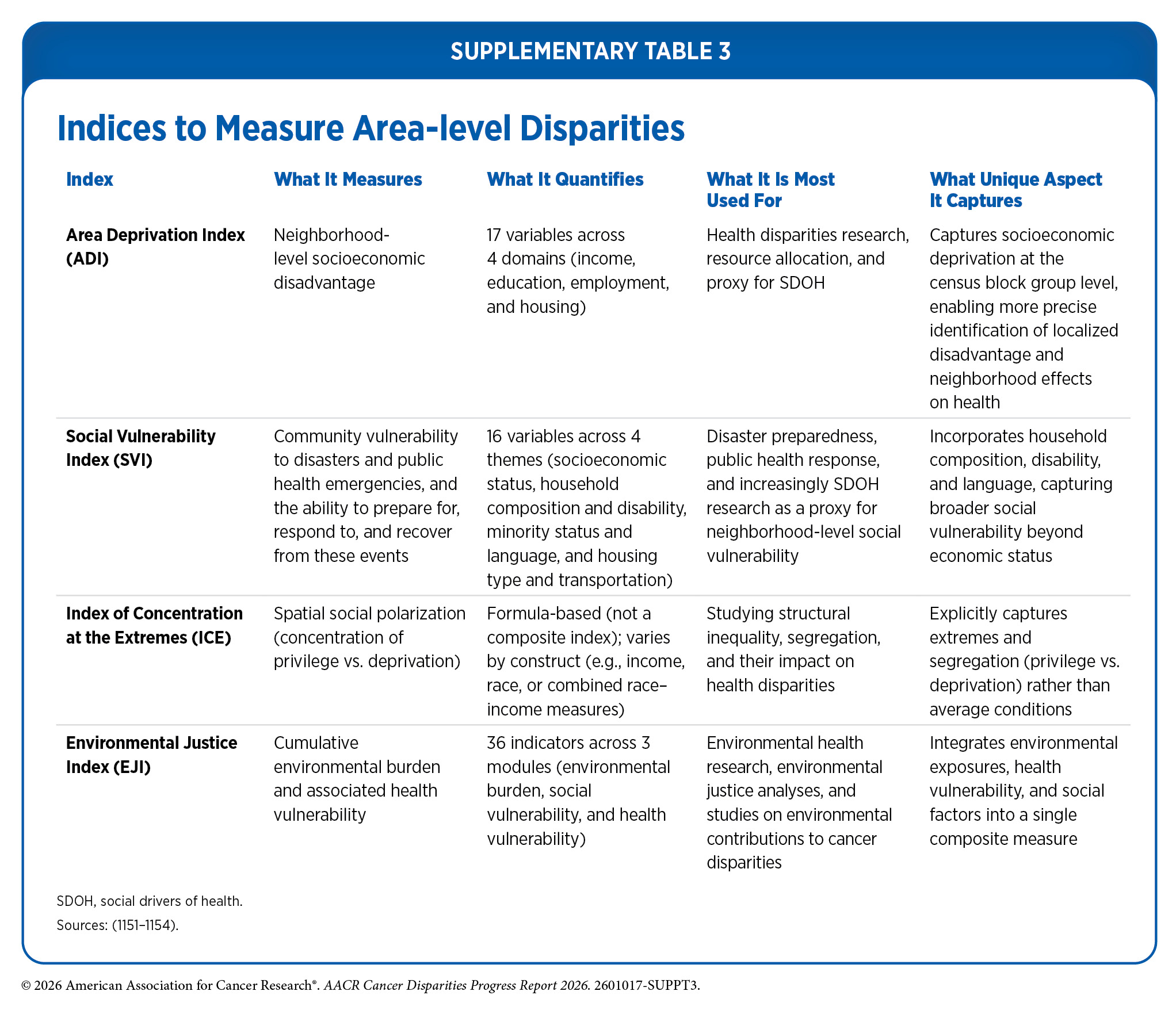
Neighborhood conditions are shaped by both social and physical contexts. The social environment of a neighborhood includes factors such as racial and ethnic composition, neighborhood‑level socioeconomic status (SES), patterns of residential distribution and segregation, and other shared demographic factors including age, religion, sexual orientation, and gender identity. Complementing these features, the built or physical environment encompasses transportation infrastructure, public services, and the policies and regulations that influence land use and development. Together, social and built environments shape key neighborhood characteristics, including cultural norms, collective efficacy, access to education and employment opportunities, availability of culturally and linguistically appropriate resources, exposure to crime and safety conditions, and residents’ access to health‑promoting resources such as nutritious food, medical facilities, clean air and water, and environments free from toxic exposures. Researchers use several methods to quantify and examine social and built environments for understanding and addressing disparities (see Supplementary Table 3).
Racial and ethnic minority groups in the United States are disproportionately more likely to reside in neighborhoods characterized by disadvantaged social and built environments. Patterns of residential segregation that underlie these disparities are not incidental; rather, they are the product of long‑standing discriminatory policies and practices rooted in structural racism. Among these, redlining represents one of the most consequential and enduring drivers of residential segregation nationwide.
Redlining—an institutionalized practice in which financial institutions systematically denied or restricted mortgage lending and other financial services in neighborhoods deemed “hazardous” for investment, often on the basis of race or ethnicity—played a central role in shaping where people could live and accumulate wealth (116)Mitchell B, et al. (2018). Although redlining has been illegal for decades, its effects persist, and evidence indicates that de facto redlining and racial bias in mortgage lending continue to influence housing patterns today. As a result, many low‑income households, disproportionately from racially and ethnically minoritized populations, remain concentrated in neighborhoods with fewer resources and poorer social and physical conditions.
Contemporary neighborhoods that were historically redlined continue to experience adverse conditions, including higher levels of air pollution and other environmental hazards (117)Bauer SJ, et al. (2025) Public Health, 238: 181. . A growing body of research has linked historical redlining to a range of adverse health outcomes, including increased chronic disease risk and a disproportionate burden of cancer (118)Kraus NT, et al. (2024) Public Health Nurs, 41: 287. (119)Karvonen KA, et al. (2025) Cancer, 131: e35677. (120)Lima SM, et al. (2025) Cancer Causes Control, 36: 483. (121)Lawrence WR, et al. (2025) Cancer, 131: e35850. (122)Roland HB, et al. (2024) Cancer, 130: 4012. . A recent study examining overall 5‑year survival among young adults found that those residing in historically redlined neighborhoods had significantly lower survival (85.1 percent) compared to young adults diagnosed in non‑redlined neighborhoods (90.3 percent) (119)Karvonen KA, et al. (2025) Cancer, 131: e35677. .
Similarly, women residing in historically redlined neighborhoods were 60 percent more likely to die from breast cancer than women living in non‑redlined areas (123)Miller-Kleinhenz JM, et al. (2024) JAMA Netw Open, 7: e2356879. . These findings highlight how past housing policies have exerted lasting effects on neighborhood environments and health, reinforcing inequities across generations. Today, the consequences of redlining extend beyond chronic environmental exposures, as climate driven disasters increasingly threaten the stability and health of these same communities.
