Supporting Cancer Patients and Survivors
In this section, you will learn:
- In the United States, the number of people living with a history of cancer is expected to rise by 5.2 million in the next 11 years, reaching 22.1 million by January 1, 2030.
- Each person diagnosed with cancer faces a unique set of challenges, but one in four survivors reports a poor physical quality of life and one in 10 reports poor mental health – related quality of life.
- Palliative care, modifying behaviors, and cancer rehabilitation can improve quality of life.
- Improving implementation of palliative care, behavior modification, and cancer rehabilitation across the continuum of cancer care is essential if we are to better meet the needs of the rapidly expanding population of cancer survivors.

Research is driving advances in cancer detection, diagnosis, and treatment that are helping more and more people to survive longer and lead fuller lives after a cancer diagnosis. According to the latest estimates, more than 16.9 million U.S. adults and children with a history of cancer were alive on January 1, 2019, compared with just 3 million in 1971, and this number is projected to rise to 22.1 million by January 1, 2030 (3, 256). Meeting the needs of this rapidly expanding population will require a concerted effort from all stakeholders committed to reducing the morbidity and mortality of cancer, including advocates such as Tomma Hargraves, whose experience with lung cancer led her to train to become a patient lay navigator so that she could help others diagnosed with the disease.
While a person is considered a cancer survivor from the time of diagnosis through the remainder of his or her life, not everyone identifies with this term. Each person who is diagnosed with cancer has a unique experience. These experiences range from successful treatment and living cancer free for the remainder of life, with or without adverse effects of treatment, to living with cancer and its effects for the remainder of life.
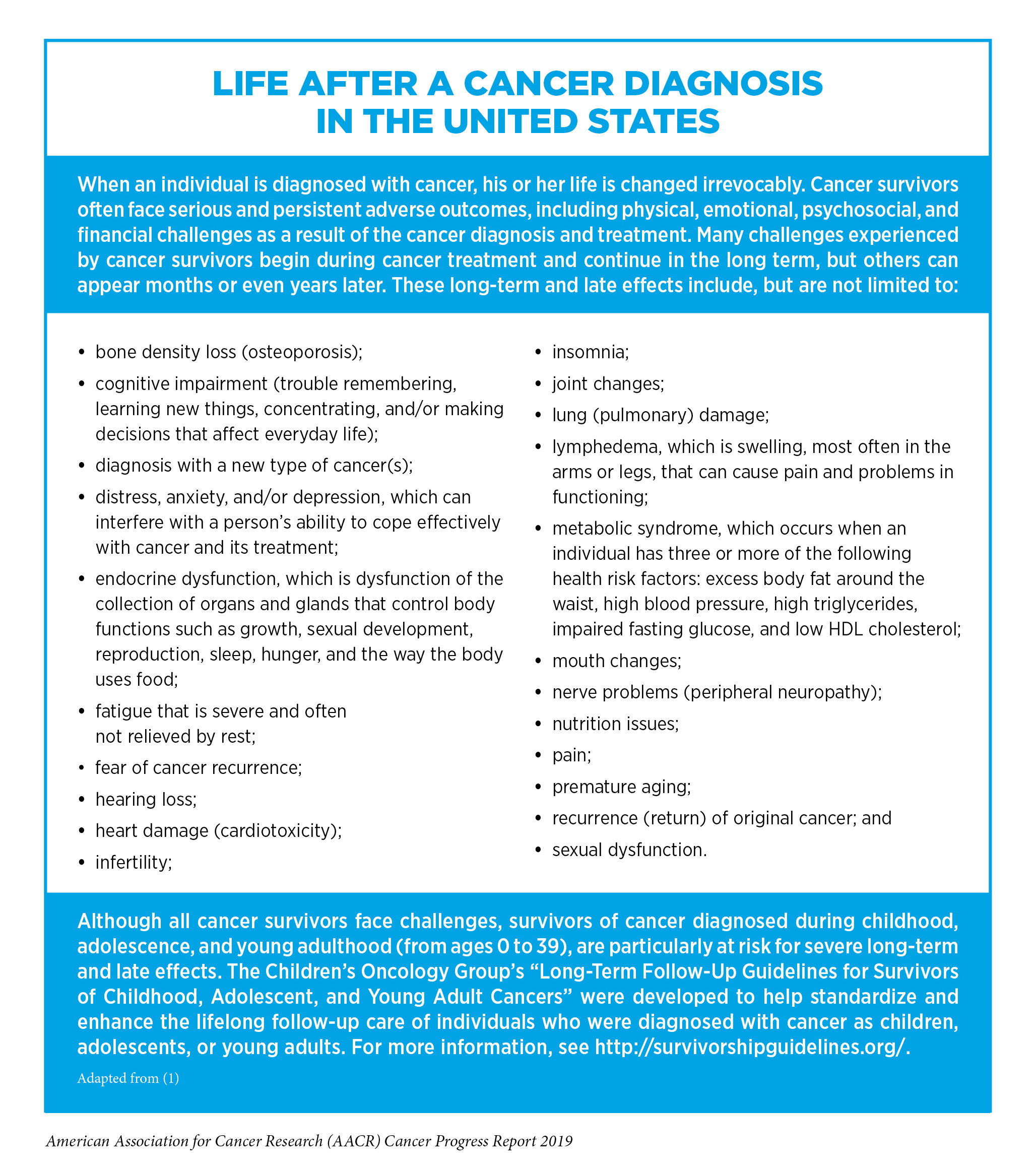
Cancer survivorship encompasses three distinct phases: the time from diagnosis to the end of initial treatment, the transition from treatment to extended survival, and long-term survival. Each phase of cancer survivorship is accompanied by a unique set of challenges (see sidebar on Life after a Cancer Diagnosis in the United States). Importantly, the issues facing each cancer survivor vary, depending on many factors, including gender, age at diagnosis, type of cancer diagnosed, general health at diagnosis, and type of treatment received.