Climate change (see Environmental Exposures) is compounding the health toll of structural racism in ways that directly shape cancer risk and outcomes. As one example, in Altadena, California, Black families reversed decades of redlining into a rare pocket of generational wealth and stable homeownership—a key social driver of cancer prevention, screening adherence, and survivorship. The January 2025 Eaton Fire, which was made more likely and intense due to global warming, burned through those same redlined tracts, placing a greater proportion of Black households inside the fire perimeter, and damaging or destroying nearly half of Black‑owned homes. In 2026, insurance gaps and corporate land acquisition are displacing this community in real time, disrupting care continuity, weakening community networks, and undermining residential stability, all of which may impact long‑term health outcomes (124)Inclusive Action. Confronting Disaster. Curbing Corporate Speculation in Post-fire Altadena. Accessed: March 31, 2026. (125)Strategic Actions for a Just Environment. Compounding Disaster. A Spatial Analysis of Housing Risk and Speculation in Post-fire Altadena. Accessed: March 31, 2026. (126)UCLA Center for Neighborhood Knowledge. LA Wildfires: Impacts on Altadena’s Black Community. Accessed: March 31, 2026. .
A recent study of residential segregation and lung cancer risk in a cohort of Black and White adults residing in the Southern United States found that reduced residential segregation was associated with fewer lung cancer cases among Black individuals (128)Xiao Y, et al. (2025) JAMA Network Open, 8: e2518481. . Indicators of health behaviors, environmental exposures, and socioeconomic context—including menthol cigarette use, exposure to fine particulate matter (PM₂.₅), secondhand smoke exposure within the home, and educational attainment—collectively accounted for about 47 percent of the association with lung cancer risk for Black individuals (128)Xiao Y, et al. (2025) JAMA Network Open, 8: e2518481. . These findings highlight how segregated neighborhood environments shape conditions, such as differential exposure to air pollution, housing quality, access to educational opportunities, as well as industry practices like targeted tobacco marketing. Additional research is needed to fully understand factors that contribute to elevated lung cancer risk among Black individuals living in residentially segregated areas.
Findings from a nationally representative, population‑based study demonstrated significant differences in cervical, breast, and colorectal cancer (CRC) screening based on neighborhood socioeconomic characteristics. Individuals residing in areas with higher social–environmental ranking (SER), a metric that reflects greater social vulnerability and environmental hazard burden, consistently exhibited lower screening rates compared to those living in areas with low‑ or moderate‑SER (129)Zindani S, et al. (2025) J Surg Oncol, 131: 1110. . Cervical cancer screening was 17 percent lower in moderate‑SER areas and 32 percent lower in high‑SER areas relative to low‑SER areas. Similarly, breast cancer screening was 16 percent lower in moderate‑SER areas and 36 percent lower in high‑SER areas, while CRC screening was 11 percent lower and 20 percent lower in moderate‑ and high‑SER areas, respectively (129)Zindani S, et al. (2025) J Surg Oncol, 131: 1110. . Collectively, these findings underscore the role of neighborhood‑level social and environmental conditions in shaping access to and uptake of cancer screening services and potentially cancer outcomes.
Socioeconomic Status (SES)
Individual‑ and area‑level SES are commonly used constructs that are important contributors to cancer disparities. Assessing SES provides insight into the social and economic conditions of a population and helps identify patterns of inequality across groups. In addition to individual‑level measures, SES can also be defined at the neighborhood‑ or area‑level, capturing the aggregate socioeconomic characteristics of residents and features of the surrounding social environment. SES is often categorized as low, medium, or high, reflecting an individual’s social and economic position within society. SES is typically measured using indicators such as educational attainment, income, and occupation. SES is a central driver of health disparities across the life course, including disparities in cancer incidence, treatment, and outcomes, and affects individuals across racial, ethnic, age, and geographic groups. For example, a recent study found that children diagnosed with Wilms tumor or neuroblastoma who resided in areas characterized by low SES or higher levels of neighborhood disadvantage were more likely to experience poorer outcomes, even after controlling for race, age, and other clinical factors (130)Nofi CP, et al. (2025) Journal of Pediatric Surgery, 60. .
Neighborhood‑level SES reflects not only the socioeconomic composition of a community but also access to resources and opportunities, including availability of goods and services; transportation infrastructure; exposure to crime, safety conditions, and policing practices; and prevailing social norms. Residents of low‑SES neighborhoods may face limited transportation options, greater distances to retail outlets and high‑quality health care facilities, and fewer supermarkets or other vendors offering affordable, healthy food. These constraints can contribute to food insecurity—defined as inadequate access to sufficient, safe, and nutritious food—and, in turn, adversely affect health outcomes and contribute to disparities.
Racial and ethnic minority groups and other medically underserved populations disproportionately experience persistently low SES as a result of historical and ongoing structural inequities. Compared to the White population, a higher proportion of nearly all racial and ethnic minority groups in the United States lived below the federal poverty level in 2024, experienced food insecurity, lacked health insurance coverage, and had lower levels of educational attainment (131)Kwon C, et al. (2026) JAMA Health Forum, 7: e256935. (132)Centers for Disease Control and Prevention. Health Insurance Coverage: Early Release of Estimates From the National Health Interview Survey, January–June 2025. Accessed: March 31, 2026. .
Consistent with these patterns, individuals and communities with lower SES experience a disproportionate burden across the cancer continuum, including differences in risk, stage at diagnosis, treatment, and survival, with education emerging as a central driver of these disparities (17)Islami F, et al. (2026) CA Cancer J Clin, 76: e70045. . A large‑scale review found that residents of low‑SES areas had a 37 percent higher risk of developing CRC compared to those living in high‑SES areas. In addition, overall mortality and CRC‑specific mortality were 24 percent and 26 percent higher, respectively, among individuals with lower SES than among those with higher SES (134)Lawler TP, et al. (2025) Social Science & Medicine, 381: 118212. . Lower SES was also associated with a 24 percent lower likelihood of completing recommended CRC screening, highlighting the role of SES‑related barriers in prevention and early detection (134)Lawler TP, et al. (2025) Social Science & Medicine, 381: 118212. .
Low SES contributes to an elevated cancer burden through multiple interconnected factors across the cancer continuum. Individuals with low SES frequently face barriers to timely high‑quality preventive, diagnostic, and treatment services, increasing the likelihood of delayed cancer diagnosis and suboptimal care. At the neighborhood level, low‑SES communities are more likely to experience disproportionate exposure to environmental carcinogens and other adverse conditions that increase cancer risk. Low SES also shapes broader lived experiences, including chronic stress and adverse mental health outcomes, which can further influence cancer risk, treatment adherence, and survivorship.
Together, these intersecting factors underscore the need for comprehensive, multisector strategies that address both individual‑ and neighborhood‑level conditions by expanding access to resources, opportunities, and support that promote socioeconomic stability and reduce cancer disparities.
Health Care Access
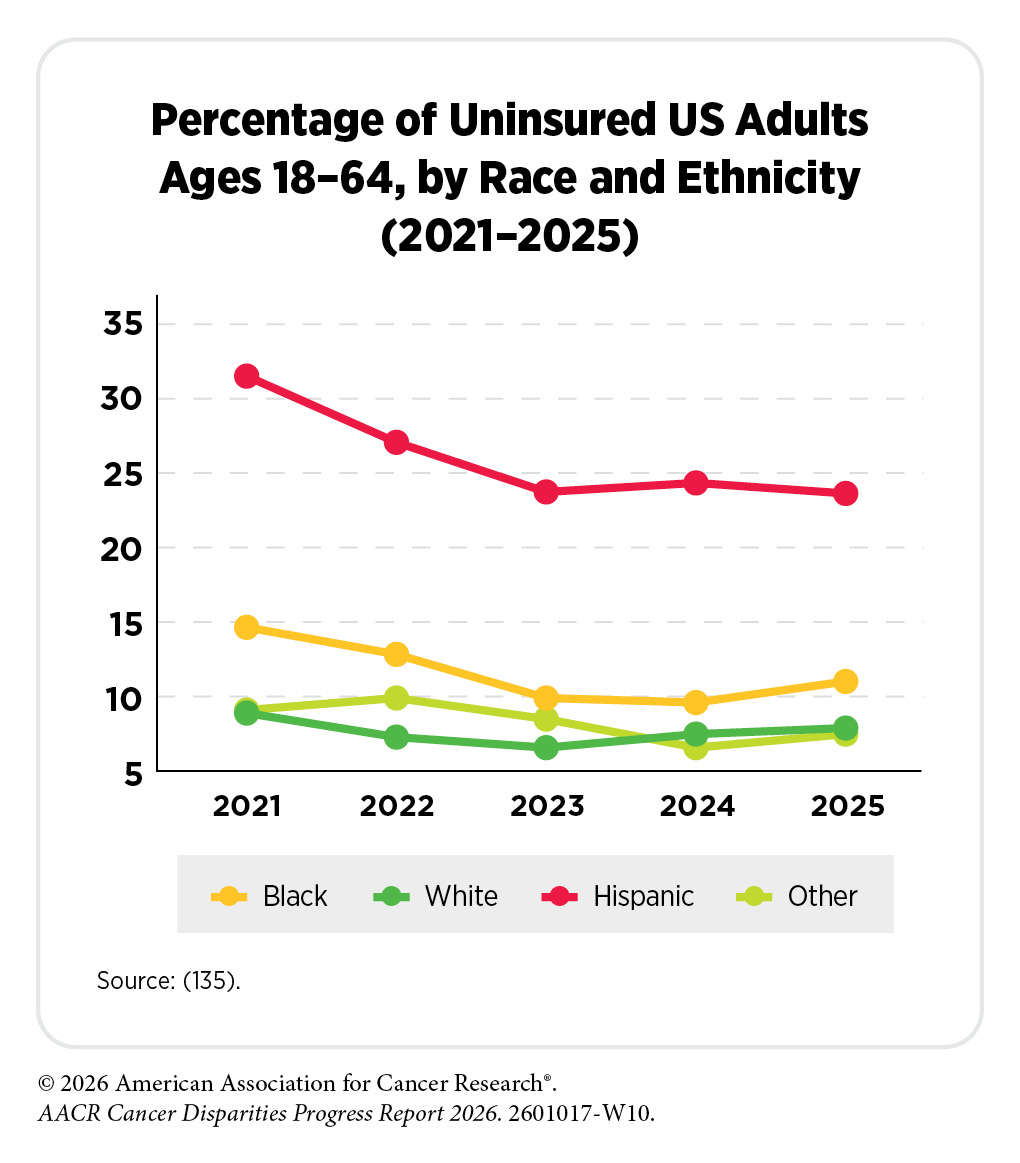
Access to timely, affordable, and high quality health care is a critical SDOH and a major driver of disparities across the cancer continuum. Health care access refers to the extent to which individuals and populations are able to obtain appropriate health services that improve health outcomes, including cancer prevention, early detection, treatment, survivorship care, and end of life care. In 2025, 11.6 percent of US adults ages 18 to 64 years were uninsured, equating to 23.6 million individuals (132)Centers for Disease Control and Prevention. Health Insurance Coverage: Early Release of Estimates From the National Health Interview Survey, January–June 2025. Accessed: March 31, 2026. .
Disparities in access to and receipt of high‑quality health care remain substantial in the United States and disproportionately affect racial and ethnic minority groups and other medically underserved populations (see Disparities in Clinical Research and Cancer Treatment). A considerable proportion of individuals in these populations are either uninsured or underinsured and receive lower quality care. Evidence suggests that policy interventions can improve access but may not fully eliminate disparities.
As one example, a study of more than 2,000 sexual and gender minority (SGM) adults found that in 2013, prior to implementation of the Patient Protection and Affordable Care Act (ACA), nearly 20 percent of participants reported being uninsured. By 2017–2018, the uninsured rate declined to 13.2 percent, but disparities remained (136)Xie Z, et al. (2025) LGBT Health, 12: 77. . SGM individuals who belonged to racial and ethnic minority groups reported higher uninsured rates compared to their White counterparts. Specifically, SGM individuals from Black and Hispanic populations were 53 percent and 52 percent more likely, respectively, to be uninsured compared to those who were White. Additionally, SGM individuals living below the federal poverty level were two to three times more likely to be uninsured than those with incomes at or above 400 percent of the federal poverty level (136)Xie Z, et al. (2025) LGBT Health, 12: 77. .