Unfortunately, certain segments of the U.S. population shoulder a disproportionate burden of the adverse effects of cancer and cancer treatment, which can negatively affect the duration and quality of life after a cancer diagnosis (see sidebar on Disparities in Health and Quality of Life after a Cancer Diagnosis). In addition, a recent study found that these segments of the U.S. population were also at increased risk of experiencing financial hardship because of the out-of-pocket expenditures caused by a cancer diagnosis and cancer treatment (257). For example, 37 percent of cancer survivors who had no health insurance reported needing to borrow money, going into debt, declaring bankruptcy, or being unable to cover their copayments compared with 22 percent of cancer survivors who had private health insurance (257).
Financial hardship, or financial toxicity, extends beyond out-of-pocket direct medical costs and can be caused by indirect costs of lost productivity, such as days lost from work or disability days (263). Several recent studies have highlighted how this form of financial toxicity affects survivors of cancer diagnosed during adolescence or young adulthood (AYA) (ages 15 to 39) (264-265). One showed that AYA cancer survivors have annual excess productivity losses of more than $2,000, and another showed that treatment type affects physical and mental work capacity and time off from work. For example, AYA breast cancer survivors who were treated with chemotherapy were more than twice as likely to take unpaid time off from work as those who were not treated with chemotherapy (265).
Improving Quality of Life and Outcomes across the Continuum of Cancer Care
For patients and survivors with cancer, quality of life is a multidimensional concept that goes beyond the person’s cancer-related outcomes and considers their overall physical, mental, emotional, and social functioning (266). As more and more people are surviving longer after a cancer diagnosis, the issue of quality of life has become increasingly important across the continuum of cancer care (267).
In recent years, numerous changes in cancer treatment are helping to reduce the short-term, long-term, and late effects of treatment, and thereby improving quality of life for cancer patients and survivors (see Progress across the Clinical Cancer Care Continuum). For example, molecularly targeted therapeutics more precisely target a patient’s cancer cells compared with cytotoxic chemotherapeutics and therefore tend to cause fewer adverse effects, although longer follow-up of patients is needed to determine if molecularly targeted therapeutics have any long-term or late effects. In addition, health care providers and researchers are identifying ways to tailor surgery, radiotherapy, and cytotoxic chemotherapy to minimize their adverse effects without negatively affecting survival. The success of these approaches is highlighted by one recent study that found that significantly fewer survivors of cancer diagnosed in childhood are dying because of late effects of cancer treatment, such as a new cancer or heart disease, compared with three decades ago (268).