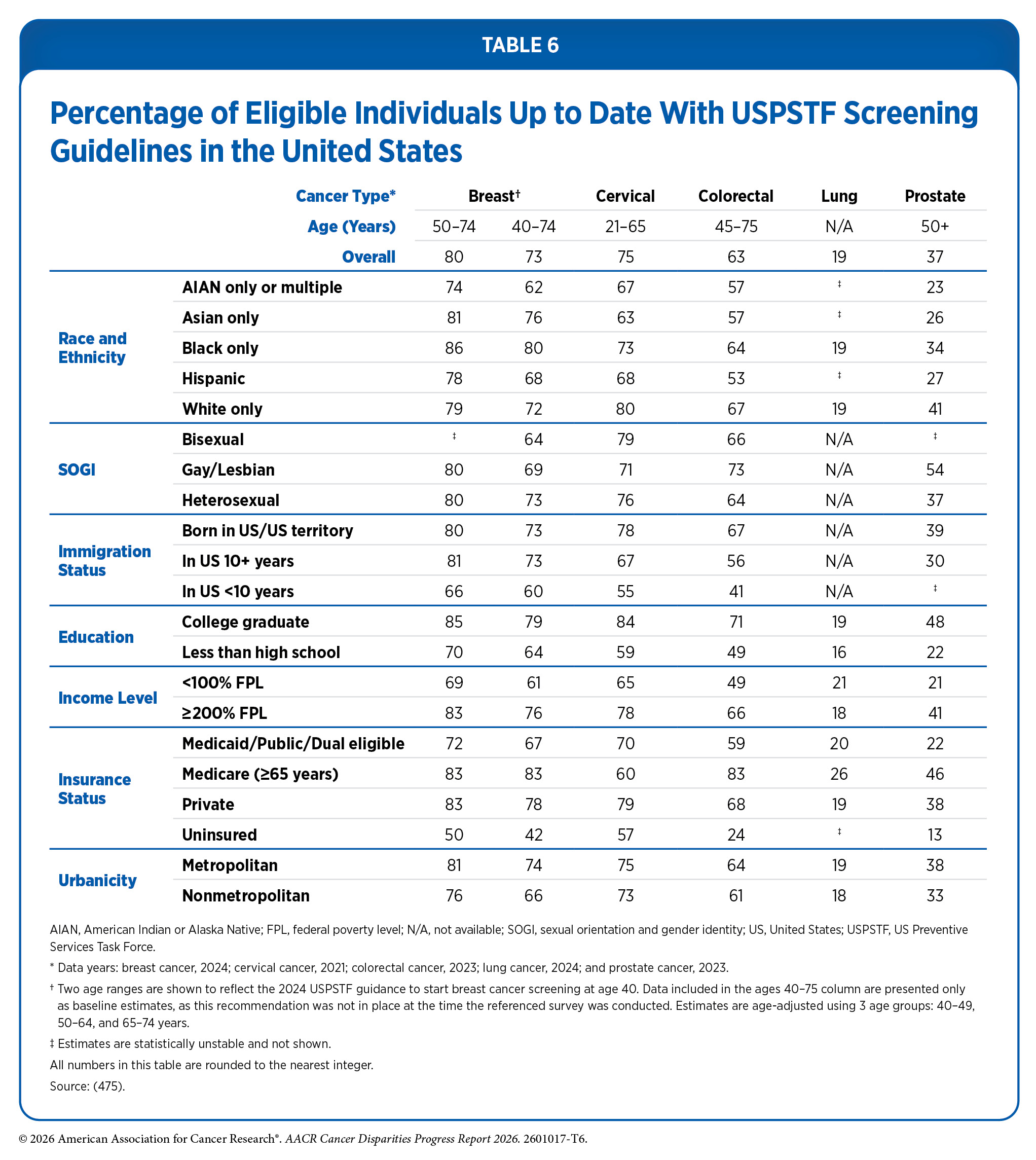
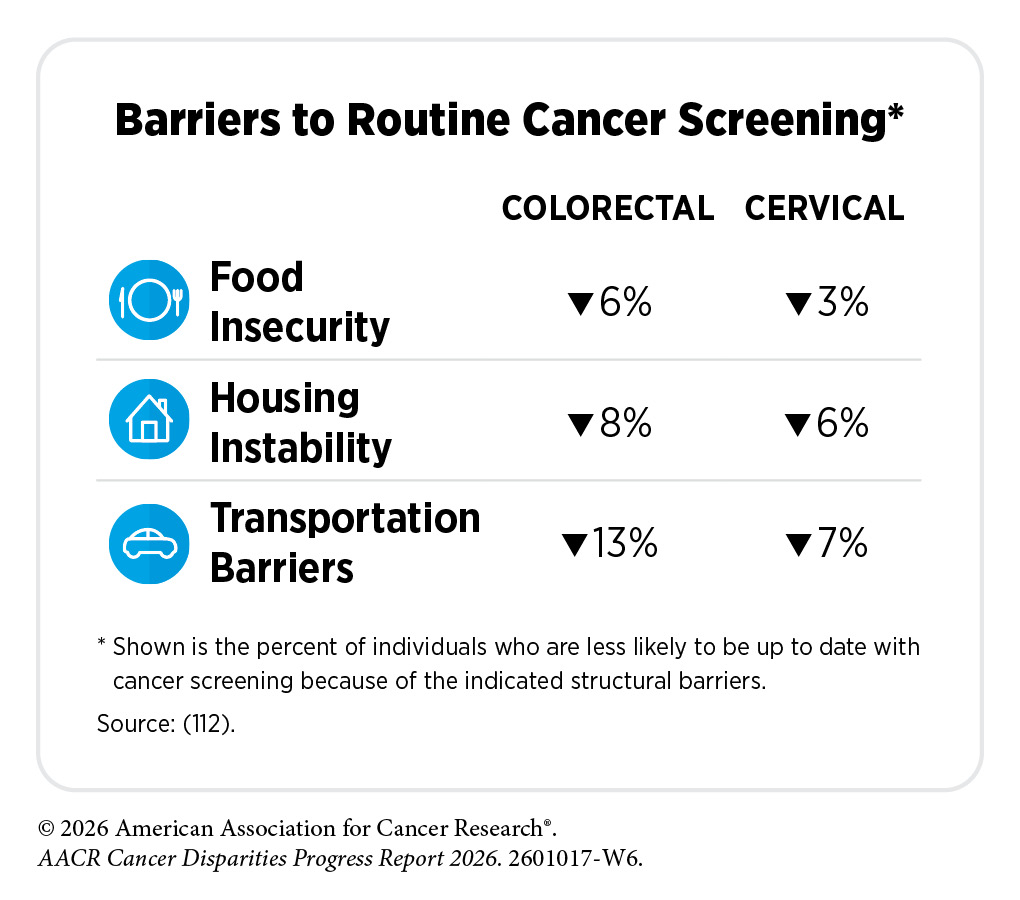
Lack of access to and receipt of quality health care has adverse effects across the cancer care continuum. Compared to those with private insurance, uninsured individuals are less likely to be up to date with the recommended cancer screening and are more likely to be diagnosed with cancer at an advanced stage. For example, one study examined receipt of cancer screening among nearly 84,000 women who were seen at 186 community‑based health care organizations, and many of whom were uninsured or publicly insured. Within this cohort, screening prevalence was below national averages for all three cancer sites (see Table 6). Most women were up to date with breast and cervical cancer screening (72.6 percent and 62.2 percent, respectively), whereas CRC screening uptake was substantially lower, with only 44 percent of women being up to date (112)Banegas MP, et al. (2024) JNCI Cancer Spectrum, 8. . Overall, screening prevalence in this cohort was below national averages for all three modalities (see Table 6). Further, researchers found that women were 3 percent to 6 percent less likely to be up to date with breast cancer screening if they experienced food insecurity, housing instability, or transportation barriers (112)Banegas MP, et al. (2024) JNCI Cancer Spectrum, 8. . These findings highlight the intersectional nature of SDOH, whereby co‑occurring economic, social, and access barriers amplify disparities in cancer preventive care and downstream outcomes.
Importantly, even when insurance coverage is available, access to care may still be limited by geographic factors, including the availability of nearby health care facilities and the time and distance required to reach them, further exacerbating disparities in cancer prevention and care. A recent review found that individuals traveling longer distances for radiation therapy were more likely to be non‑adherent to treatment and, in some cases, had poorer outcomes compared to those traveling shorter distances; however, findings were mixed across studies evaluated in the review, highlighting the complex relationship between travel burden and cancer outcomes (137)Silverwood SM, et al. (2024) Adv Radiat Oncol, 9: 101652. .