Despite advances in treatment that are helping improve quality of life, researchers have found that cancer survivors report lower general health and quality of life compared with people without a history of cancer (269-270). For example, in one study, 25 percent of cancer survivors reported a poor physical quality of life and 10 percent reported a poor mental-health related quality of life compared with 10 percent and 6 percent of people without a history of cancer, respectively (269). Therefore, identifying new ways to improve general health and quality of life throughout a patient’s experience with cancer, beginning at diagnosis and continuing through treatment, follow-up, survivorship, and end-of-life care, is an area of intensive research investigation.
Improving quality of life is also important because research suggests that quality of life is linked to cancer-related outcomes, including survival. In fact, several strategies, including outpatient specialty palliative care, integration of electronic patient-reported outcomes into routine oncology practice for symptom monitoring and management, and exercise, have been shown to improve quality of life and survival (271-274).
Palliative Care
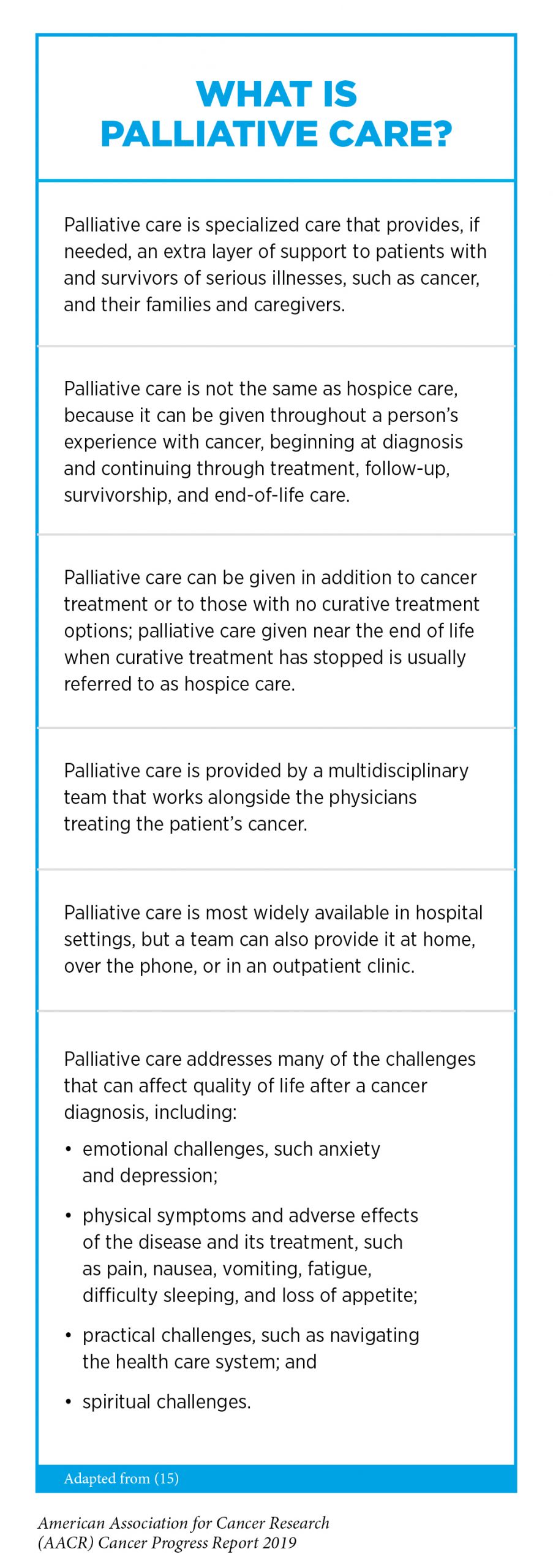
One approach that can be used across the continuum of cancer care to optimize the quality of life for patients, survivors, and their families and caregivers is palliative care (see sidebar on What Is Palliative Care?). Palliative care can be given throughout a person’s experience with cancer, beginning at diagnosis and continuing through treatment, follow-up, survivorship, and end-of-life care. The goal is not to treat the cancer but to provide those who need it with an extra layer of care that prevents or treats the symptoms and adverse effects of the disease and its treatment, as well as addresses the functional, psychological, social, and spiritual challenges that accompany a cancer diagnosis.