Although significant disparities in access to health care persist, recent policy changes have contributed to improved insurance coverage for some populations. Notably, the proportion of individuals in the United States living in same‑sex relationships who have health insurance has increased over the past two decades, in part reflecting policy milestones such as the ACA and the legalization of same‑sex marriage. A recent study using data from 2008 to 2022 found that individuals in same‑sex married couples achieved insurance coverage rates comparable to that of different‑sex married couples (138)Harrell BJ, et al. (2025) JAMA Network Open, 8: e2532844. . However, these gains were largely concentrated among same‑sex couples with higher incomes and in US regions that expanded Medicaid coverage (138)Harrell BJ, et al. (2025) JAMA Network Open, 8: e2532844. . These findings highlight the role of inclusive policies in expanding access to health care, while underscoring the continued importance of addressing persistent disparities across populations.
Chronic Stress
Chronic stress represents a critical pathway through which structural and social inequities influence health, including cancer risk and outcomes. Rather than reflecting temporary psychological distress, chronic stress refers to the prolonged activation of physiological stress responses resulting from persistent exposure to adverse social, economic, and environmental conditions. These exposures often include systemic stressors such as discrimination, racism, economic insecurity, neighborhood deprivation, and other forms of structural marginalization. Conceptual frameworks such as the minority stress model help researchers understand how ongoing sources of stress—such as racism, homophobia, or transphobia—can affect the body at a biological level over time by repeatedly activating stress and inflammatory responses (139)Frost DM, et al. (2023) Curr Opin Psychol, 51: 101579. .
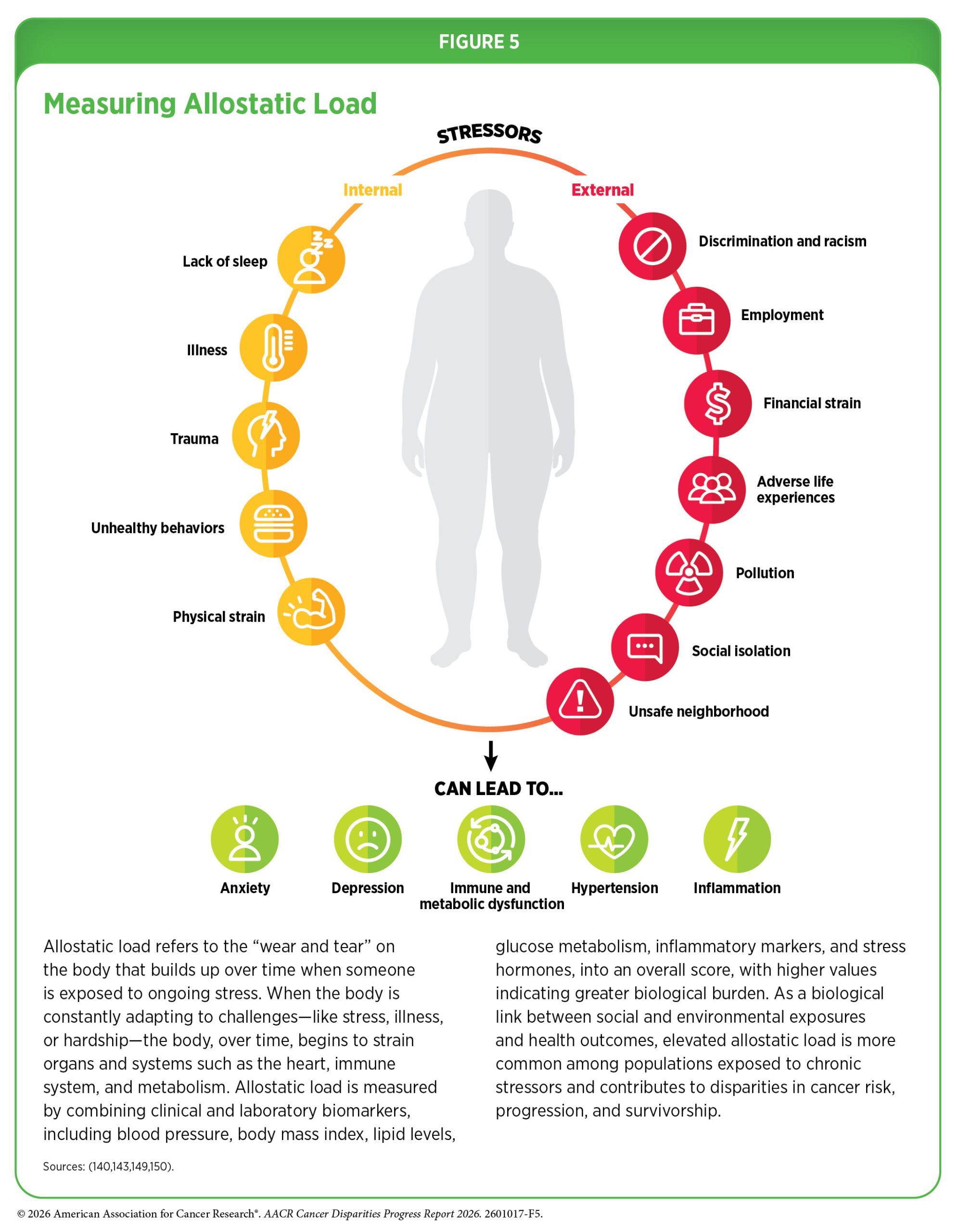
Research has shown that repeated stress over time leads to a pathophysiologic manifestation referred to as allostatic load, which represents the cumulative “wear and tear” on multiple biological systems, including neuroendocrine, immune, metabolic, and cardiovascular pathways (see Figure 5) (140)McEwen BS, et al. (1993) Arch Intern Med, 153: 2093. . Elevated allostatic load has been associated with dysregulated immune function and inflammation, which are key mechanisms linking chronic stress to adverse health outcomes such as asthma, diabetes, heart conditions, and cancer (140)McEwen BS, et al. (1993) Arch Intern Med, 153: 2093. (141)Llanos AAM, et al. (2022) Front Oncol, 12: 857548. (142)Guan Y, et al. (2025) JAMA Network Open, 8: e2528019. (143)Xing CY, et al. (2020) Breast Cancer Res Treat, 184: 901. (144)Gormley M, et al. (2025) npj Breast Cancer, 11: 90. (145)Barrett M, et al. (2022) Trends in Molecular Medicine, 28: 1040. (146)Harris AR, et al. (2025) JAMA Netw Open, 8: e2459754. .
SDOH, including features of the built environment, are central contributors to chronic stress and allostatic load. Racial and ethnic minority populations and other medically underserved groups are disproportionately exposed to stressors such as economic insecurity, neighborhood disinvestment, residential segregation, environmental hazards, housing instability, food insecurity, over‑policing, and limited access to health‑promoting resources. These conditions are shaped by historical and contemporary social injustices, and create environments in which stressors are frequent, chronic, and cumulative across the life course. Built environment characteristics—such as exposure to ambient noise, air pollution, overcrowding, unsafe housing, neighborhood violence, lack of green space, and proximity to industrial or high‑traffic areas—further amplify physiologic stress responses and contribute to elevated allostatic load.