Health care providers and researchers are constantly looking to identify new ways to palliate the physical symptoms and other adverse effects of cancer and its treatment. One strategy used to reduce the pain caused by cancer that has spread to the bones is palliative radiotherapy. In most cases, patients receive multiple doses of radiotherapy. However, recent results from a phase II clinical trial comparing the safety and effectiveness of a single high dose of stereotactic body radiotherapy and standard multifraction radiotherapy showed that significantly more patients who received a single high dose of stereotactic body radiotherapy reported relief from bone pain after 2 weeks, 3 months, and 9 months, compared with patients who received multifraction radiotherapy (275). In addition, the rate of recurrence of the treated bone metastases at both 1 and 2 years was lower among patients who received a single high dose of stereotactic body radiotherapy, suggesting that this may provide a new approach to palliating bone pain that requires fewer hospital visits, making it more convenient and effective for patients.
Recent research shows that integrating palliative care during the early stages of cancer care can significantly improve quality of life and significantly lower hospital costs (276-278). Thus, it is imperative that we increase awareness of the important role that palliative care can play across the continuum of clinical cancer care because many patients do not receive palliative care or even know what it is (279-280).
Psycho-oncology
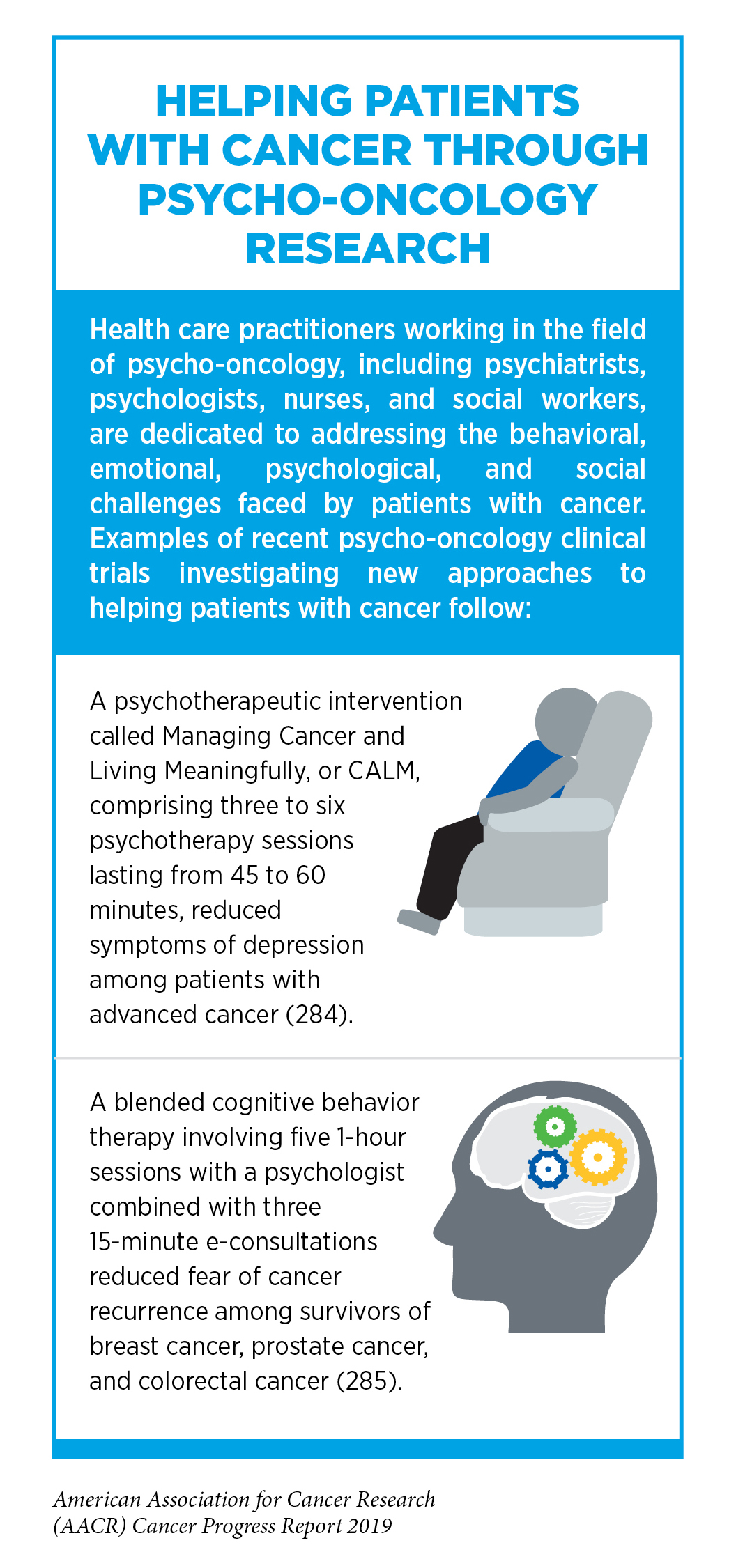
Researchers and health care providers committed to developing new approaches to addressing the behavioral, emotional, psychological, and social challenges posed by cancer work in the field of psycho-oncology (see sidebar on Helping Patients with Cancer through Psycho-oncology Research). These challenges include treatment-related cognitive impairment, fear of cancer recurrence, anxiety, depression, stress, posttraumatic stress disorder, and feelings of despair. Addressing these challenges is important not just for improving quality of life, but also for improving outcomes because challenges such as depression and anxiety are often associated with decreased adherence to cancer treatment and decreased survival (281-282).
Promoting Healthy Behaviors
Evidence is emerging that modifying behaviors to eliminate or avoid many of the lifestyle-related factors that increase a person’s risk of developing cancer and other chronic health conditions, such as cigarette smoking, inactivity, excess body weight, unhealthy diet, and alcohol consumption, can improve outcomes and quality of life for cancer patients and survivors (285-287) (see Preventing Cancer: Identifying Risk Factors).
For example, research has shown that cancer patients and survivors who smoke cigarettes are at increased risk of cancer recurrence, developing a second cancer, treatment-related toxicity, poorer response to treatment, and death from cancer (57). Fortunately, all cancer patients and survivors who are current smokers can improve their prognosis by quitting smoking. Despite this knowledge, one study found that 9 percent of cancer survivors continue to smoke (288). Therefore, more research is needed to develop optimal strategies to provide patients with cancer who smoke with the best strategies for smoking cessation (289).
Research has also shown that eating a diet rich in vegetables, fruits, and whole grains, or a diet high in fiber, following a diagnosis of nonmetastatic colon cancer can reduce mortality (290-291), and that exercising regularly or being physically active can reduce recurrence and mortality for survivors of several types of cancer, including early breast cancer, childhood cancer, colorectal cancer, and prostate cancer (292-293). In addition, exercise can improve overall quality of life for patients and survivors who are undergoing treatment for cancer and for those who have completed treatment (294-295). More specifically, exercise during and after treatment is completed has been shown to alleviate many of the adverse long-term and late effects of cancer and cancer treatments, including anxiety, depression, cognitive impairment; fatigue, lymphedema, pain, peripheral neuropathy, and poor sleep quality, and to improve heart and lung function (296-304). This burgeoning body of evidence has led experts to recommend that cancer patients and survivors achieve and maintain a healthy body weight, participate in regular physical activity, and eat a diet rich in vegetables, fruits, and whole grains (305).