Disparities in allostatic load have been documented across population groups. Black adults have higher allostatic load scores than White adults, with observed differences among both men (2.5 vs. 2.1, respectively) and women (2.6 vs. 1.9, respectively) (147)Duru OK, et al. (2012) J Natl Med Assoc, 104: 89. . Research has shown that allostatic load is also associated with SES. As one example, individuals with higher levels of educational attainment exhibit allostatic load scores approximately 15 percent to 30 percent lower than those with a high school diploma or less (148)Richardson LJ, et al. (2021) SSM – Population Health, 15: 100771. .
A growing body of research links chronic stress and elevated allostatic load to cancer risk and outcomes. Chronic stress has been associated with biological processes relevant to cancer initiation and progression, including immune dysregulation, chronic inflammation, and altered hormonal signaling. Epidemiologic studies increasingly report associations between psychological stress and risk of several common cancers, including breast, prostate, lung, and colorectal cancers, and hematologic malignancies (141)Llanos AAM, et al. (2022) Front Oncol, 12: 857548. (143)Xing CY, et al. (2020) Breast Cancer Res Treat, 184: 901. (151)Obeng-Gyasi S, et al. (2021) npj Breast Cancer, 7: 100. (152)Stabellini N, et al. (2023) JNCI Cancer Spectrum, 7: pkad005. (153)Shen J, et al. (2025) Sci Rep, 15: 37505. (154)Guan Y, et al. (2024) Cancers (Basel), 16. . For example, anxiety and stress‑related disorders have been linked to increased lung cancer risk, and preexisting stress‑related diagnoses have been associated with higher overall cancer mortality, particularly among individuals diagnosed with advanced‑stage disease or hematologic cancers.
Chronic stress also interacts with other SDOH by shaping coping behaviors and health care engagement. Individuals experiencing sustained stress may be more likely to engage in cancer risk–related behaviors, such as tobacco or alcohol use, as well as poor diet, all of which are patterned by neighborhood environments and targeted marketing practices (see Disparities in the Burden of Modifiable Behavioral Cancer Risk Factors). In addition, cancer diagnosis, treatment, and survivorship can introduce new and persistent stressors that further increase allostatic load, with downstream consequences for physical health, mental well‑being, and quality of life for both patients and caregivers. Recent data suggest that social risk factors, such as financial strain, social isolation, negative life events, and perceived stress, may exacerbate stress reactivity among Black individuals with cancer (155)Sanogo F, et al. (2026) Cancer Res Commun, 6: 698. .
Together, these findings highlight the importance of studying chronic stress and allostatic load within the broader context of social and built environments. Addressing cancer disparities, therefore, requires approaches that extend beyond individual‑level interventions to reduce exposure to chronic stressors embedded in neighborhoods and social systems, and to mitigate their biological consequences across the cancer continuum.
Modifiable Risk Factors
Modifiable cancer risk factors—including tobacco use, unhealthy diet, alcohol consumption, and insufficient physical activity—are commonly framed as individual health behaviors, yet they are strongly shaped by social injustices and structural conditions that influence lifestyle. Long‑standing inequities rooted in racism, economic disinvestment, and discriminatory policies have created environments in which racial and ethnic minority populations and other medically underserved communities face disproportionate exposure to conditions that promote cancer‑related risk behaviors. As a result, the ability to modify these behaviors is often limited by circumstances beyond individual control.
The social and built environments play a particularly important role in shaping exposure to and engagement in modifiable risk factors. For example, neighborhoods affected by historical and contemporary disinvestment are more likely to have a high density of tobacco retailers and alcohol outlets, often coupled with limited access to affordable, healthy foods and safe spaces for physical activity (120). Targeted tobacco and alcohol marketing practices, proximity to retail outlets, and zoning and land use decisions influence initiation, intensity, and persistence of use of these substances, contributing to higher prevalence of smoking and heavy alcohol consumption in these communities (156)Yerger VB, et al. (2002) Tob Control, 11: 336. (157)Haley SJ, et al. (2023) Int J Environ Res Public Health, 20. (158)Schwartz E, et al. (2021) Health Place, 68: 102529. . Similarly, neighborhood safety concerns, inadequate infrastructure, and lack of recreational resources can restrict opportunities for physical activity, while food environments characterized by limited availability of nutritious options increase reliance on calorie dense, nutrient poor diets.
Collectively, these patterns illustrate how social injustices and features of the built environment shape exposure to modifiable cancer risk factors across the life course. Understanding modifiable behaviors within this broader context underscores why interventions focused solely on individual behavior change are insufficient and highlights the importance of addressing the upstream social and environmental conditions that shape cancer risk (see Disparities in the Burden of Modifiable Behavioral Cancer Risk Factors).
Biological Factors
Advances in cancer biology have substantially expanded understanding of the molecular mechanisms underlying cancer initiation, progression, and treatment response. Advances in cancer genomics and related technologies have revealed that alterations in gene expression, epigenetic regulation, and variations in DNA sequence can influence cancer risk and outcomes (see Understanding Cancer Development in the Context of Cancer Disparities). Importantly, a growing body of evidence demonstrates that these biological processes do not operate in isolation. Environmental exposures and social conditions, including those shaped by structural factors, can influence molecular and cellular pathways relevant to cancer development through mechanisms such as chronic inflammation, immune dysregulation, and stress‑related biological changes. In this context, the interaction between SDOH and biological factors represents a critical mechanism which contributes to disparities in cancer risk, progression, and survival.
Chronic stress and adverse environmental exposures can drive epigenetic changes, which can turn genes on or off or modify how they function without altering the underlying DNA sequence (see Influences Inside the Cell). Social and environmental stressors, such as pollution, chronic stress, or unsafe living conditions, can influence the body in ways that increase cancer risk.
For example, a recent study reported that Black women exposed to higher levels of air pollution, particularly fine particulate matter (PM₂.₅), and greater neighborhood deprivation had 2.6‑ and 1.2‑fold higher likelihood, respectively, of exhibiting crown‑like structures in breast tissue—a cellular feature with an established link to breast cancer (160)Harris AR, et al. (2025) JAMA Netw Open, 8: e2461334. . Crown‑like structures are a visible indicator of chronic inflammation, which can promote epigenetic alterations influencing gene expression and cancer risk. Together, this evidence illustrates how area deprivation and environmental disadvantage may become biologically embedded through inflammation‑driven epigenetic mechanisms, reinforcing the importance of addressing neighborhood conditions that sustain chronic stress exposure as part of comprehensive strategies to reduce cancer disparities.
Approaches to Assess Drivers of Health and Reduce Cancer Disparities
As described in the preceding sections, SDOH shape lived experiences and influence health outcomes across the life course. These drivers operate through interconnected social, economic, and environmental pathways, contributing to persistent cancer disparities that disproportionately affect racial and ethnic minority groups and other medically underserved populations. Addressing SDOH therefore represents a critical opportunity to improve population health and reduce inequities in cancer risk, access to care, and outcomes. Across the cancer continuum, stakeholders are increasingly implementing coordinated, multipronged strategies to address SDOH at the individual, community, health system, and policy levels. In the following sections, we highlight selected approaches that are advancing understanding of SDOH and contributing to efforts to mitigate cancer disparities and promote health equity.