Cancer Rehabilitation
General nutrition and physical activity guidelines can help cancer patients and survivors increase their chances of a better outcome and their chances of a higher quality of life. However, individuals diagnosed with cancer have their own unique needs for regaining and improving health. For many patients, these needs are not fully met by general guidelines, and this has led to an increasing recognition of the importance of cancer rehabilitation programs.
Cancer rehabilitation can improve quality of life by providing patients who need it with a tailored program of interventions to improve their daily function and quality of life (306). Cancer rehabilitation involves a multimodal, transdisciplinary team of health care professionals, which can include physiatrists, physical therapists, occupational therapists, speech-language pathologists, and rehabilitation nurses. After the team has identified an individual’s personal cancer-related and cancer treatment – related impairments, they will develop a targeted treatment program to address the impairments (307). For example, interdisciplinary rehabilitation interventions that include a prosthesis, gait training, and impairment-specific therapeutic exercise can benefit patients who have a limb amputated as part of treatment for osteosarcoma; and medications and speech-language therapy can benefit patients who have changes in short-term memory or concentration after cancer treatment.

As discussed in Treatment with Surgery, there is growing recognition that intervening before (prehabilitation) and during active cancer treatment can promote recovery and reduce the incidence and/or severity of the symptoms and adverse effects of the disease and its treatment (308). For example, in one study, prehabilitation with a speech – language pathologist for education, baseline assessment of swallowing, nutrition, and prophylactic oral motor exercises helped reduce posttreatment swallowing and swallowing-related impairments for patients with head and neck cancer (309). In another study, prehabilitation consisting of home-based, moderate-intensity exercise reduced anxiety and increased physical functioning before and after surgery for men preparing to undergo radical prostatectomy after a prostate cancer diagnosis (310). In addition, numerous aspects of prehabilitation, including preoperative exercise, can benefit patients with breast cancer (190, 311), such as Christine Cosby).
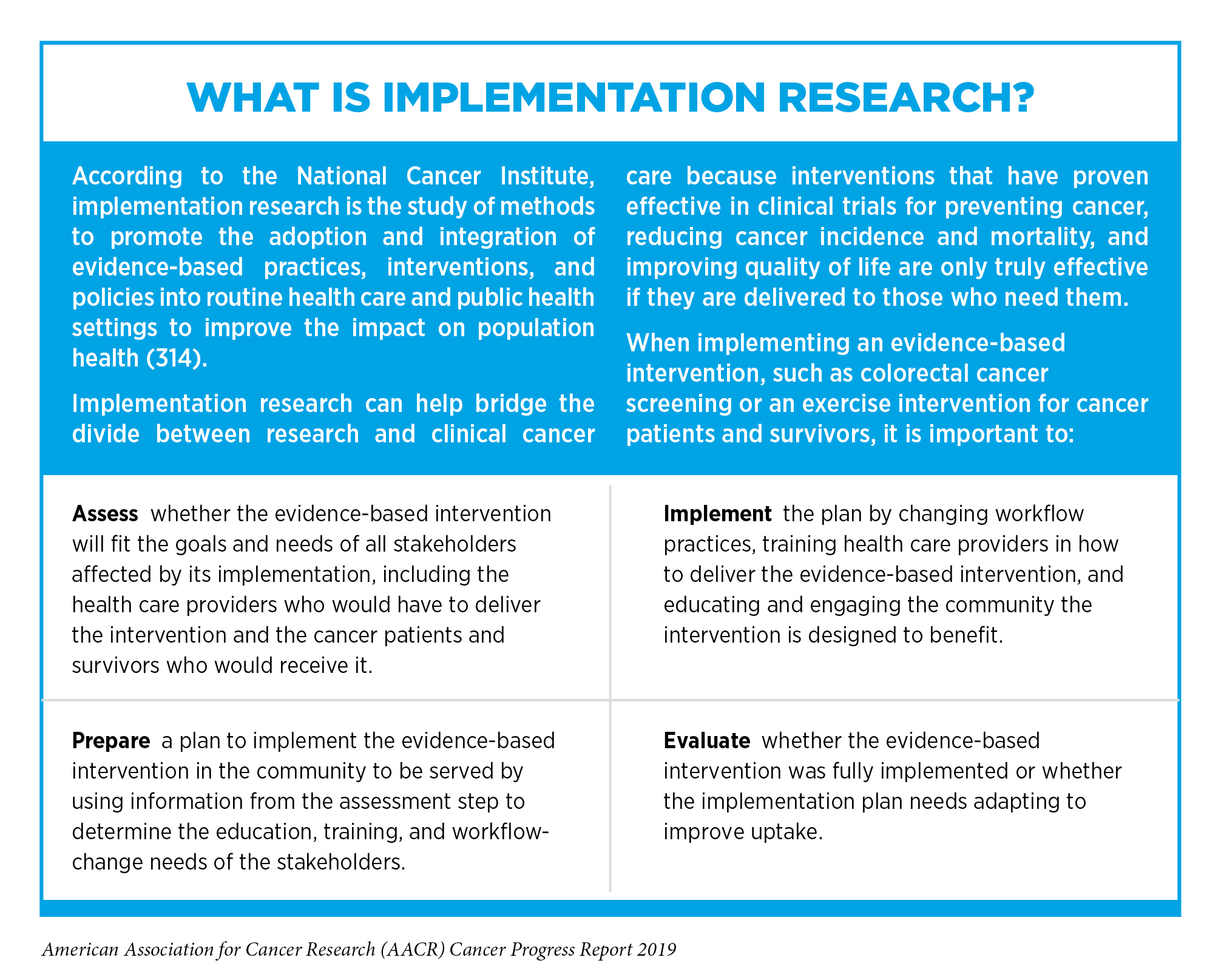
Despite the emerging evidence that prehabilitation, enhanced recovery programs, and rehabilitation can improve quality of life across the continuum of cancer care, one recent study showed that only 1 percent to 2 percent of cancer survivors receive rehabilitation for cancer-related and cancer treatment – related impairments (306). This highlights the need for all stakeholders committed to reducing the morbidity and mortality of cancer to come together to ensure the efficient and effective integration of cancer rehabilitation services into the care of cancer patients and survivors. One recent study showed that the implementation of a collaborative telerehabilitation program consisting of 6 months of centralized telerehabilitation provided by a physical therapist-physician team improved function and reduced pain for patients who had advanced cancer (312). The program also reduced the time patients spent in hospitals and in long-term care facilities. Despite the success of this program, identifying the best way to implement cancer rehabilitation into the continuum of cancer care remains an area of intensive investigation in the increasingly important area of implementation research (306) (see sidebar on What Is Implementation Research?).
Delivering Care to Cancer Survivors
As more and more people are surviving longer after a cancer diagnosis, it has become increasingly clear that the transition from initial cancer treatment to follow-up, long-term survivorship care can be complicated.
Coordinating Care
Most cancer survivors have poorer health and quality of life than other individuals of a similar age and are at increased risk for long-term morbidity and premature mortality as a result of their cancer diagnosis and treatment. Therefore, cancer survivors have complex health-care needs that are best met by a wide range of health care professionals.
Emerging evidence suggests that cancer survivors receive the highest level of care if their care is well coordinated, either by an oncologist and primary care provider or shared by multiple specialists (267), (314). Given that the follow-up cancer care needs of each survivor are unique, we need to identify the optimal way to provide comprehensive, coordinated, patient-centered care to all cancer survivors, rather than using a one-size-fits-all approach (315).
The Important Role of Caregivers
Caregivers provide an extension to a cancer survivor’s health care team, playing a vital role across the continuum of cancer care, from diagnosis through long-term survivorship. The population of caregivers is growing proportionally with the number of cancer survivors. One recent study of caregiving in 18 U.S. states led researchers to estimate that there are 1.1 million family caregivers of adults with cancer living in these states and that more than one in five of these people provided caregiving for more than 20 hours per week (316).
It is important to note that all caregivers are at risk for poor health outcomes, in particular, poor mental health outcomes (285). However, research shows that those who provide caregiving for longer hours experience worse outcomes (316). Such research is bringing increasing awareness to the need for new strategies to optimize and tailor support for caregivers.