Population‑focused Approaches
Population‑level policies and evidence‑based interventions play a critical role in addressing SDOH and can improve health outcomes while also strengthening societal and economic resilience.
Several long‑standing, nationwide initiatives prioritize SDOH as a core component of population health improvement. One such effort is the US Department of Health and Human Services’ Healthy People 2030 initiative, which emphasizes multisector strategies to improve social and built environments and reduce health inequities (161)US Department of Health and Human Services. Office of Disease Prevention and Health Promotion. Healthy People 2023. Accessed: March 17, 2024. . Addressing SDOH is embedded throughout Healthy People 2030 goals and objectives, reflecting a broad recognition of the role of social conditions in shaping health outcomes. Similarly, population-level policy interventions such as the ACA have altered key SDOH by expanding health insurance coverage, increasing access to preventive services, and strengthening community-based care systems. Substantial evidence demonstrates that ACA‑associated Medicaid expansion has been linked with increased uptake of cancer screening, earlier cancer diagnosis, greater use of evidence‑based cancer treatments, and improvements in survival across population groups (see Impact of Health Insurance and Access to Care and Overcoming Cancer Disparities Through Science‑based Public Policy) (136)Xie Z, et al. (2025) LGBT Health, 12: 77. (162)Tamirisa N, et al. (2024) Ann Surg, 280: 136. (163)Hussain MR, et al. (2025) Cancers (Basel), 17. .

In addition to broad policy reforms, evidence‑based strategies are being implemented to address specific social needs that affect cancer prevention and care. Transportation insecurity, for example, can contribute to delayed or missed preventive services and treatment, leading to adverse health and economic consequences (112)Banegas MP, et al. (2024) JNCI Cancer Spectrum, 8. (164)Graboyes EM, et al. (2022) J Natl Cancer Inst, 114: 1593. . To mitigate this barrier, the Centers for Medicare & Medicaid Services administers the Non‑Emergency Medical Transportation (NEMT) program, which provides eligible Medicaid beneficiaries with transportation to medical appointments and is the largest program addressing health care–related transportation needs nationwide. Health systems, nonprofit organizations, and private sector partners have also implemented transportation support initiatives, as was the case with Dennis P. Gruenhagen, with early evidence suggesting improvements in care adherence and reductions in missed appointments and associated health care costs (165)Pringle S, et al. (2024) Support Care Cancer, 32: 317. .
Food insecurity represents another major social challenge affecting patients with cancer, particularly those from racial and ethnic minority groups and other medically underserved communities. Several initiatives have been developed to address this need. As one example, the Food to Overcome Outcome Disparities (FOOD) program, launched by a comprehensive cancer center in New York City, integrates on‑site food pantries, nutrition education, and food navigation services within safety‑net hospitals and oncology clinics (167)Gany FM, et al. (2020) J Health Care Poor Underserved, 31: 595. . Evaluations of the program demonstrate significant improvements in food security among participating patients. More broadly, partnerships between health care systems and housing authorities have also addressed upstream social needs (168)Gany F, et al. (2022) Journal of Clinical Oncology, 40: 3603. . For example, the Permanent Supportive Housing initiative, implemented by the Louisiana Department of Health in collaboration with the Louisiana Housing Authority, has demonstrated reductions in Medicaid expenditures and hospital utilization, highlighting the potential health and cost benefits of coordinated housing and health policies (169)Human Services Research Institute. Evaluation of the Louisiana Permanent Supportive Housing Initiative. Accessed: March 17, 2024. .
Continued investment in and evaluation of population‑level strategies, alongside efforts to sustain and scale effective programs, will be essential to advancing health equity and reducing the cancer burden across diverse populations.
Research‑focused Approaches
Approaches focused on understanding and addressing SDOH are central to improving population health and reducing cancer disparities over the long term. Federal agencies, including the National Institutes of Health (NIH), NCI, and the Centers for Disease Control and Prevention (CDC), along with cancer‑focused organizations, continue to support coordinated efforts to study, develop, and implement interventions that are responsive to the needs of diverse communities. Within NIH, the National Institute on Minority Health and Health Disparities (NIMHD) plays a leading role in advancing research aimed at improving minority health and reducing health disparities.
An example is the RESPOND (Research on Prostate Cancer in Men of African Ancestry: Defining the Roles of Genetics, Tumor Markers, and Social Stress) study, established through a partnership with NIMHD and NCI, which is one of the largest coordinated efforts to examine factors contributing to the disproportionate burden of aggressive prostate cancer among Black men (see Overcoming Cancer Disparities Through Science‑based Public Policy) (170)National Institutes of Health. NIH and Prostate Cancer Foundation launch large study on aggressive prostate cancer in African-American men. Accessed: March 2017, 2024. . The RESPOND study has established a national network of investigators across multiple institutions and has enrolled more than 12,000 Black men diagnosed with prostate cancer. By integrating biological data with information on social, environmental, and behavioral factors, RESPOND aims to improve understanding of the complex pathways underlying prostate cancer disparities and to inform more effective prevention, diagnosis, and treatment strategies. Similarly, the Assessing Cervical Cancer Healthcare Inequities in Diverse Populations (ACHIEVE) study examines the role of structural racism in shaping disparities in cervical cancer treatment and survival, with the goal of advancing equitable cervical cancer care for all women (171)The Achieve Study. Assessing Cervical Cancer Healthcare Inequities in Diverse Populations. Accessed: March 31, 2026. .
In addition, NIH and NCI continue to support several large-scale cohort studies designed to elucidate the root causes of cancer disparities. These include the Multiethnic Cohort Study, which follows over 215,000 residents of Hawai‘i and Los Angeles across diverse racial and ethnic groups to examine cancer and other chronic diseases (172)University of Hawai‘i Cancer Center. The Multiethnic Cohort Study. Accessed: March 26, 2024. ; the Southern Community Cohort Study, an NCI‑funded prospective cohort of approximately 85,000 adults, two thirds of whom are Black, designed to investigate social, environmental, and biological contributors to cancer disparities in the southeastern United States (173)Signorello LB, et al. (2010) J Health Care Poor Underserved, 21: 26. ; the ASian American ProspectIve REsearch (ASPIRE) cohort study, which represents all Asian ethnic groups across the United States and aims to better understand the causes of cancer in diverse Asian American communities (174)Science Insider. First long-term cancer study in Asian Americans set to launch this year. Accessed: March 31, 2026. ; and the Black Women’s Health Study, which examines determinants of chronic diseases, including breast cancer, among Black women (175)Rosenberg L, et al. (1995) J Am Med Womens Assoc (1972), 50: 56.

One of NIH’s largest and most comprehensive initiatives addressing health disparities is the All of Us Research Program (All of Us), which seeks to enroll one million or more participants to create a diverse and representative research cohort reflecting the demographic, socioeconomic, and geographic diversity of the United States. The program collects a broad range of data—including genomic information, electronic health records, lifestyle factors, and environmental exposures—to support research on disease prevention, treatment, and health equity (91)All of Us Research Program I, et al. (2019) N Engl J Med, 381: 668. . As of March 2026, All of Us enrolled more than 881,000 participants, with nearly 66,000 individuals with a history of cancer, over 80 percent of whom are underrepresented in biomedical research and approximately 45 percent from racial and ethnic minority groups (176)All of Us Research Program. All of Us Genomic Quality Report. Accessed: March 31, 2026. (177)All of Us Research Hub. All of Us Public Data Browser. Accessed: March 31, 2026. .
Together, these initiatives provide models for advancing cancer disparities research and for integrating social, environmental, and biological data to inform equitable cancer control strategies.
Despite the scope and scale of these large, long‑standing research efforts, cancer‑related health disparities persist in the United States, emphasizing the need for continued and expanded investigation. In response, VOICES of Black Women, a large prospective cohort study designed to further advance understanding of factors contributing to disparities in cancer risk and outcomes among Black women, was launched (178)McCullough LE, et al. (2025) Cancer, 131: e35775. . VOICES of Black Women builds on prior large‑scale studies by examining well‑established cancer risk factors while also integrating emerging areas of research, including neighborhood and built environments, social support, use of personal care products, experiences of racism and discrimination, and intergenerational wealth. By capturing a broader range of social, environmental, and structural influences, this initiative reflects an evolving approach to cancer disparities research that seeks to more fully characterize the contexts in which risk develops and persists.
Community‑focused Approaches
In recent years, there has been growing recognition that effectively addressing SDOH requires sustained, community-based approaches grounded in the lived experiences of affected populations. Community engaged initiatives play a critical role in translating research into practice by fostering trust, strengthening local capacity, and ensuring that interventions are culturally relevant and responsive to community priorities. In the past 2 years, a number of new and expanded efforts have emphasized bidirectional partnerships between academic institutions, health systems, community organizations, and residents to address cancer disparities through integrated strategies that span research, education, outreach, and policy implementation. These initiatives reflect a shift toward place based, participatory models that explicitly address structural inequities and social and environmental contexts influencing cancer risk and outcomes. In this section, we highlight selected community-based initiatives that exemplify these approaches and illustrate their potential to advance cancer health equity.
Researchers are increasingly employing innovative, community engaged approaches to bridge the gap between scientific discovery and the lived experiences of populations disproportionately affected by cancer. The Florida–California Cancer Research, Education and Engagement (CaRE²) Health Center represents one such approach, exemplifying a scalable model of bidirectional engagement between researchers and community members (179)Hensel B, et al. (2023) J Cancer Educ, 38: 1429. . Through its innovative Community Scientist Research Ambassador model, the program integrates research, education, and outreach to strengthen community understanding of cancer risk, prevention, and participation in medical research. Delivered through a structured 13‑week virtual curriculum and offered in both English and Spanish, the program provides community members with targeted education on key aspects of cancer research and information about cancers with high morbidity and mortality in these populations, including prostate, lung, and pancreatic cancers. Graduates of the program are equipped to participate in cancer research teams providing important community perspectives that can inform research, serving as bridges between the community and the scientific enterprise.
Evaluation of the program shows that understanding of breast and prostate cancers improved following completion of the CaRE² course, highlighting the effectiveness of culturally and linguistically tailored, community‑centered education (179)Hensel B, et al. (2023) J Cancer Educ, 38: 1429. . By embedding education within trusted community partnerships and emphasizing mutual learning, the CaRE² Health Center demonstrates how community‑based initiatives can enhance research relevance, build capacity, and promote more inclusive participation in cancer research.
In addition to academic institution‑led community engagement efforts, federal agencies have launched community‑based research initiatives to better understand and address the multilevel drivers of cancer disparities. The CDC, for example, has supported a set of research initiatives focused on identifying effective strategies to reduce preventable cancers, promote timely and appropriate cancer screening, and improve survivorship outcomes among populations experiencing disproportionate cancer burdens.
One such initiative is Project Black People Against Tobacco (BAT), a community driven effort in Jackson, Mississippi, aimed at reducing tobacco use among Black communities. Project BAT employs multiple strategies, including referrals to smoking cessation services, development of culturally relevant educational resources, community engagement to increase awareness of the harms of tobacco use, and education on policy approaches to reduce smoking in public places, which has been effective in other communities. The project also emphasizes engagement with local decision-makers to support tobacco control policies that reduce exposure and promote cessation (181)Centers for Disease Control and Prevention. Reducing Cancer Disparities Through Partnerships. Accessed: March 31, 2026. .
Another CDC supported initiative, New York City Cancer Outreach Network in Neighborhoods for Equity and Community Translation (NYC CONNECT), aims to improve access to cancer screening through community clinical partnerships in New York City. This initiative is grounded in efforts to address systemic racism across multiple contexts, including neighborhood environments, food access, and health care systems, that shape cancer screening behaviors among marginalized populations, including Black, Asian, and Hispanic communities. As part of its approach, NYC CONNECT examines how reducing structural barriers and fostering community partnerships can increase timely uptake of cancer screening.
CDC’s Racial and Ethnic Approaches to Community Health (REACH) program has similarly supported community‑based policy, systems, and environmental approaches to cancer and other non‑communicable disease prevention in low‑resource and geographically isolated communities. In Hawai‘i, REACH funding supported the Advancing and Sustaining Pacific Interventions to Reach Equity initiative, which promoted healthy nutrition standards, expanded access to fresh produce, and reduced tobacco use across the US‑affiliated Pacific Island, including Guam, the Republic of the Marshall Islands, Republic of Palau, and the Federated States of Micronesia (182)Centers for Disease Control and Prevention. REACH 2023 Program Recipients. Accessed: March 31, 2026. . This infrastructure has also extended cervical cancer screening to populations with historically low or no prior screening coverage (183)Palafox NA, et al. (2024) Cancer Control (Woodbridge), 2024: 59(184)Qin J, et al. (2024) J Womens Health (Larchmt), 33: 839. .
Complementing these CDC led efforts, NCI has established the Advancing Cancer Control Engaged Research through Transformative Solutions (ACCERT) initiative. ACCERT is a consortium of four research centers focused on developing and testing interventions that address the impact of SDOH on adverse cancer prevention and control outcomes. The initiative emphasizes the importance of developing new measures and methods to assess community‑level SDOH, integration of community engagement into cancer control research, and capacity building among investigators and community partners. By focusing on lived experience and place based context, ACCERT seeks to accelerate the translation of equity focused research into sustainable, community responsive cancer control strategies (185)Division of Cancer Control and Population Sciences. Advancing Cancer Control Engaged Research through Transformative Solutions (ACCERT). Accessed: March 31, 2026. .
Collectively, these initiatives underscore that meaningful progress in addressing SDOH and reducing cancer disparities depends on sustained community engagement. By centering the voices, priorities, and lived experiences of communities most affected by inequities, community-based approaches help identify specific barriers, build trust, and co‑create solutions that are both relevant and effective. Engagement at the community level is therefore not ancillary, but foundational to addressing the structural and social conditions that shape cancer risk, access to care, and outcomes. Strengthening partnerships among communities, researchers, health systems, and policymakers will remain essential to advancing strategies that reduce disparities and improve health outcomes across populations.
Next Section: Understanding Cancer Development in the Context of Cancer Disparities Previous Section: The State of US Cancer Disparities in 2026